


Article Figures & Data
Figures
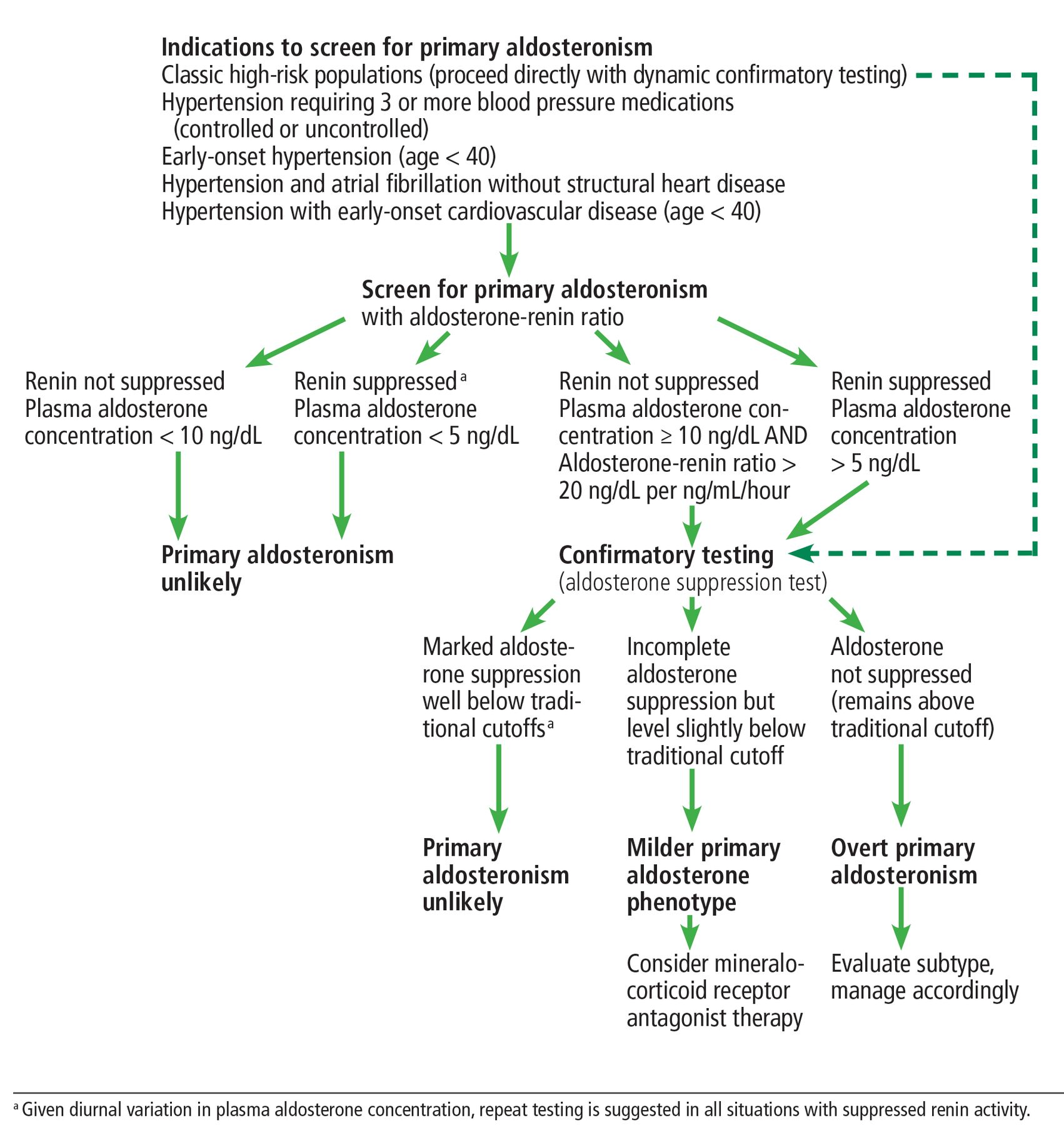
- Figure 1
Our suggested algorithm for screening for and diagnosis of primary aldosteronism.

Tables
Screening tests More conservative Most widely accepted More liberal Aldosterone-renin ratio (ng/dL per ng/mL/hour) ≥ 40 ≥ 30 ≥ 20 Plasma aldosterone concentration (ng/dL) ≥ 20 ≥ 15 ≥ 10 Confirmation aldosterone suppression tests More conservative More liberal With oral salt 24-Hour urinary aldosterone excretion rate (μg) > 12–14 > 10 With intravenous saline Plasma aldosterone concentration (ng/dL) > 10 > 5 With fludrocortisone Seated plasma aldosterone concentration (ng/dL) > 6 with plasma renin activity < 1 ng/mL/hour With captopril Plasma aldosterone concentration, < 30% decrease from baseline Aldosterone-renin ratio (ng/dL per ng/mL/hour) > 30 > 20 Based on information in references 2 and 11.




{kind=link}