


ABSTRACT
Glucocorticoids cause significant bone loss, predominantly affecting trabecular bone, with consequent fragility fractures. The risk of fractures is related to the dose and duration of glucocorticoid use, but an increased risk may be observed even at low doses and even in the first month of treatment. Steps to prevent or treat osteoporosis should be considered in all patients who take the equivalent of prednisone at a dose of 2.5 mg or more per day for 3 or more months.
The Fracture Risk Assessment tool (FRAX) includes a yes-or-no question about glucocorticoid use, but the formula is based on a medium dose, and the FRAX score should be adjusted upward in patients on high doses and downward in patients on lower doses.
Lifestyle modifications and optimization of calcium and vitamin D intake are recommended for all patients on long-term glucocorticoid therapy.
Bisphosphonates are the first-line drugs for patients at moderate or high fracture risk, based on proven efficacy, safety, and low cost.
Zoledronate (intravenous), teriparatide, and denosumab are second-line options for patients at high risk of fracture on glucocorticoids who cannot tolerate oral bisphosphonates.
Glucocorticoids are associated with a variety of adverse effects including osteoporosis, with fractures occurring in as many as 50% of long-term users.1 A meta-analysis2 has shown strong correlations between cumulative dose and loss of bone mineral density, and between daily dose and risk of fracture. The relative risk of fracture is significantly increased even with daily doses as low as 2.5 mg of prednisolone,3 and depends on duration of therapy; daily oral prednisone therapy for 3 to 6 months or more has been shown to increase the risk of bone loss in most studies.4,5 After glucocorticoids are discontinued, the fracture risk gradually decreases to baseline but may be only partially reversible.4,5 The problem affects a great many people, as these drugs are used to treat a variety of inflammatory diseases, and the estimated prevalence of oral use is more than 1% in the United States and United Kingdom.6–8
In 2017, the American College of Rheumatology (ACR) published guidelines for preventing and treating glucocorticoid-induced osteoporosis, with recommendations and algorithms for assessing and categorizing fracture risk, both initially and on follow-up.9 This review summarizes the 2017 ACR recommendations, as well as advances in treatment since then.
HOW GLUCOCORTICOIDS DAMAGE BONE
Bone loss in patients taking glucocorticoids has 2 phases, with rapid loss in the first several months to 1 year followed by a further slower and progressive decline.10 The loss is predominantly from trabecular bone, with marked changes in the lumbar spine, but the femoral neck and other sites are also affected.2 Even at relatively low doses, such as prednisone 2.5 mg daily, glucocorticoids have been shown to cause more than an 8% decrease in trabecular bone mineral density after just 20 weeks of therapy.11
Glucocorticoids damage bone though several mechanisms:
By increasing bone resorption. Initial bone loss is caused by increased bone resorption resulting from upregulation of RANK ligand and suppression of osteoprotegerin.12,13 Further, glucocorticoids inhibit gonadotropin secretion, so that serum levels of androgen and estrogen are lower, also causing bone resorption. They also decrease calcium absorption in the intestines, antagonize vitamin D, and decrease renal calcium reabsorption, all resulting in a secondary hyperparathyroid state.14
By decreasing bone formation. In cell cultures, glucocorticoids at high doses decrease bone formation by inhibiting osteoblast proliferation, increasing rates of apoptosis of osteoblasts.15 They also have been shown to suppress Wnt gene expression in a dose-dependent manner, which in turn suppresses osteogenesis.
By decreasing bone vascularization, likely by reducing production of vascular endothelial growth factor by osteoblasts, creating areas of necrosis.16 That may explain why reduction in bone strength is greater than that due to reduced bone mass alone.17
RISK FACTORS AND FRAX
Other risk factors can contribute to bone loss in patients taking glucocorticoids. Nonmodifiable risk factors include advanced age, white race, female sex, early menopause, low weight or body mass index, previous fragility fracture, history of rheumatoid arthritis, and a family history of hip fragility fracture. Modifiable risk factors include low calcium or vitamin D intake, estrogen deficiency, immobility, cigarette smoking, and excessive alcohol or caffeine intake. Other comorbid disorders contributing to bone loss must also be taken into account.18
The fracture risk calculation
Released in 2008 by the World Health Organization, the Fracture Risk Assessment Tool (FRAX; https://www.sheffield.ac.uk/FRAX/index.aspx) has been validated and is commonly used in clinical practice. It calculates the 10-year probability of a major fracture of the spine, forearm, hip, or shoulder, and the 10-year probability of a hip fracture. The FRAX models were developed from population-based cohorts from different countries of the world and are further subcategorized by race. It requires the following information:
Age or date of birth
Sex
Weight
Height
Bone mineral density of the femoral neck (optional, but recommended for greater accuracy19).
Yes-or-no answers are required for:
Previous fragility fracture
Hip fracture in a parent
Smoking status
Glucocorticoid use (prednisolone ≥ 5 mg/day or the equivalent, for > 3 months)
Diagnosis of rheumatoid arthritis
Alcohol intake of 3 units per day or more
Disorders associated with secondary osteoporosis–eg, type 1 diabetes, osteogenesis imperfecta in adults, untreated long-standing hyperthyroidism, hypogonadism or early menopause (before age 45), chronic malnutrition or malabsorption, and chronic liver disease.
FRAX risk adjustment for glucocorticoid dose
The FRAX score for a patient using glucocorticoids is based on a medium dose. Hence, it may underestimate the actual fracture risk in people on higher doses and overestimate the risk in people on lower doses.
Kanis et al20 devised a simple FRAX adjustment (Table 1) based on glucocorticoid dose and age. For example, for those receiving higher doses of glucocorticoids (prednisolone ≥ 7.5 mg/day or equivalent), the adjusted risk of major osteoporotic fracture is 15% higher in the 60-to-70 age group and 20% higher in the 40-to-50 age group compared with unadjusted risk. The FRAX score can also be adjusted without regard for age, as follows:
Adjustment in FRAX score by glucocorticoid dose and age
In patients on medium doses (eg, prednisolone 2.5 to 7.5 mg/day) no adjustment to the FRAX risk is needed.
In patients on low doses (eg, prednisolone < 2.5 mg/day), multiply the unadjusted FRAX risk of a major osteoporotic fracture by 0.80, and multiply the unadjusted risk of a hip fracture by 0.65.
In patients on high doses (eg, prednisolone ≥ 7.5 mg/day), multiply the unadjusted FRAX risk of major osteoporotic fractures by 1.15, and multiply the unadjusted FRAX risk of hip fractures by 1.20.
Example. A 66-year-old woman with rheumatoid arthritis has been taking prednisone 10 mg for 4 months and is expected to continue this dose. According to the unadjusted FRAX score, her 10-year hip fracture risk is 0.9%. This should be multiplied by 1.2 (a 20% increase), yielding an adjusted FRAX score of 1.08%. The adjustment for glucocorticoid dose suggests that this patient should be treated, as her 10-year risk of hip fracture is now higher than 1% (moderate risk).
FRAX caveats
FRAX cannot be used to estimate the risk of fracture in patients younger than 40. Moreover, FRAX results are partly based on hip bone mineral density (if available), while glucocorticoid use results in more significant loss from the spine (trabecular bone) than from the hip, so the FRAX score may underestimate the true fracture probability.19
For patients with discordant bone mineral density in the hip vs the lower spine, the Foundation for Osteoporosis Research and Education’s 10-year risk calculator can be used (https://riskcalculator.fore.org/).
FRACTURE RISK CATEGORIES
The ACR9 stratifies the risk of fracture in glucocorticoid users into 3 categories:
Low fracture risk
Patients age 40 and older with adjusted FRAX risk of less than 10% for major osteoporotic fracture or less than 1% for hip fracture
Patients under age 40 who do not have risk factors other than glucocorticoid exposure.
Moderate fracture risk
Patients age 40 and older whose adjusted FRAX risk of major osteoporotic fracture is 10% to 19%, and whose risk of hip fracture is 1% to 3%
Patients under age 40 on glucocorticoids taking 7.5 mg or more daily for at least 6 months, and either hip or spine bone mineral density Z score below –3, or rapid bone loss of at least 10% at the hip or spine over 1 year.
High fracture risk
Patients of any age with a history of osteoporotic fracture
Patients age 40 and older whose T score (hip or spine) is –2.5 or lower (in men age 50 and older, and in postmenopausal women)
Patients with adjusted FRAX risk 20% or higher for major osteoporotic fracture or 3% or higher for hip fracture.
Adults age 30 and older on a very high dose of glucocorticoids (eg, prednisone ≥ 30 mg daily and > 5-g cumulative dose over the past year) are included in the moderate-to-high-risk group for treatment.
INITIAL RISK ASSESSMENT
The initial fracture risk assessment for an adult includes a detailed history reviewing the risk factors for osteoporosis and details of glucocorticoid use including dosages, frequency, and duration. Modifiable, nonmodifiable, and secondary causes of osteoporosis should be reviewed as appropriate, including fall risk.
Physical examination should include weight, height (looking for a decrease), and thorough evaluation of limbs and spine, checking for signs of fracture (bony deformities, spinal tenderness, and kyphosis).
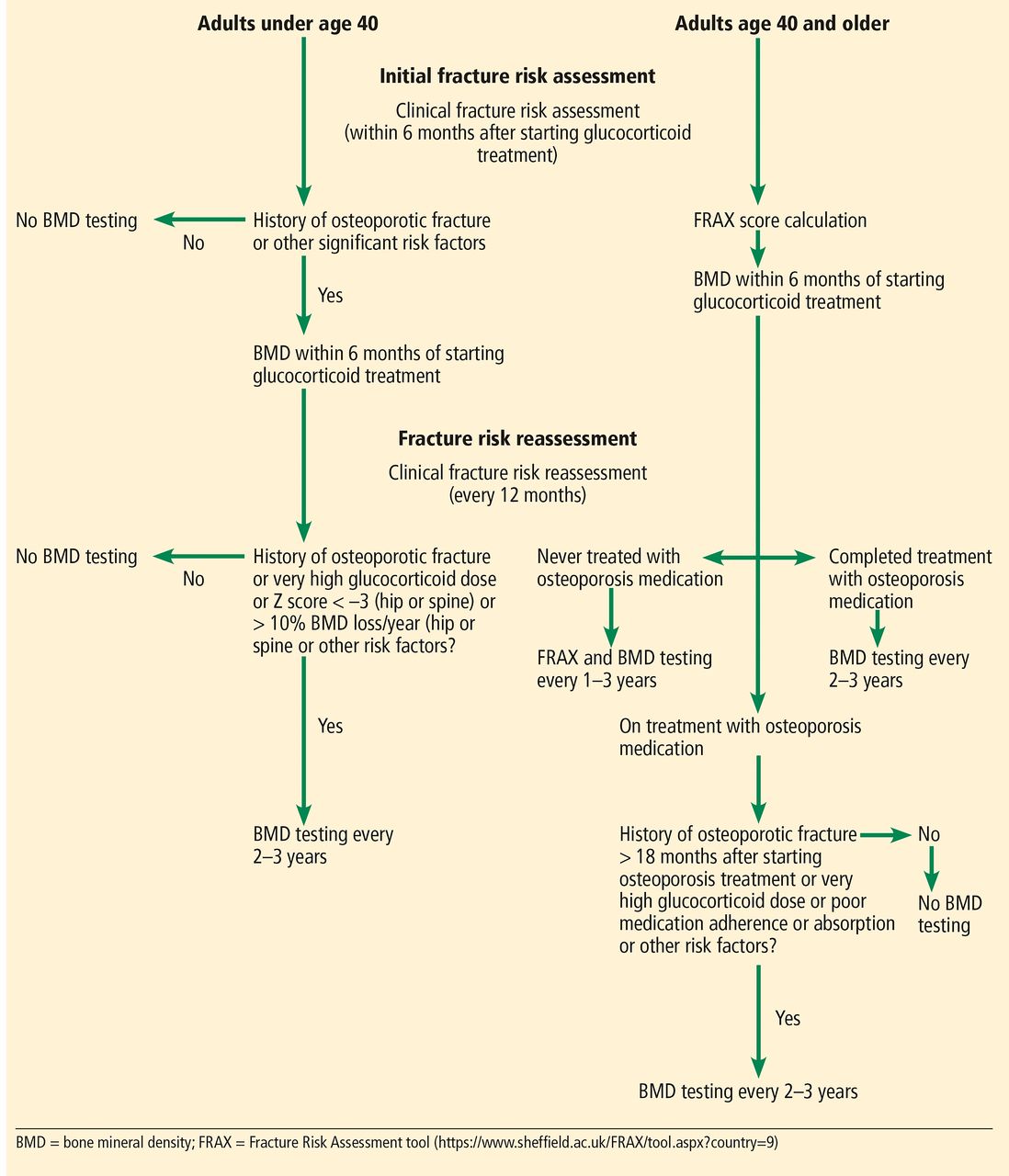
The initial evaluation should be done as soon as possible, but preferably within 6 months after starting glucocorticoid treatment (Figure 1).9

An algorithm for initial fracture risk assessment and reassessment in adult patients, based on current guidelines.
Adapted from information in reference 9.
For adults younger than 40, bone mineral density should be measured as soon as possible or within 6 months after starting glucocorticoids if they are at high fracture risk (due to prior osteoporotic fractures) or have other significant osteoporotic risk factors.
For adults 40 and older, the FRAX score should be calculated as soon as possible or within 6 months after starting glucocorticoids and should include the bone mineral density if this testing is available.
REASSESSING FRACTURE RISK
Every year, a comprehensive evaluation including fracture risk assessment should be completed for patients on glucocorticoids to determine how frequently the bone mineral density needs to be tested (Figure 1)9:
Adults younger than 40 should undergo bone mineral density testing every 2 to 3 years if any of the following features are present:
High fracture risk (prior osteoporotic fractures)
High-dose glucocorticoids (eg, prednisone 30 mg or more daily, and cumulative dose 5 g per year)
Bone mineral density Z score –3 or less (hip or spine)
Bone mineral density loss from the hip or spine 10% or more per year, or other significant osteoporotic risk factors.
Adults age 40 and older should be reevaluated based on treatment status. Those on glucocorticoids who have never started osteoporosis treatment (except for vitamin D and calcium) should have their FRAX score calculated, with bone mineral density testing if possible, every 1 to 3 years. Those on glucocorticoids who have completed osteoporosis treatment, or on glucocorticoids and currently on osteoporosis treatment with risk factors for higher fracture risk (including fracture that occurs after 18 months of treatment), should undergo bone mineral density testing every 2 to 3 years.
Additionally, adults age 40 and older should undergo more frequent bone mineral density testing if on high initial doses (eg, prednisone ≥ 30 mg daily and cumulative dose of 5 g per year) or if at high fracture risk due to prior osteoporotic fracture. Bone mineral density testing can be done closer to every 3 years for patients on lower doses of glucocorticoids and without any other osteoporotic risk factors or who have higher bone mineral densities.
RECOMMENDATIONS FOR TREATMENT
The ACR9 made its 2017 recommendations after rating the evidence of benefit vs harm for the different treatment options and thoroughly reviewing the literature, after which an expert panel of rheumatologists and internists reached a decision by consensus. Most of the recommendations were conditional, owing to uncertain evidence.
For all: Lifestyle, calcium, and vitamin D
All adults taking the equivalent of prednisone 2.5 mg or more daily for 3 or more months should incorporate lifestyle changes to optimize their bone density, eg, follow a healthy diet, maintain a normal weight (body mass index), stop smoking, limit alcohol intake to less than 3 units/day, engage in low-impact weight-bearing exercises, and take measures to prevent falls.
In addition, these patients should optimize their calcium and vitamin D intake.9 Vitamin D helps increase osteoblastogenesis and intestinal absorption of calcium, and glucocorticoids counteract this.21 A meta-analysis disclosed that vitamin D and calcium supplementation prevented bone loss at the lumbar spine and forearm in glucocorticoid-treated patients; the effect was modest but clinically and statistically significant.22 The recommended daily vitamin D intake is about 600 to 800 international units, with a serum level 20 ng/mL or higher as the goal. Calcium intake, preferably through diet, should be in the range of 1,000 to 1,200 mg daily.
The recommendations for lifestyle, calcium intake, and vitamin D intake are conditional due to indirect and low-quality evidence in glucocorticoid users.
PHARMACOLOGIC TREATMENT
The guidelines9 recommended pharmacologic treatment in addition to the above measures in patients at moderate or high risk of fractures, including patients of any age who have had a previous osteoporotic fracture.
An oral bisphosphonate is the first choice, intravenous bisphosphonate the second choice, teriparatide the third choice, and denosumab the fourth (Table 2). This ranking was based on the opinions of the ACR guideline voting panel. The panel recommended oral bisphosphonates as a first choice and parenteral bisphosphonates as a second choice after comparing data about absolute fracture reduction, harms (toxicity and inconvenience of daily injections), and costs (Table 3). A purely evidence-based ranking was not possible since the number of comparative studies was small.
Treatment based on age and fracture risk
Considerations regarding osteoporosis medications
Bisphosphonates
A Cochrane review of 27 randomized controlled trials23 found high-quality evidence that bisphosphonates reduce the risk of vertebral fractures in glucocorticoid-induced osteoporosis, with data extending to 24 months of use, and prevent bone loss at both the lumbar spine and femoral neck. The effect of glucocorticoids on nonvertebral fractures was minimal to none.
Alendronate has been shown to increase bone mineral density in both the lumbar spine and hip in patients taking glucocorticoids and also to reduce the rate of new vertebral fractures.24–27
Risedronate similarly was shown in a randomized, placebo-controlled trial to significantly increase bone mineral density.28
Intravenous bisphosphonates (eg, zoledronic acid, pamidronate) have also been shown to significantly reduce the rates of non-vertebral fractures, vertebral fractures, and hip fractures.
A meta-analysis of 8 randomized, placebo-controlled trials involving 13,335 patients showed that treatment with zoledronic acid significantly reduced the incidences of non-vertebral fractures, vertebral fractures, and hip fractures. Zoledronic acid was also associated with significant improvement in bone mineral density in the lumbar spine, total hip, femoral neck, and trochanter.29 However, the incidence of any adverse event was higher in the zoledronic acid group than in the control group.
A randomized controlled trial30 showed that intravenous zoledronic acid was superior to risedronate in increasing the bone mineral density of the lumbar spine for both treatment and prevention of osteoporosis.
Oral bisphosphonates are cost-effective and considered first-line agents for glucocorticoid-induced osteoporosis. However, intravenous zoledronic acid is superior to oral bisphosphonates and may be preferable in certain patient groups if better compliance is required or fracture risk is high.8
Teriparatide
Teriparatide is a synthetic analogue of parathyroid hormone that activates the Wnt/beta-catenin pathway in osteoblasts, thereby increasing bone formation. Since inhibition of bone formation is a key mechanism in glucocorticoid-induced osteoporosis, anabolic agents such as teriparatide may be pivotal in its treatment.
Compared with alendronate in treating glucocorticoid-induced osteoporosis in a 36-month randomized controlled trial,31 teriparatide was associated with greater increases in bone mineral density in the spine, hip, and femoral neck and with fewer new vertebral fractures. Also, a meta-analysis in 2016 showed teriparatide was efficacious in preventing vertebral fractures in glucocorticoid users.32
Despite data that teriparatide reduces the risk of radiographic vertebral fractures more than bisphosphonates do, the 2017 ACR guidelines9 recommended it as a second option after bisphosphonates, in view of its higher cost and its inconvenient route of administration (daily injections).33 However, we recommend that it be considered as a first-line option in patients who have at least one grade 2 or higher (on a scale of 1 to 4) vertebral fracture, based on literature review.
Bone is rapidly lost after teriparatide is discontinued, so an antiresorptive agent should be started soon thereafter if appropriate.25
Denosumab
Denosumab is a fully humanized monoclonal antibody against RANK ligand with a potent antiresorptive effect, resulting in higher bone mineral density at the lumbar spine and total hip and lower risk of new fractures in patients on glucocorticoids.34
The safety and efficacy of denosumab in treating glucocorticoid-induced osteoporosis were evaluated in the 12-month primary analysis of a 2-year, randomized, multicenter, double-blind, parallel-group, active-controlled study in 795 patients.35 Patients received either oral risedronate 5 mg daily or denosumab 60 mg subcutaneously every 6 months for 1 year. Denosumab was noninferior (the primary outcome) and superior (a secondary outcome) to risedronate at 1 year in its effect on lumbar bone mineral density in patients who had been on glucocorticoids for at least 3 months or even less than 3 months. Given these findings, denosumab can be used in patients in whom bisphosphonates are contraindicated.
A post hoc analysis revealed that the vertebral fracture rate increased to the level seen in the untreated population after denosumab was discontinued, which needs to be kept in mind when choosing this treatment.36
The US Food and Drug Administration has approved denosumab for treating gluco-corticoid-induced osteoporosis in men and women at high risk of fractures who are either initiating or continuing glucocorticoids in a daily dosage equivalent to 7.5 mg or more of prednisone and are expected to remain on them for at least 6 months. (This approval came after the ACR guidelines were written.)
TREATMENT IN SPECIAL POPULATIONS
The ACR guidelines included recommendations for initial treatment in special populations.9
Women
In women at moderate to high risk who have childbearing potential, treatment is recommended for those who do not plan on becoming pregnant while receiving osteoporosis medication and are either sexually inactive or using birth control.
Treat with an oral bisphosphonate rather than calcium and vitamin D alone
Second-line therapy is teriparatide
For patients at high risk for whom oral bisphosphonates and teriparatide are not appropriate, consider intravenous bisphosphonates or denosumab (in that order of preference), but consider the potential fetal risks with both options.
These recommendations are conditional, based on low-quality evidence. They have been extrapolated from other treatment groups.
In women who are pregnant:
Optimize calcium, vitamin D, and lifestyle modifications
No other osteoporosis medications are recommended in this group, given the lack of safety data.
Young patients
In adults age 30 or older receiving high-dose glucocorticoids (eg, initial dose of prednisone 30 mg per day or higher and cumulative dose higher than 5 g in 1 year):
Treat with an oral bisphosphonate rather than calcium and vitamin D alone
Treat with an oral bisphosphonate rather than an intravenous bisphosphonate, teriparatide, or denosumab
If bisphosphonates are not appropriate, other treatments are available (Table 2). These recommendations are conditional.
Organ transplant recipients
For adults with organ transplants who are treated with glucocorticoids, treatment is the same as for everyone else (Table 2) if the glomerular filtration rate is at least 30 mL/minute and there is no evidence of metabolic bone disease. Renal transplant patients should be evaluated by a metabolic bone disease expert.
The ACR and others9,37 did not recommend denosumab in transplant patients due to lack of safety data when used along with other immunosuppressive medications. However, in a study in 63 organ transplant recipients (15 diabetic patients who received simultaneous kidney and pancreas transplants, 34 patients who received kidney transplants, and 14 patients with liver grafts), denosumab was well tolerated (without serious adverse effects or infections). It improved bone mineral density in the lumbar spine and proximal femur, proving to be a successful option for transplant patients.38
FOLLOW-UP TREATMENT RECOMMENDATIONS
No studies have evaluated the duration of osteoporosis treatment in glucocorticoid-induced osteoporosis. The 2017 ACR guidelines, however, have provided some framework for treatment duration.
In adults age 40 and older taking an oral bisphosphonate, switching the therapy is conditionally recommended if a fracture is sustained after at least 18 months of treatment or if bone mineral density loss is greater than 10% per year. If the treatment failure is from poor absorption or adherence, then intravenous bisphosphonates should be considered.
For adults age 40 and older who have completed 5 years of oral bisphosphonate treatment and are at moderate or high risk of fracture, treatment can be:
Continued
Switched to an intravenous bisphosphonate if there is an absorption or adherence problem
Switched to another class of medication.
Adults age 40 and older on osteoporosis medication, calcium, and vitamin D whose glucocorticoid treatment is stopped and at low risk should discontinue the medication. However, calcium and vitamin D should be continued. These recommendations are conditional.
Adults age 40 and older on osteoporosis medication, calcium, and vitamin D whose glucocorticoid treatment has stopped and at moderate or high risk should complete the osteoporosis medication treatment. This recommendation is conditional for moderate-risk patients but strong for high-risk patients.
SUMMING UP
Glucocorticoid-induced osteoporosis is a major cause of bone loss and consequent fragility fractures. Despite high risk of fractures and comprehensive recommendations for treatment, most patients on glucocorticoids are not treated for it.
In addition to lifestyle modifications, pharmacologic treatment is recommended in both men and women taking glucocorticoids based on dose and duration of use. The first-line agents continue to be oral bisphosphonates. Intravenous bisphosphonates, teriparatide, and denosumab are recommended for patients with high risk for fractures or unable to tolerate oral bisphosphonates.
Footnotes
Dr. Magrey has disclosed board membership and consulting for Eli Lilly and board membership, consulting, teaching, and speaking for Novartis.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.