


When the International Study of Comparative Health Effectiveness With Medical and Invasive Approaches (ISCH-EMIA) trial1–3 was presented at the American Heart Association meeting in November, 2019, it generated multiple headlines in major news sources. CNN covered the story by saying, “For heart disease, meds may work as well as invasive surgery, major trial shows.”4 The Washington Post published a story entitled “Stents and bypass surgery are no more effective than drugs for stable heart disease, highly anticipated trial results show.”5
See related article, page 401
Neither these nor other similar headlines accurately convey the current body of evidence regarding the role of coronary revascularization in patients with coronary artery disease. The benefits of early revascularization in reducing mortality and reinfarction risk have been well established in patients who have unstable angina at rest, acute myocardial infarction, and significant unprotected left main coronary artery disease.6–9 However, since the publication of the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial10 in 2007, we have also known that patients with stable angina or ischemia do not experience a reduction in the risk of death, myocardial infarction, or cardiac arrest with percutaneous coronary intervention. Importantly though, percutaneous coronary intervention is associated with better relief of ischemic symptoms and quality of life than medical therapy alone.
Here, we describe the design, results, and limitations of the recent ISCHEMIA trial1–3 and how its findings confirm and expand our existing understanding of the role of coronary revascularization in patients with stable ischemic syndromes.
ISCHEMIA TRIAL DESIGN AND METHODOLOGY
The ISCHEMIA trial1–3 was a randomized trial that compared, in a 1-to-1 ratio, an initial invasive or conservative treatment strategy in 5,179 patients with stable coronary artery disease with moderate or severe ischemia by noninvasive stress testing.
The key exclusion criteria were:
Significant unprotected left main coronary artery disease (≥ 50% stenosis)
Estimated glomerular filtration rate less than 30 mL/min/1.73 m2
New York Heart Association class III or IV heart failure
Recent myocardial infarction, percutaneous coronary intervention, or coronary artery bypass grafting
Severe left ventricular dysfunction (ejection fraction < 35%)
Intolerable angina at baseline.
All patients received guideline-directed optimal medical therapy. Coronary computed tomography was performed to exclude left main disease unless the coronary anatomy was previously defined. Patients with renal dysfunction did not undergo coronary computed tomography. The invasive strategy group underwent coronary angiography followed by revascularization within 1 month after randomization.
The primary end point of the trial was a composite of cardiovascular death, nonfatal myocardial infarction, hospitalization for unstable angina, hospitalization for heart failure, or resuscitated cardiac arrest. The key secondary end points in North American participants were a composite of cardiovascular death and nonfatal myocardial infarction, angina, and measures of quality of life and health economics.
Concurrent studies were performed in patients with advanced chronic renal failure11 and nonobstructive coronary artery disease with inducible ischemia.
TRIAL RESULTS
It took over a decade for the trial investigators to enroll 8,518 patients after screening nearly 26,000 candidates.
Of these 8,518 patients, 3,339 were excluded for various reasons, eg:
1,350 did not have moderate or severe ischemia on stress testing
1,218 did not have obstructive coronary artery disease
434 had left main coronary artery disease.
Coronary computed tomography was performed in 73% of patients.
Most (77%) of the patients were men, and the median age was 64. About 40% had diabetes mellitus. Most (90%) had a history of stable angina, and 29% had progressive angina in the previous 3 months, while 34.3% had no angina in the previous 4 weeks. Moderate to severe ischemia was documented in 87%. Nearly everyone in the trial was receiving a statin and aspirin, nearly 60% had a low-density lipoprotein cholesterol level less than 70 mg/dL, and 77% had a systolic blood pressure lower than 140 mm Hg.
Among patients randomized to the invasive strategy, approximately 80% underwent revascularization, of whom 25% underwent surgical revascularization (using the internal mammary artery in 92%). Most of the per-cutaneous coronary interventions were performed using second-generation drug-eluting stents (n = 1,329).
In the conservative strategy group, 28% of the patients ultimately underwent cardiac catheterization and revascularization for suspected or confirmed events (13.8%), optimal medical therapy failure (3.9%), or nonadherence (8.1%).
In the invasive strategy group, conventional coronary angiography confirmed triple-vessel disease (≥ 50% stenosis on quantitative coronary angiography) in 39.6% of the patients. More than one-third of the patients had proximal left anterior descending lesions (≥ 50% stenosis on quantitative coronary angiography). Fractional flow reserve-guided revascularization was performed in 20.3% of the cases. More than 400 patients in the invasive-strategy group underwent no revascularization, as a large proportion (221) of them had nonobstructive coronary artery disease. Coronary anatomy was found to be unsuitable for revascularization in 111 patients, and 28 patients preferred not to undergo revascularization.
Outcomes
After a median follow-up of 3.2 years, the event rates in the invasive vs conservative strategy groups did not differ significantly for the primary outcome (hazard ratio [HR] 0.93, 95% confidence interval [CI] 0.80–1.08) or cardiovascular death or myocardial infarction (HR 0.90, 95% CI 0.77–1.06).
However, the rate of spontaneous myocardial infarction was lower in the invasive strategy group (HR 0.67, 95% CI 0.53–0.83), as was the rate of hospitalization for unstable angina (HR 0.50, 95% CI 0.27–90). The rate of periprocedural myocardial infarction was higher in the percutaneous coronary intervention group than in the medical therapy group (HR 2.98, 95% CI 1.87–4.74), although periprocedural myocardial infarctions have been shown to have less prognostic importance (unless associated with Q waves or creatine kinase-MB > 10 times the upper limit of normal) than spontaneous myocardial infarctions.12
This finding raises the intriguing possibility of the benefit of revascularization in reducing spontaneous myocardial infarctions beyond symptom improvement in this patient population. However, spontaneous myocardial infarction was not a prespecified end point and thus must be regarded as a hypothesis-generating result that requires further validation. Moreover, the greater incidence of spontaneous myocardial infarction did not affect overall mortality, at least over the median 3.2 years of follow-up. Long-term follow-up might shed more light on the impact of spontaneous myocardial infarction on mortality and whether the rates of myocardial infarction continue to diverge between the 2 treatment groups over time. It would also be interesting to see the characteristics of the spontaneous myocardial infarction in each cohort, especially if they were large or complicated.
Results in patients with chronic kidney disease
The ISCHEMIA-CKD trial11,13 assessed the same hypothesis as the ISCHEMIA trial in 777 patients with renal dysfunction (end-stage renal disease on dialysis or estimated glomerular filtration rate less than 30 mL/min/1.73 m2). The findings were similar to those of the ISCHEMIA trial, although the incidence of stroke was higher with the invasive strategy (HR 3.76, 95% CI 1.52–9.32), as was the rate of death or new dialysis (HR 1.48, 95% CI 1.04–2.11). Interestingly, the invasive approach was beneficial in individuals with severe inducible ischemia.
Quality of life
The burden associated with medical therapy and recurrent symptoms is not inconsequential. Frequent trips to outpatient clinics and emergency departments for recurrent symptoms and inability to participate in cardiac rehabilitation and exercise and weight-loss programs impair quality of life in patients with coronary artery disease.14 Multiple previous trials10,15 have shown improvement in quality of life after percutaneous coronary intervention in patients with stable angina.
In the ISCHEMIA trial,3 patients randomized to invasive therapy had significantly greater improvements in disease-specific health status (angina symptoms, functional status, and quality of life) than those in the conservative treatment group.
While differences in health status were only modest in the overall trial population, this was driven by the fact that 35% did not have angina at baseline, and 44% had angina only 1 to 3 times per month. A minority of the trial population, only 20%, were severely symptomatic with daily or weekly angina. Not surprisingly, patients who were asymptomatic or minimally symptomatic at baseline had little or no change in symptom status over follow-up. In contrast, patients with moderate to severe symptoms at baseline had substantial improvements in angina frequency and quality of life with revascularization compared with conservative management, benefits that were sustained over the 36-month observation period. Similar findings were observed in the ISCHEMIA-CKD trial.3,16
LIMITATIONS OF THE ISCHEMIA TRIAL
Due to slow recruitment and lower-than-expected event rates, the primary end point was changed from cardiovascular death or nonfatal myocardial infarction to a composite of cardiovascular death, nonfatal myocardial infarction, hospitalization for unstable angina, hospitalization for heart failure, or resuscitated cardiac arrest. Although this modification was a prespecified contingency and was enacted before the trial was unblinded, it raises questions regarding whether additional end points like resuscitated cardiac arrest or heart failure are relevant to percutaneous coronary intervention in stable coronary artery disease.
More relevant to the interpretability of the trial was that patients with lower ischemia burden (5%) and abnormal exercise tolerance testing were included to increase enrollment, potentially diluting the results of the trial. Nearly 13% of the invasive strategy group had nonobstructive coronary artery disease and did not require revascularization.
Moreover, as noted in the discussion above on quality of life, only a small proportion of patients were severely symptomatic with the potential to experience substantial improvements in quality of life and angina frequency.
Finally, the impact of complete revascularization, mode of revascularization, and invasive functional assessment are yet to be explored in the ISCHEMIA trial.
INVASIVE PHYSIOLOGY ASSESSMENT IN STABLE CORONARY ARTERY DISEASE
Findings from trials using the instantaneous wave-free ratio (IFR),17,18 or fractional flow reserve (FFR)19–21 have suggested that these functional measurements of hemodynamic significance may help identify patients for whom revascularization is best suited.
FAME 2. The Fractional Flow Reserve Versus Angiography for Multivessel Evaluation 2 (FAME 2) randomized trial15 found that in patients with stable angina and FFR 0.80 or less, percutaneous coronary intervention reduced the rate of death, nonfatal myocardial infarction, and urgent revascularization at 5 years compared with medical therapy, a benefit driven by a reduction in the rate of urgent re-vascularization. Patients deferred for revascularization based on a nonsignificant FFR value of more than 0.80 had a good long-term prognosis.
Similar to the ISCHEMIA trial findings, the FAME 2 trial15 also demonstrated a trend in which percutaneous coronary intervention was associated with a nearly significant reduction in myocardial infarction at 5 years (HR 0.66, 95% CI 0.43–1.00) compared with medical therapy.
The RIPCORD trial (Does Routine Pressure Wire Assessment Influence Management Strategy at Coronary Angiography for Diagnosis of Chest Pain?)22 evaluated the routine use of pressure wire assessment during coronary angiography and demonstrated a drastic difference in decision-making before and after pressure wire assessment.
This finding provided the hypothesis for the RIPCORD 2 trial,23 which will evaluate all patients undergoing catheterization for elective indications and urgent stabilized non-ST-elevation acute coronary syndromes with a routine pressure wire. The primary out come measures are economic and quality of life. This trial will shed more light on FFR-guided angiography and steer further trials in this arena targeting hard end points.
ONE SIZE DOES NOT FIT ALL
The population of the ISCHEMIA trial1–3 was heterogeneous and included patients with or without symptoms, assessed with various imaging tests proving ischemia. Importantly, the trial excluded patients with intolerable angina. The results were consistent with those of previous trials, and percutaneous coronary intervention had no survival benefit in patients with stable coronary artery disease without severe left main disease.
Importantly, however, revascularization did improve quality of life and reduce angina frequency in moderately or severely symptomatic patients. Moreover, rates of spontaneous myocardial infarction and hospitalizations for unstable angina were lower in the invasive treatment group. Based on the trial findings, tools can be developed that would predict the possible advantages and disadvantages of each management strategy in individual patients.
The ISCHEMIA trial1–3 does not change the indication for revascularization in stable coronary artery disease that has been established so far. Revascularization should be reserved to treat individuals with refractory angina and moderate to severe ischemia to improve the quality of life. The ISCHEMIA trial1–3 results do not apply to patients with significant unprotected left main disease, ischemic cardiomyopathy, or acute coronary syndromes.
Figure 1 is a suggested algorithm for managing patients with stable angina. The ISCH-EMIA trial provides added reassurance that patients without symptoms with an abnormal stress test can be treated noninvasively once left main disease is excluded.
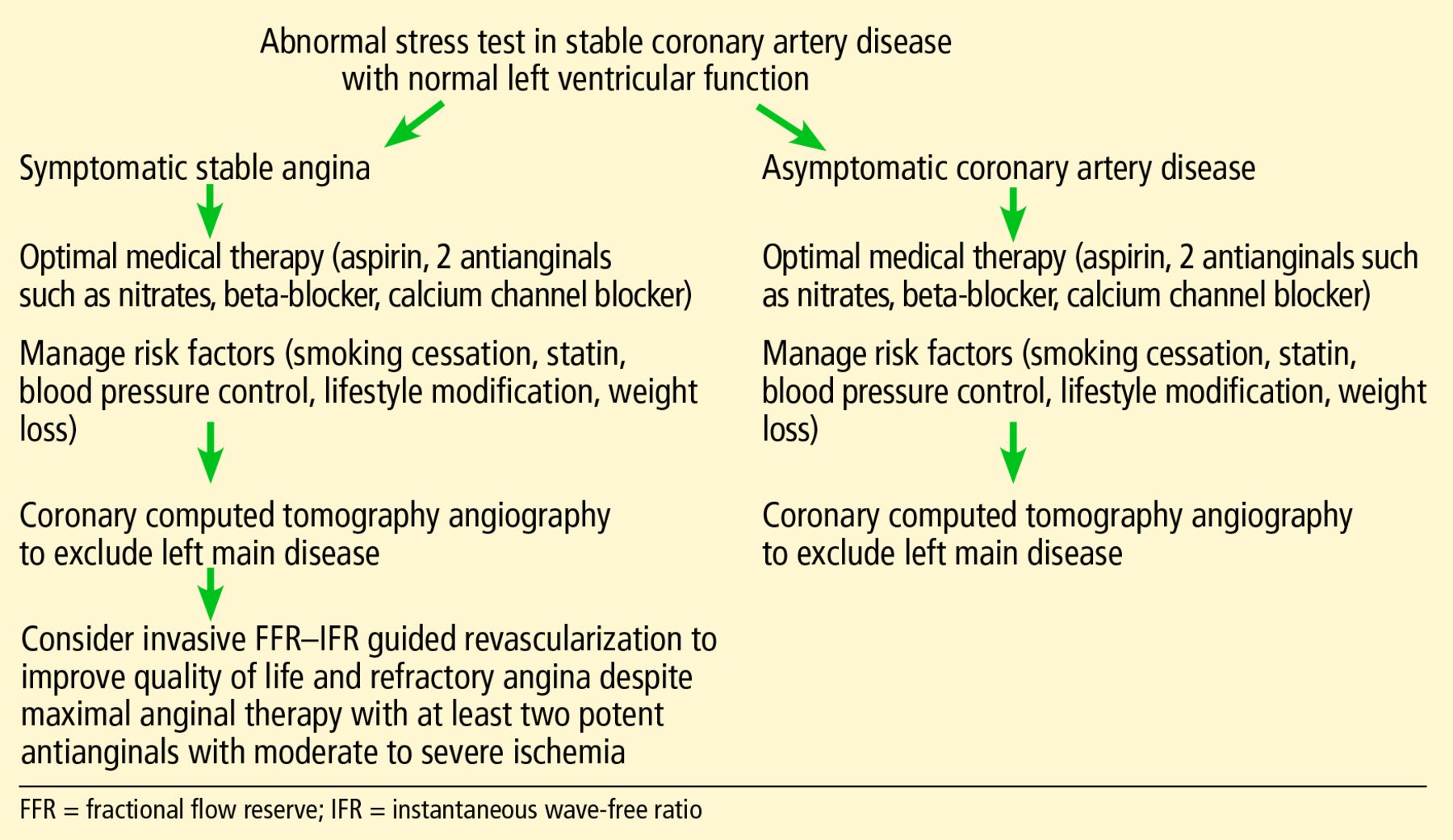
Algorithm for management of stable coronary artery disease.
Stable coronary artery disease needs a patient-centered approach, and one size does not fit all. Management should take into consideration the clinical history, impact on quality of life, risk factors, and the burden of ischemia. A multidisciplinary approach and up-front, frank discussion is necessary regarding an invasive strategy, contemplating the risk and benefits.
The ISCHEMIA trial indicates that patients who have stable coronary artery disease, an abnormal stress test, and no left main disease can be medically managed safely without invasive treatment.
Cardiac computed tomography is useful to exclude left main disease.
The ISCHEMIA trial results are relevant to stable coronary artery disease and do not apply to significant unprotected left main disease, ischemic cardiomyopathy, and acute coronary syndromes.
Interestingly, rates of spontaneous myocardial infarction and hospitalizations for unstable angina were lower in the invasive treatment group than in the conservative management group. However, further research is necessary to confirm this finding at a large scale.
Revascularization continues to be beneficial in patients with refractory angina and moderate to severe ischemia to improve the quality of life.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}