


A 58-year-old man presented with difficulty in moving his left hand. Three weeks before this presentation, he had symptoms of an upper respiratory tract infection, which resolved spontaneously in several days. And 1 week after that, he experienced a severe stabbing pain in his entire left upper arm, which resolved in several days. At that time, he also developed difficulty in moving the thumb and index finger of his left hand.
On physical examination, manual muscle testing showed weakness in the left opponens pollicis muscle and flexor digitorum profundus muscle of the left index finger, without apparent atrophy. There was no evidence of sensory disturbance. Tendon reflexes were normal in the upper and lower extremities, and pathological reflexes were negative.
The OK sign test was positive in the left hand (Figure 1). Blood tests, cervical magnetic resonance imaging, electromyography, and nerve conduction velocity testing showed no abnormal findings. Based on the history, symptoms, OK sign test, and lack of abnormalities on other parts of the workup, the patient was diagnosed with Parsonage-Turner syndrome.
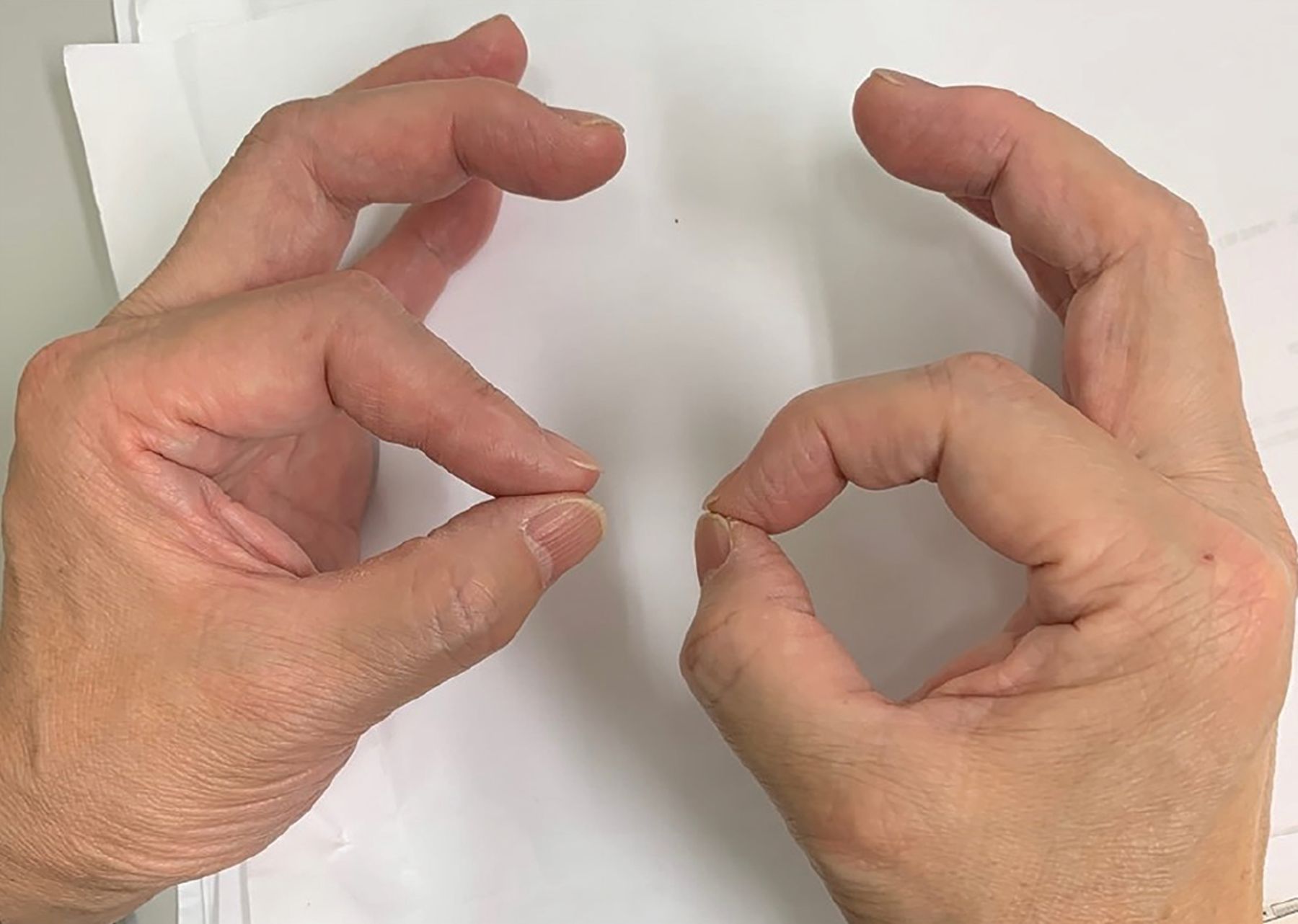
The OK sign test was positive in the left hand, with reduced flexion in the first interphalangeal joint and the second distal interphalangeal joint, as compared with the corresponding joints of the nonaffected (right) hand.
His symptoms resolved in several months after rehabilitation with physical therapy.
PARSONAGE-TURNER SYNDROME: DISTINGUISHING FEATURES
Parsonage-Turner syndrome, also referred to as idiopathic brachial plexopathy or neuralgic amyotrophy, is characterized by an acute onset of unilateral neuralgia of the upper extremity.1 The neuralgia resolves in several days to 2 weeks.1 Thereafter, muscle atrophy and motor paralysis develop in the ipsilateral side.1 The most commonly affected muscles are proximal ones, including the supraspinatus, infraspinatus, anterior serratus, deltoid, and biceps brachii.2 Cases of selective anterior-posterior interosseous nerve palsy have also been reported.3
The anterior interosseus nerve is a branch of the median nerve, which supplies motor innervation to the anterior forearm flexors, the thenar muscles, and the lateral 2 lumbricals. It also supplies sensory innervation to the lateral palm and anterior lateral 3 and one-half fingers. Both proximal median nerve palsy above the elbow and carpal tunnel syndrome result in reduced sensation in the thumb, index finger, and middle finger. Anterior interosseus nerve palsy alone does not cause sensory disturbance.
Akane et al4 reported that 27 of 51 (52.9%) patients with anterior-posterior interosseous nerve palsy had preceding upper extremity pain, and 9 of the 27 (33.3%) had pain in the entire arm. In the cases that began with pain, the first signs of weakness appeared within 7 days in 66.6%. A preceding infection was observed in 3 cases.
The OK sign test is administered by asking patients to make an OK sign with the thumb and index finger. It is positive if it detects reduced flexion in the first interphalangeal joint and the second distal interphalangeal joint, as compared with the corresponding joints of the nonaffected hand, and thus is useful in the diagnosis of anterior interosseous nerve palsy.5
Electromyography usually indicates acute denervation and axonal degeneration with potential positive fibrillation spike waves.6 However, 3.7% of patients with Parsonage-Turner syndrome show no abnormalities on electromyography2 because the alterations are generally not perceptible until 3 weeks after the onset of symptoms.6 Some cases also reported no abnormalities on magnetic resonance imaging or nerve conduction velocity testing.4 As patients with interosseous nerve palsy often lack characteristic imaging findings, careful history-taking is important in the diagnosis.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2021 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.