


Wheezing is a common symptom often associated with airway obstructive diseases such as asthma and chronic obstructive pulmonary disease (COPD). Dr. Chevalier Jackson, a prominent otolaryngologist of the late 19th and early 20th century, is credited with the aphorism, “All that wheezes is not asthma.”1 However, all that wheezes is obstruction of one kind or another.
See related article, page 147
In this issue of CCJM, Patel and Madan2 describe a patient with shortness of breath and wheezing who was ultimately found to have a tracheal web causing her symptoms. Here, we offer additional comments on this patient’s course, including historic features of the case, utility of the physical examination, and the value of pulmonary function testing.
HISTORIC FEATURES OF THE CASE
Patel and Madan’s patient was a 53-year-old woman, a nonsmoker, with shortness of breath of 3 years’ duration who had been diagnosed first with asthma and then with COPD. She had been hospitalized twice for presumed asthma exacerbations, without response to systemic steroids and antibiotics. Spirometry demonstrated severe obstruction that did not respond to a bronchodilator and normal lung volumes that showed no evidence of hyperinflation or air trapping. After reevaluation by a pulmonologist, the diagnostic key was her spirometric flow-volume loop. Ultimately, she was found to have a tracheal web by bronchoscopy and was successfully treated with endobronchial argon plasma coagulation.
CLUES TO THE CAUSE OF WHEEZING
In fairness to those who treated her for asthma and COPD, these obstructive diagnoses are common causes of shortness of breath and wheezing, and an empiric trial of therapy is often reasonable. However, we guess there may have been clues early in her course to suggest this was not ordinary obstructive disease. Using this case, we offer a systematic approach to dissecting the etiology of wheezing by reviewing the patient’s history, physical examination, and pulmonary function testing.
The patient’s history
This patient presented with progressive shortness of breath, although it is unclear whether it was variable, which is usually a feature of asthma, especially early on. We know she had never smoked. Nonsmokers can, of course, have asthma, and they can also have COPD, but this is much less common.
Whenever a nonsmoker is diagnosed with COPD, it is worth asking about possible exposure to biomass fuels (rare in developed areas of the world), other airway irritants, and underlying predisposing conditions. Anyone suspected of having COPD, regardless of smoking history, should also be tested for alpha-1 antitrypsin deficiency, with both alpha-1 antitrypsin level and genotype analysis.
COPD severity is often classified according to the criteria of the Global Initiative for Chronic Obstructive Lung Disease (Table 1), which determines its suggested treatment.3 Our patient would be classified as being in group D based on frequent hospitalizations and severe symptoms, which would generally require therapy with long-acting bronchodilators and possibly inhaled corticosteroids.3 These treatments were ineffective. Once it became clear that usual therapies for both asthma and COPD were ineffective, an indepth evaluation of her airway disease was indicated.
Global Initiative for Chronic Obstructive Lung Disease classification of COPD, with recommended therapy
The physical examination
Our patient apparently had wheezing early on, although we are not told whether she herself heard any airway noise or whether it was appreciated only on examination. Wheezing is typically a sign, not a symptom, meaning the sound is detected on lung auscultation, and usually the patient is unaware of it. If the patient reported her own wheezing, then we should immediately suspect the airway noise is probably stridor.
Careful examination can usually distinguish these 2 different airway sounds. Wheezing is the polyphonic (multipitch or “musical”) sound made by airflow through small and medium airways, the “distal” airways. It is predominantly or often exclusively heard on expiration due to lung parenchyma compression during expiration, which further narrows the distal airways. No distinguishing feature of wheezing can tell us whether it is due to asthma or COPD. Either diagnosis may be associated with rhonchi or other additional airway sounds.
Stridor is the sound made by airflow through an obstructed large central (proximal) airway. Some causes of stridor cause obstruction exclusively on expiration or inspiration, but many cause obstruction during both phases of breathing. Also, since stridor is usually caused by a focal narrowing at one point in the airway, its pitch is usually constant or monophonic.
It is likely that this woman’s airway noise was monophonic and heard during both inspiration and expiration, both features suggestive of stridor.
Pulmonary function testing
The hallmark of obstruction on pulmonary function testing is a reduced ratio of forced expiratory volume in 1 second to forced vital capacity (FEV1/FVC), meaning that the FEV1 is reduced out of proportion to the FVC.4 Since a reduced FEV1/FVC ratio reflects decreased airflow, this pattern is seen in any condition that inhibits or “obstructs” that flow, such as asthma, COPD, or a fixed narrowing of an airway.
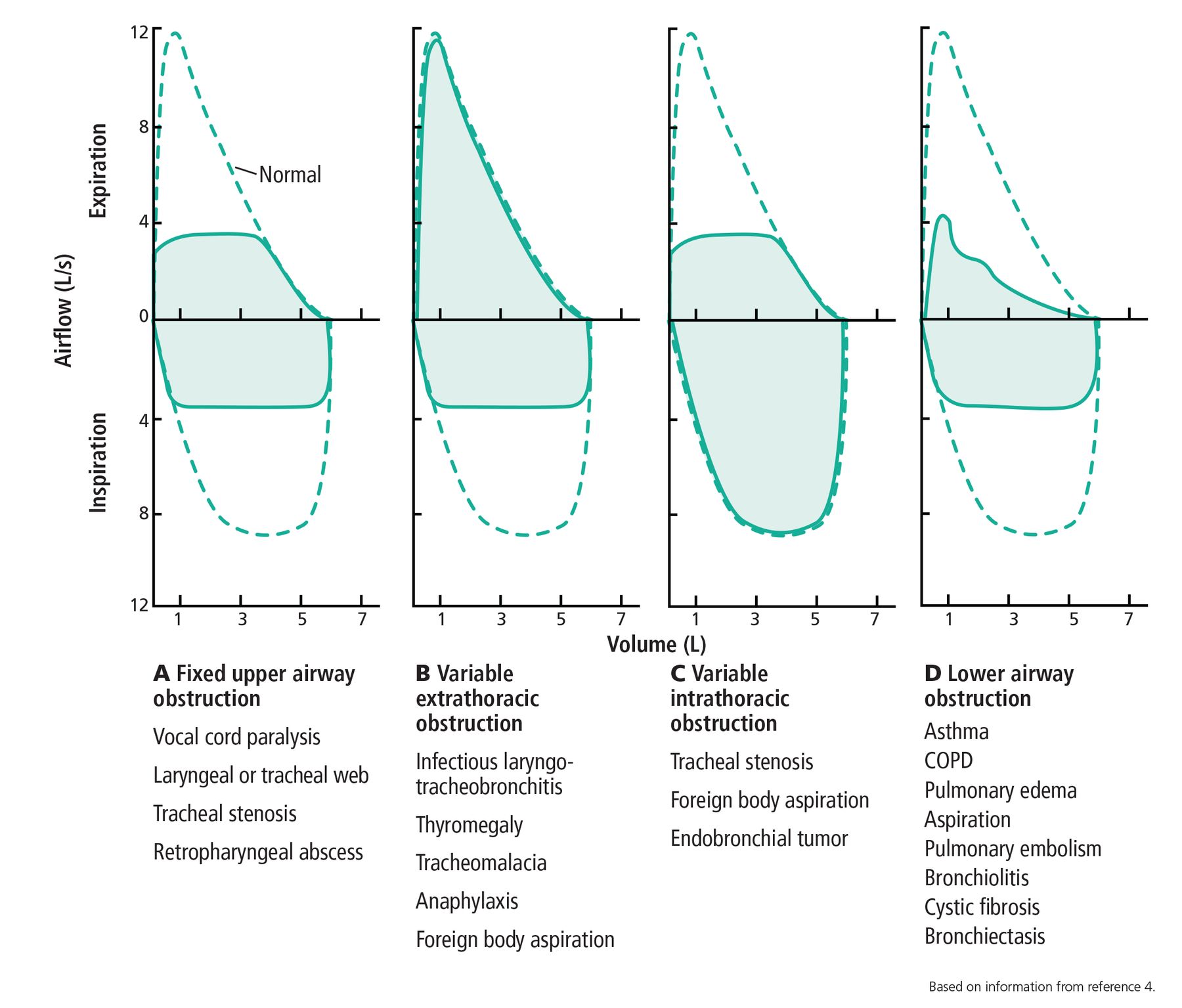
Fortunately, pulmonary function testing gives additional information that can help identify more specific causes of reduced flow. As a general rule for variable obstruction lesions, an upper airway obstruction (outside the thorax) will predominantly limit inspiratory flow (Figure 1B), whereas intrathoracic obstruction will mostly decrease the expiratory flow (Figure 1C). Our patient’s flow-volume loop showed attenuation of both expiratory and inspiratory flow, suggestive of a central fixed obstruction (Figure 1A).
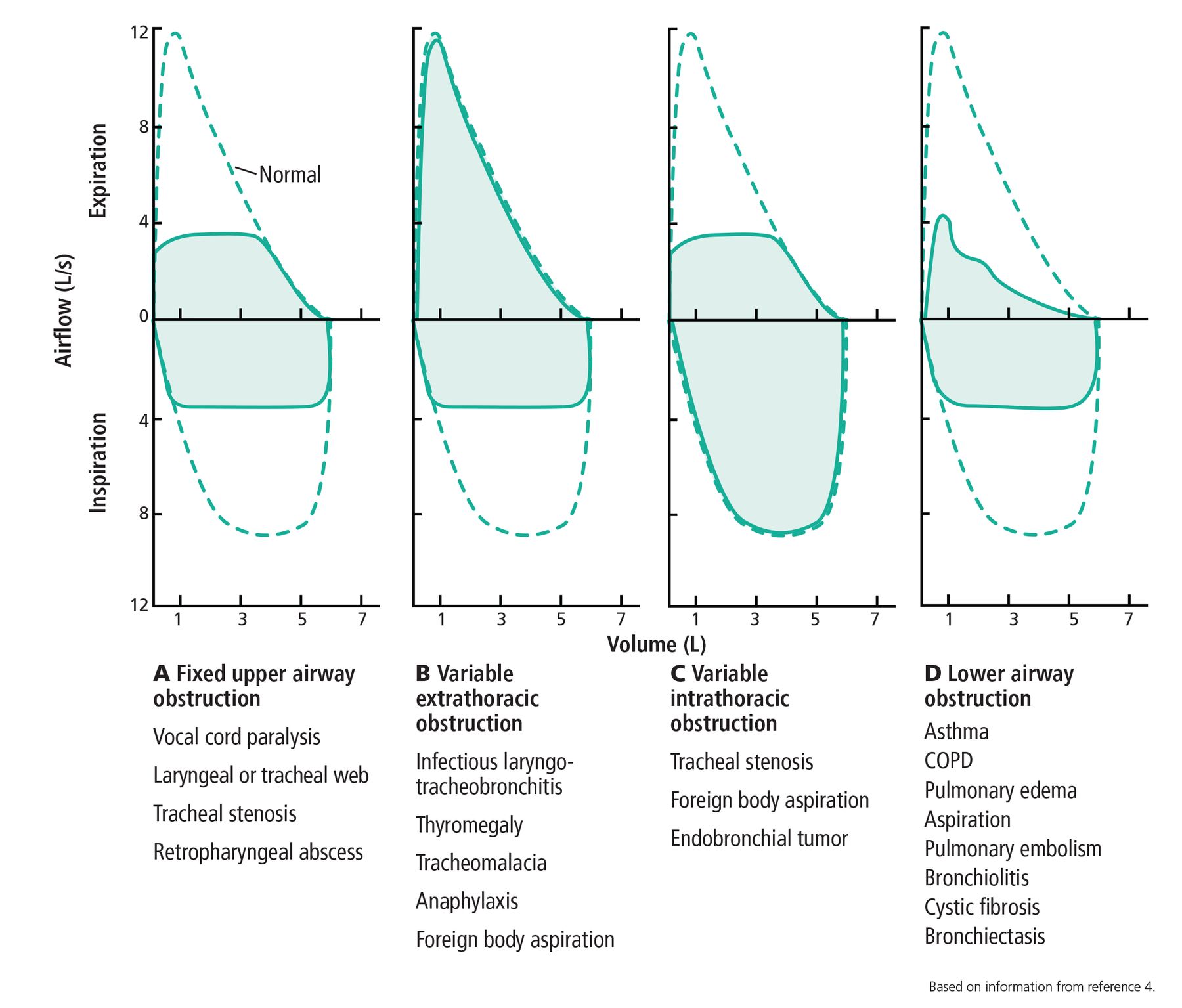
Attenuation of the flow-volume loop in different types of airway obstruction.
Pulmonary function testing cannot diagnose a tracheal web. Only bronchoscopy can show the specific cause of obstruction, but the flow-volume loop is the strongest evidence before invasive inspection that the problem is not a distal airways disease like asthma or COPD.6
TAKE-HOME MESSAGE
It is always far easier to critique the diagnostic missteps of others than to make the correct diagnosis yourself. We make no claims of always going straight to the right answer in our own clinic. The case reported by Patel and Madan is an excellent example of the diagnostic pitfalls presented by common combinations of complaints and findings. A thorough and systematic approach, emphasizing the medical history, the physical examination, and the correct interpretation of pulmonary function test results ultimately led the clinicians to the correct diagnosis.
Perhaps the take-home message is that while we enjoy unprecedented diagnostic advantages due to advanced and emerging technology, in the end, even rare and unusual diseases are usually identified with the fundamental tools of a sound history, physical examination, and basic, targeted testing.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2021 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.