


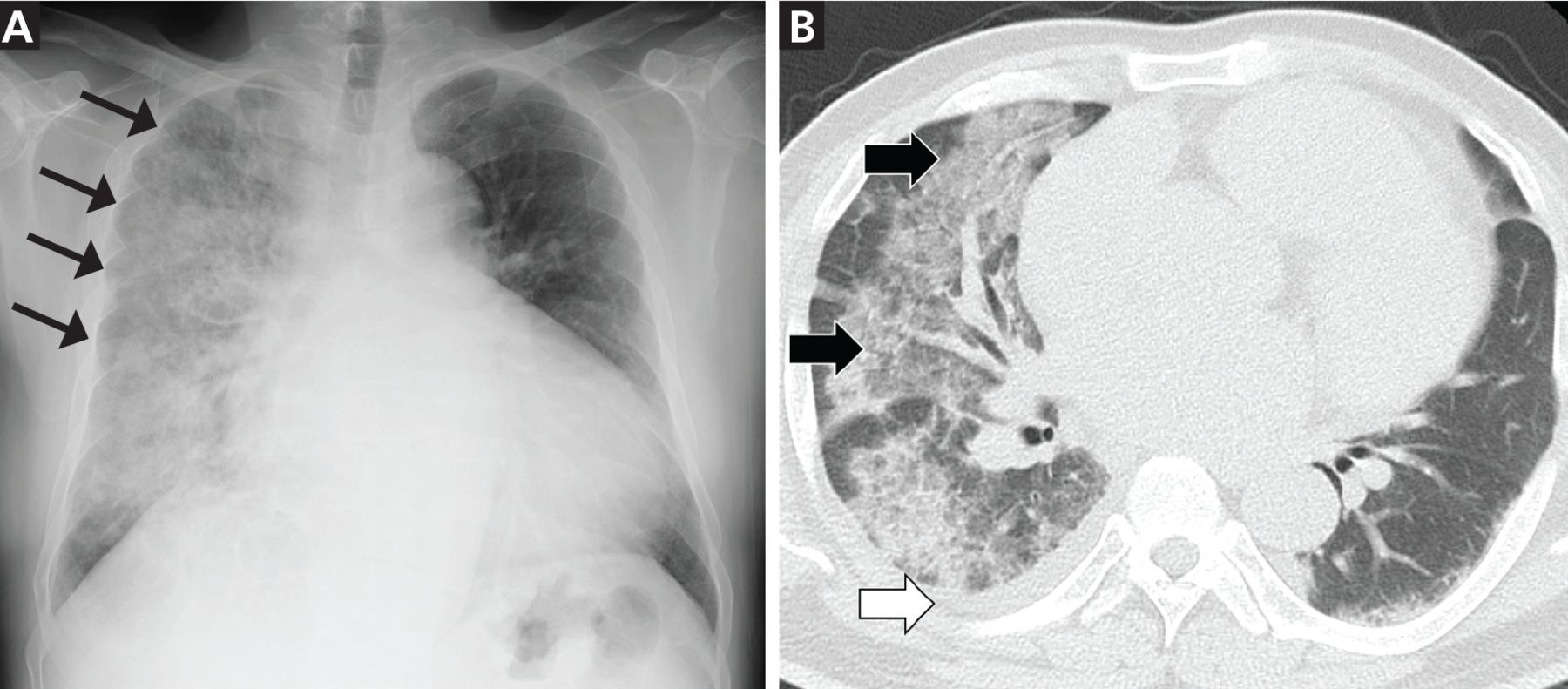
A 48-year-old man was transferred to our hospital for dyspnea. Although he had no significant medical history, he had been hospitalized for COVID-19 at a local healthcare facility 1 month earlier. Three weeks after discharge from that facility, he noted progressively worsening exertional dyspnea and fatigue. He returned to that facility, where he was afebrile at presentation and was diagnosed with bacterial pneumonia secondary to COVID-19 infection based on chest radiography and computed tomography that revealed a unilateral consolidation in the right lung and an inexplicable enlargement of the heart (Figure 1).

(Left) Chest radiography showed a right unilateral consolidation (arrows) and enlarged cardiac silhouette. (Right) Chest computed tomography revealed diffuse ground-glass opacities and consolidation (black arrows) together with a small amount of pleural effusion in the right lung (white arrow).
On admission to our facility, he presented with the following vital signs:
Clear level of consciousness
Blood pressure 134/96 mm Hg
Pulse rate 120 beats per minute
Body temperature 36.1°C (96.9°F)
Respiratory rate 24 breaths per minute
Oxygen saturation 91% on oxygen delivered by nasal cannula at 2 L per minute.
Physical examination revealed mild right jugular venous distention and mild pitting edema of the lower extremities. Coarse crackles were noted in the right lung, but no abnormal heart sounds were documented.
Although electrocardiography was unremarkable except for sinus tachycardia with no ST-segment or T-wave abnormalities, we considered heart failure in the differential diagnosis given his findings on physical examination and imaging. Transthoracic echocardiography revealed diffuse left ventricular hypokinesis with an ejection fraction of 20% and moderate mitral regurgitation toward the posterior left atrial wall. Additionally, his serum N-terminal probrain natriuretic peptide level was 6,469 pg/mL (reference range, 0–125 pg/mL). The patient was diagnosed with congestive heart failure and was placed on intravenous furosemide, nitrates, and noninvasive positive pressure ventilation. Initial therapy dramatically improved his dyspnea and chest radiograph within 72 hours after admission without the use of antibiotics (Figure 2). The patient made a full recovery and was discharged on hospital day 11.

Chest radiograph 72 hours after admission and initiation of intravenous furosemide, nitrates, and noninvasive positive pressure ventilation. Unilateral consolidation in the right lung rapidly improved.
UNILATERAL PNEUMONIA WITH COVID-19
Approximately 1 out of every 10 patients with COVID-19 pneumonia presents with unilateral––as opposed to bilateral—pneumonia.1 Generally, one would consider viral or secondary bacterial pneumonia as the most likely diagnosis when a patient presents with unilateral consolidations on chest radiography. However, cardiogenic pulmonary edema accounts for 2.1% of unilateral pulmonary edema.2
On imaging, cardiogenic pulmonary edema generally appears as an opacity involving the right lung and is frequently attributed to severe mitral regurgitation.2 The direction of the mitral regurgitation toward the posterior left atrial wall could selectively impede the right pulmonary venous system,3,4 and the regurgitant flow may focally elevate the pressure in the right pulmonary vein.4 Our patient had retrograde blood flow toward the posterior left atrial wall. However, we could not confirm “severe” mitral regurgitation. Other factors that would affect the distribution of pulmonary edema include decubitus position of the patient (gravitational effect), position of the pulmonary veins, and preexisting lung disease.4
When encountering unilateral lung consolidations on chest imaging during the COVID-19 era, one should avoid the common pitfall of hastily attributing the finding to COVID-19 and instead should consider the full spectrum of differential diagnoses, including cardiogenic pulmonary edema.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}