


An 87-year-old man presented to an orthopedic clinic with a 2-month history of dull pain below his right knee. Magnetic resonance imaging revealed an encapsulated mass in the right tibia (Figure 1). Based on this result and the patient’s clinical course, subacute osteomyelitis was suspected, but the patient was managed symptomatically without antibiotic treatment because his symptoms and general condition were mild and stable.

Imaging results of the patient’s lower right leg taken 1 year before hospital admission. On the left, T2-weighted magnetic resonance imaging shows an encapsulated abscess surrounded by granulation tissue and bone edema (arrow) in the proximal part of the right tibia, causing subacute osteomyelitis. On the right, radiography shows a mass lesion (arrow), misdiagnosed as a bone tumor.
One year later, he was admitted to the hospital because of swelling of the anterior aspect of the right proximal tibia. At that time, he was afebrile, without any history of a possible source of infection such as recent trauma or dental procedure.
Laboratory testing results revealed elevation of the following inflammatory markers:
White blood cell count 9.3 × 103 cells/μL (reference range 3.3–8.6)
C-reactive protein level 65.2 mg/L (0–3)
Erythrocyte sedimentation rate 100 mm/h (2–10).
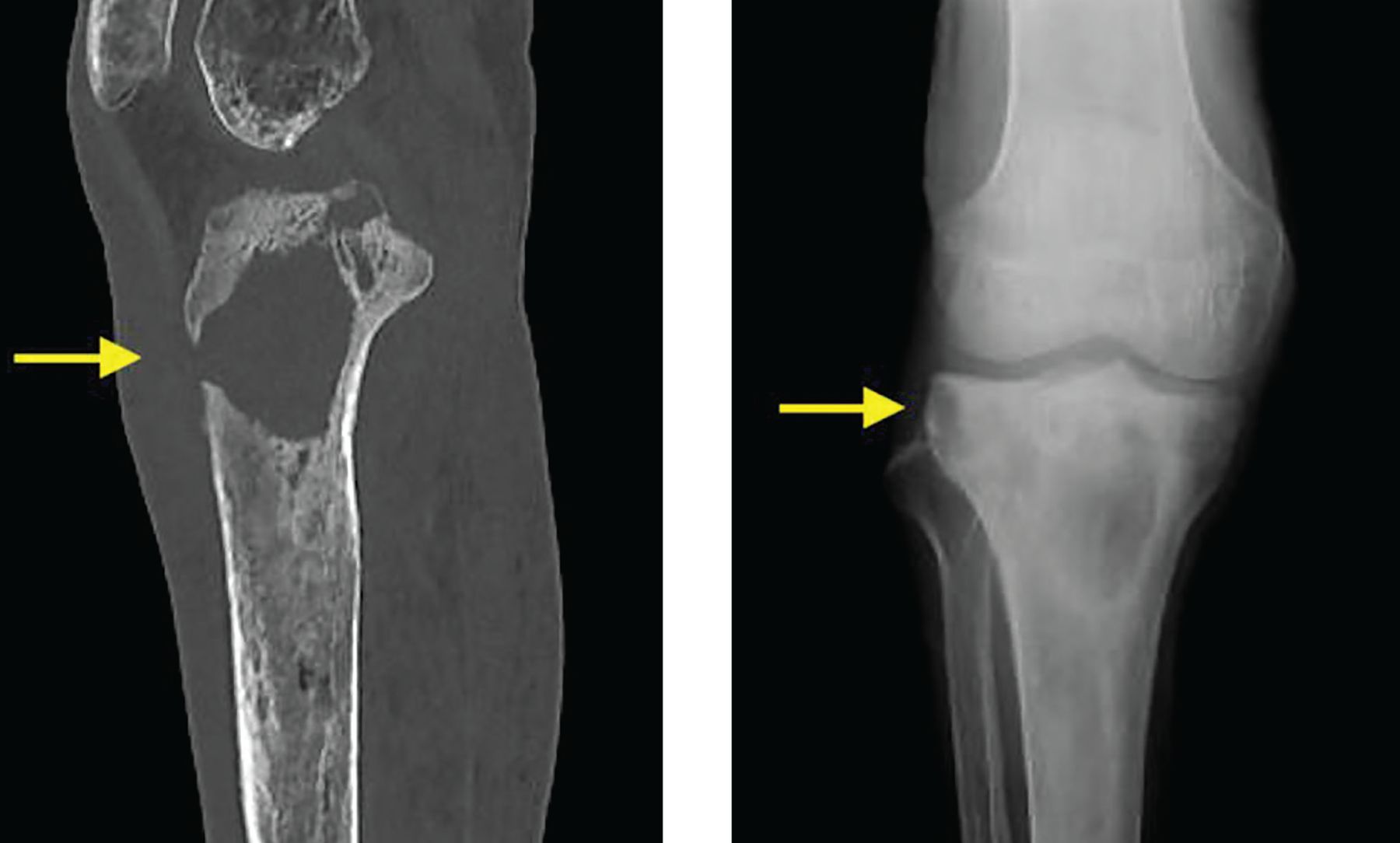
Computed tomography and plain radiography revealed a sinus tract connecting the tibial lesion to the subcutaneous tissue (Figure 2). The patient underwent surgical debridement of the abscess. Culture of a pus sample obtained intraoperatively grew methicillin-resistant Staphylococcus aureus, but a blood culture was negative. According to the patient’s clinical course and imaging findings, he was suspected of having presented with Brodie abscess at his initial presentation at the orthopedic clinic 1 year earlier, and the lesion was considered to represent a deterioration of untreated chronic osteomyelitis since that time.

On hospital admission, computed tomography (left) demonstrated a well-visualized sinus tract connecting to subcutaneous tissue (arrow), and radiography (right) of the abscess showed well-circumscribed osteolysis with sclerotic margins (arrow), which had developed during the year since the initial presentation.
The patient’s symptoms improved with a 4-week course of intravenous vancomycin. He continued antibiotic therapy after discharge, with a 3-month course of oral minocycline. At a follow-up visit 6 months after debridement, his symptoms were controlled with no evidence of clinical relapse.
BRODIE ABSCESS: CAUSES AND CLINICAL COURSE
Brodie abscess, first reported in 1832 by Sir Benjamin Collins Brodie,1 is a rare form of subacute or chronic osteomyelitis, usually affecting the metaphysis of long bone. Most cases occur in children and young adults, and the most commonly affected bone is the tibia.2–5 S aureus is the most common causative pathogen (over 60% of cases), followed by gram-negative rods, including Enterobacteriaceae and Pseudomonas aeruginosa, although 20% of cases are culture-negative.2,3 These pathogens are also the most common cause of acute infections, including osteomyelitis.6 However, patients with Brodie abscess can present with an insidious course, with or without fever,7–9 potentially leading to misdiagnosis of a benign or malignant bone tumor and delay in appropriate antibiotic treatment. The main source of infection is by hematogenous spread, which is often unclear because of the long clinical course of the disease.
A systematic review revealed that the possible etiologies were reported only in 56 of 407 cases, with both recent systemic infection and minor trauma being present.3 The diagnosis of Brodie abscess is confirmed based on results of radiologic imaging and culture. Inflammatory markers are unreliable diagnostic tools for Brodie abscess as they frequently show only a slight elevation or are within the normal range.3 In our patient, the C-reactive protein level was mildly elevated, but the erythrocyte sedimentation rate was significantly elevated.
TREATMENT IS SURGICAL AND MEDICAL
The standard treatment for Brodie abscess is a combination of surgical debridement and systemic antibiotic therapy.3 If the culture results reveal the causative pathogens, these results should guide the choice of antibiotic.
Antibiotic treatment duration varies from at least 10 days to 3 months or longer, depending on the clinical condition of the patient. However, patients are often treated for 4 to 6 weeks, including a few weeks of intravenous antibiotics combined with surgical debridement.3,7 Regarding surgical intervention, large cavities sometimes require stabilization by bone grafting.2 Although data on outcomes are limited, relapse rates are reported to be approximately 15% for Brodie abscess3 and 20% for chronic osteomyelitis.10
Our 87-year-old patient was observed symptomatically by his primary physician for 1 year with slow progression of his disease, which characterized the typical chronic clinical course of this disease. However, the treatment should be initiated as soon as possible when a chronic abscess is suspected, as case reports also reveal that delay of treatment can slowly exacerbate the abscess, eventually leading to a sinus tract, a fistula connecting skin and soft tissue, or bone fracture.3,9,11
Brodie abscess is rare in older adults. However, timely diagnosis and treatment can prevent exacerbation of the abscess and avoid the need for additional surgical treatment such as bone grafting or amputation, thus shortening the duration of hospitalization and preventing long-term complications.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2023 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.