


It depends. If dilation of the common bile duct is detected incidentally with ultrasonography or computed tomography (CT) and the patient has clinical signs (eg, jaundice, pruritus, fever, weight loss), concerning laboratory test results (eg, elevated total bilirubin), or additional concerning imaging findings (Table 1), then further evaluation is indicated with magnetic resonance cholangiopancreatography (MRCP) with contrast, endoscopic ultrasonography (EUS), or endoscopic retrograde cholangiopancreatography (ERCP). If the patient does not have clinical signs or concerning laboratory test results but does have risk factors for nonobstructive dilation such as age over 60, previous cholecystectomy, or opioid use, then the dilation is likely benign, and further investigation is not warranted.
Clinical considerations and red flags for incidental bile duct dilation
To avoid unnecessary testing and imaging, a patient-centered approach integrating the clinical history, liver biochemistries, and knowledge of the diagnostic yield of further testing can help clinicians determine appropriate management for incidentally detected common bile duct dilation.
WHAT CONSTITUTES BILE DUCT DILATION?
There is no absolute measurement that defines common bile duct dilation, but a dilation of 7 mm or greater is generally accepted as the cutoff for clinical and research purposes. It is important to note that measurement ranges for dilation vary based on the imaging modality, site of measurement along the duct, and patient factors (eg, age, history of cholecystectomy). The upper limit of normal for common bile duct diameter is 6 to 8 mm when measured with transabdominal ultrasonography, and 8 to 10 mm with CT.1 To adjust for age, adding 1 mm to the measurement per decade of life after age 60 or 0.4 mm for each decade of life has been proposed, although the evidence varies.1 After cholecystectomy, asymptomatic common bile duct dilation of up to 10 mm has been reported to be within normal range.2 Given the challenges to defining specific dilation values, the decision to pursue further diagnostic testing should be based on the likelihood of underlying obstructive vs nonobstructive causes.
Obstructive vs nonobstructive causes
Obstructive causes of common bile duct dilation include choledocholithiasis, malignancy (eg, pancreatic cancer, cholangiocarcinoma, ampullary carcinoma), extrinsic compression (eg, Mirizzi syndrome, lymphadenopathy, fluid collections), chronic pancreatitis stricture, periampullary diverticulum, primary sclerosing cholangitis, papillary stenosis, and parasitic worm infection (uncommon in the United States).1,3 A nonobstructive dilation can be related to age over 60, previous cholecystectomy (or other bile surgery), and opioid use,4 and dilation in patients with these risk factors is considered benign.
Rarely, bile duct dilation is caused by cysts (eg, choledochal cysts),5 which typically have a distinct appearance on imaging.
CLINICAL EVALUATION
Specific elements of the patient’s history, physical examination, and biochemical markers can help determine if biliary obstruction warrants further investigation (Table 1). Clinical symptoms such as jaundice, steatorrhea, acholic stools, dark urine, pruritus, and weight loss can reflect obstructive causes, which may include malignancy. The combination of fever, abdominal pain, and jaundice (Charcot triad) suggests ascending cholangitis, which occurs more commonly with choledocholithiasis than with malignancy in the absence of a previous biliary procedure such as ERCP.1 Acute onset of symptoms including pain is typical of choledocholithiasis, whereas gradual weight loss and jaundice (often painless) suggest a malignant process.
Abnormal liver biochemistry results including elevation of total or direct serum bilirubin, alkaline phosphatase, aspartate aminotransferase, and alanine aminotransferase can indicate an obstructive cause and should be evaluated. To some degree, these levels can be elevated in the setting of common bile duct obstruction, depending on the cause, extent, and chronicity of disease. Moreover, imaging with EUS is more likely to reveal a cause for dilated common bile duct in patients with elevated liver biochemistries than in those without (53% vs 6%), highlighting the importance of testing for these abnormalities.6 Although this article focuses on evaluating incidental common bile duct dilation, if abnormal liver biochemistries persist after an appropriate workup for bile duct dilation (see discussion below), further assessment is needed in accordance with published guidelines7 and in consultation with gastroenterology and hepatology specialists.
If there are no concerning clinical or biochemical findings for obstruction and there is no explanation for nonobstructive dilation such as older age, previous cholecystectomy, or opioid use, imaging should be done to exclude features suggestive of an infrequently encountered subclinical or impending obstructive process. These include a concurrently dilated pancreatic duct (the “double-duct sign”), which could indicate a pancreatic or ampullary tumor; an appreciable intraductal biliary stone or lesion suggesting choledocholithiasis; intrahepatic duct dilation (≥ 1–2 mm); moderate to severe extra-hepatic bile duct dilation (≥ 10 mm), or an abrupt cutoff of the common bile duct dilation.1,8 If available, prior imaging (including an intraoperative cholangiogram performed during cholecystectomy) should also be reviewed as a new or progressive dilation may be more concerning than a chronic stable dilation.
In the absence of the above findings, mild ductal dilation may be benign, especially in patients who are over age 60, have undergone cholecystectomy, or use opioids, and does not warrant further evaluation. Studies have shown that further diagnostic testing of incidentally found asymptomatic ductal dilatations without clinical or biochemical abnormalities has very low diagnostic yield,9 but it is a potential area for research.10
IMAGING OPTIONS FOR WORKUP
If a common bile duct dilation is identified and the decision is made to pursue further workup, the next step is to determine which imaging modality to use. The most commonly used options are described below.
MRCP with contrast
MRCP with contrast detects the cause of bile duct obstruction more accurately than transabdominal ultrasonography and CT. Its sensitivity for detecting choledocholithiasis is 92% and its specificity is 97%, depending on stone size; the sensitivity for malignancy is 88%, and the specificity is 95%.1 Because MRCP is noninvasive and does not require ionizing radiation, it can be a useful first tool for evaluation of bile duct dilation. However, its reported accuracy in distinguishing benign from malignant causes of obstruction varies widely, from 30% to 98%.1 The cost of the procedure is high compared with transabdominal ultrasonography and CT. In addition, some patients may suffer from severe claustrophobia or have difficulty holding their breath or lying still during the scan, potentially causing motion artifact and decreasing sensitivity of the imaging for smaller stones.1
Endoscopic ultrasonography
EUS provides high-resolution images of the pancreaticobiliary system, detecting choledocholithiasis with greater than 90% sensitivity and up to 100% specificity, and pancreatic neoplasms such as carcinoma and cysts with sensitivity of 90% or greater.1 If abnormalities are identified, diagnostic biopsy via fine-needle aspiration or fine-needle (core) biopsy can be performed as well. Visualization can be limited by pancreatic calcifications, inflammation from acute pancreatitis, altered anatomy of the stomach and proximal duodenum, and pneumobilia (most commonly resulting from previous instrumentation).1 Due to the cost and the need for sedation, EUS is typically performed in patients with a high probability of bile duct obstruction and with an anticipated need for tissue acquisition or intervention, or in patients for whom MRCP with contrast is not possible or is contraindicated.
Cholangiopancreatography
ERCP is primarily a therapeutic intervention when obstruction is probable (ie, there are signs of ascending cholangitis) rather than for purely diagnostic purposes, and it is typically preferred over percutaneous or surgical methods.11 This shift toward its use as a therapeutic modality is partly due to advances in noninvasive imaging (MRCP with contrast, EUS) that obviate the need for diagnostic ERCP and its related adverse events such as post-ERCP pancreatitis. In patients with bile duct obstruction, ERCP can provide decompression via sphincterotomy, stone extraction, or stent placement. If indicated, it can be performed immediately after EUS during a single session of anesthesia.12
CLINICAL APPROACH TO THE EVALUATION
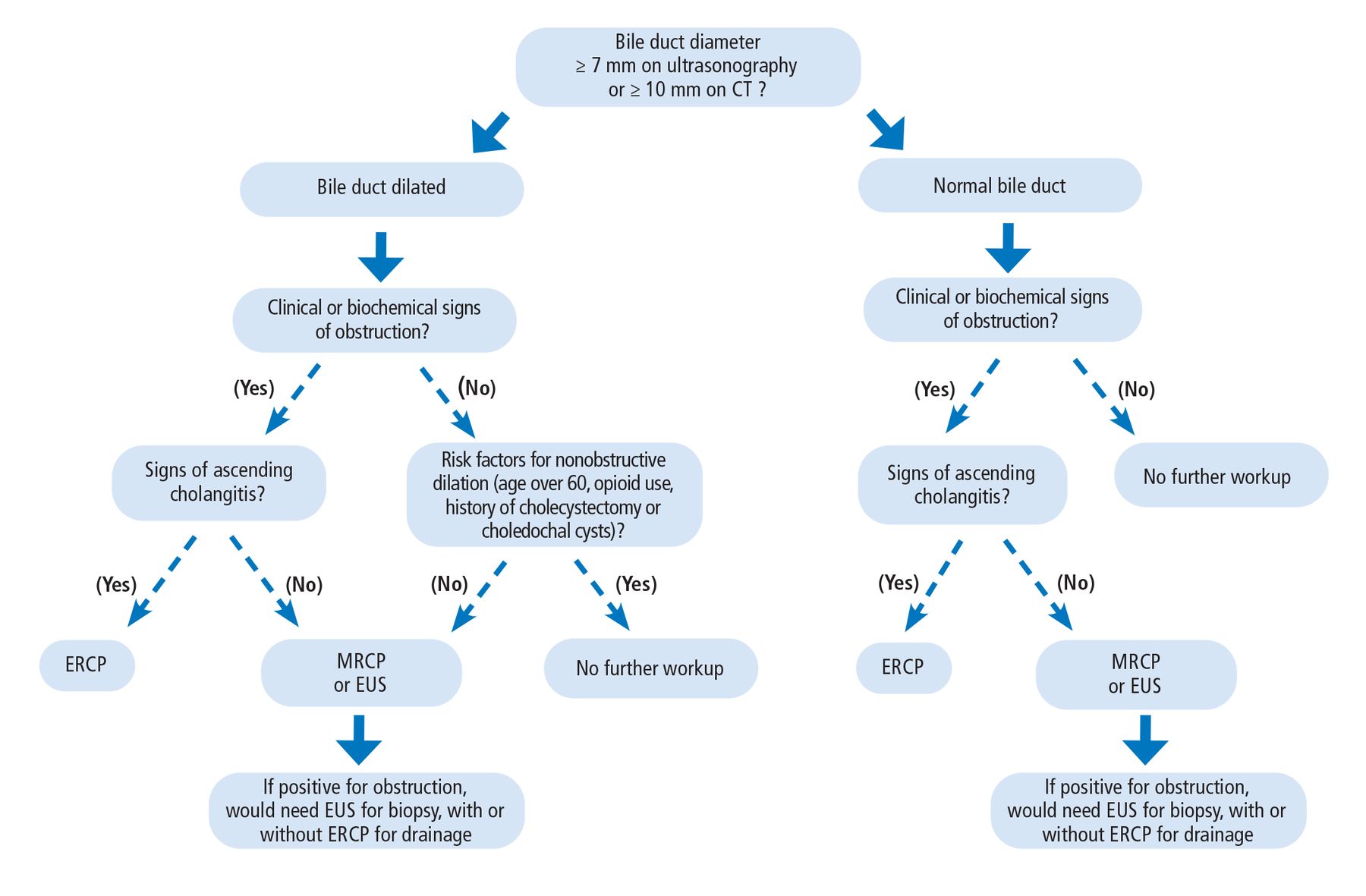
For a patient with potential incidental bile duct dilation, there are 4 general clinical decision-making pathways, as follows (Figure 1)1,3:
Common bile duct dilation (ie, ≥ 7 mm on ultrasonography or ≥ 10 mm on CT) with clinical or biochemical features of obstruction warrants further investigation. ERCP is the initial choice if there are signs of ascending cholangitis. If there are no signs of ascending cholangitis, MRCP with contrast or EUS is indicated, and if these imaging results are positive for obstruction, EUS for biopsy with or without ERCP for drainage is needed.
If there is dilation but no clinical or biochemical signs of obstruction, and if the patient has risk factors for nonobstructive dilation (eg, older age, previous cholecystectomy, opioid use), no further workup is warranted. But if the patient has no risk factors for nonobstructive dilation, then pursue MRCP with contrast or EUS.
If the common bile duct diameter is normal (ie, < 7 mm on ultrasonography or < 10 mm on CT) but there are clinical or biochemical signs of obstruction, further evaluation is warranted. If there are signs of ascending cholangitis, an ERCP is indicated. If there are no signs of ascending cholangitis, MRCP with contrast or EUS is indicated. If either imaging test shows an obstruction, EUS for biopsy with or without ERCP for drainage is needed.
If the bile duct diameter is normal and there are no clinical or biochemical characteristics of obstruction, further evaluation is not indicated.
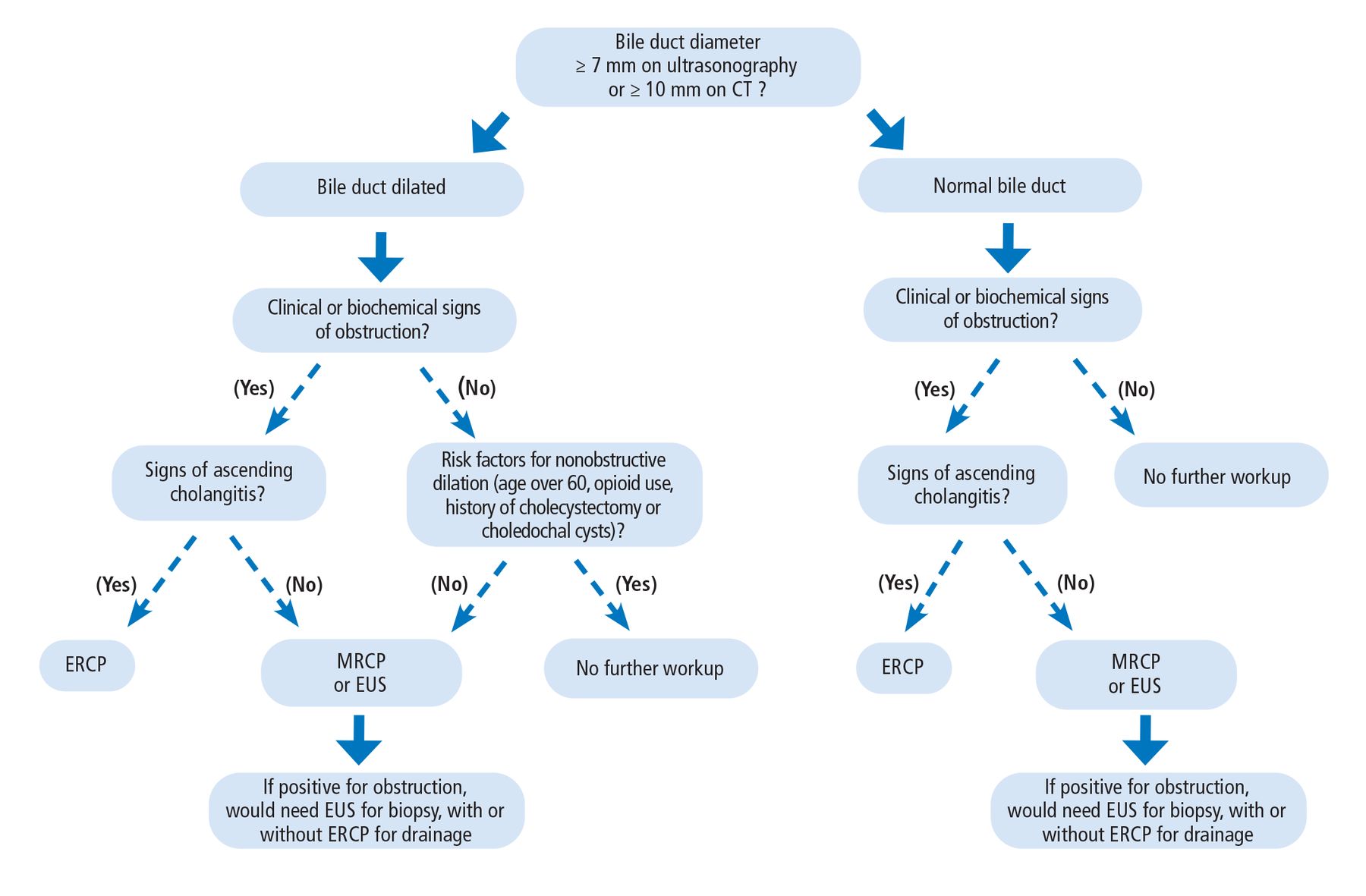
Clinical approach to incidental bile duct dilation.
CT = computed tomography; ERCP = endoscopic retrograde cholangiopancreatography; EUS = endoscopic ultrasonography; MRCP = magnetic resonance cholangeopancreatography
Based on information in reference 1.
If EUS or ERCP is warranted or if there is uncertainty regarding the workup of bile duct dilation, the patient should be referred to a gastroenterologist.
TAKE-HOME POINTS
Once identified, incidental common bile duct dilation can be categorized as nonobstructive or obstructive. Clinical, biochemical, and imaging findings should guide the decision-making regarding further evaluation or intervention. MRCP with contrast and EUS can provide an accurate and minimally invasive diagnostic evaluation, while ERCP is best reserved for patients who require therapeutic intervention.
DISCLOSURES
Dr. Sethi has disclosed consulting for Boston Scientific, Fujifilm, Interscope, Medtronic, and Olympus America. The other authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.