


Patients with chronic diarrhea or malabsorption (evidenced by weight loss, failure to thrive, or steatorrhea) should be tested for celiac disease (CD). To increase detection, testing is also recommended for patients with other symptoms or conditions that occur with CD, including bloating, constipation, abdominal pain, iron-deficiency anemia, elevated transaminase levels, neuropathy, ataxia, and infertility. Testing is also advisable for patients at increased risk of developing CD, including first-degree relatives of patients with CD, patients with dermatitis herpetiformis, and those who have autoimmune conditions such as type 1 diabetes mellitus and autoimmune thyroid disease.
The screening test of choice is tissue transglutaminase (TTG) immunoglobulin A (IgA) along with total IgA. Duodenal biopsy is indicated to confirm the diagnosis in patients with positive serology or high clinical suspicion.
WHAT IS CELIAC DISEASE?
CD is a chronic immune-mediated systemic disorder triggered in genetically susceptible people by the ingestion of gluten, a water-insoluble protein that is a constituent of wheat, rye, and barley. CD is characterized by inflammatory injury to the small bowel with gastrointestinal or systemic manifestations, or both. It can also exist with minimal or even no symptoms. Approximately 1% of the general population is affected1; most of those affected remain undiagnosed.
WHO SHOULD BE TESTED FOR CELIAC DISEASE?
The evidence that guides testing for CD continues to evolve. Classically thought to be only a syndrome of malabsorptive diarrhea, the disease is now recognized as having a myriad of nonclassical presentations. CD affects both men and women with a preponderance for women. It may occur at any age, with more than 20% of patients presenting after age 60.2 Diarrhea is found in only 30% of newly diagnosed patients.3 Despite the malabsorptive state, around 27% of CD patients in the United States are overweight.4
A 2017 US Preventive Services Task Force review found insufficient evidence to recommend screening the general asymptomatic population for CD.5 Accordingly, mass screening is not recommended in clinical practice. Diagnosis relies on maintaining an appropriate index of suspicion and using a case-finding approach,6 ie, actively screening patients who have signs or symptoms consistent with CD or belong to a high-risk group with an increased incidence of CD. Testing for CD in many of these conditions remains controversial, but it is advised and is proven to increase the identification of patients with CD.6
Classical signs and symptoms of CD that warrant testing include chronic diarrhea, particularly with evidence of malabsorption, steatorrhea, weight loss, and failure to thrive. Patients presenting with the classical dermatitis herpetiformis rash should also be tested.6,7
Nonclassical signs and symptoms of CD that warrant testing in the absence of a convincing alternative diagnosis or explanation include iron-deficiency anemia, chronically elevated serum transaminases with no alternative explanation, dyspepsia with postprandial abdominal discomfort and bloating, recurrent abdominal pain, chronic constipation, ataxia, epilepsy, peripheral neuropathy, infertility, recurrent miscarriages, delayed sexual maturity, short stature, early-onset osteoporosis, dental enamel hypoplasia, recurrent aphthous stomatitis, arthritis or arthralgia and myalgia, chronic fatigue, recurrent pancreatitis, and hyposplenism.6,8
High-risk groups with an increased incidence of CD that warrant testing include first-degree relatives of patients with CD and patients with Down syndrome, Turner syndrome, or Williams syndrome. High-risk groups also include patients with autoimmune conditions such as type 1 diabetes mellitus, autoimmune thyroid disease, autoimmune hepatitis, lupus erythematosus, and psoriasis, as well as those with microscopic colitis and selective IgA deficiency.6,8
TESTING AND DIAGNOSTIC LIMITATIONS
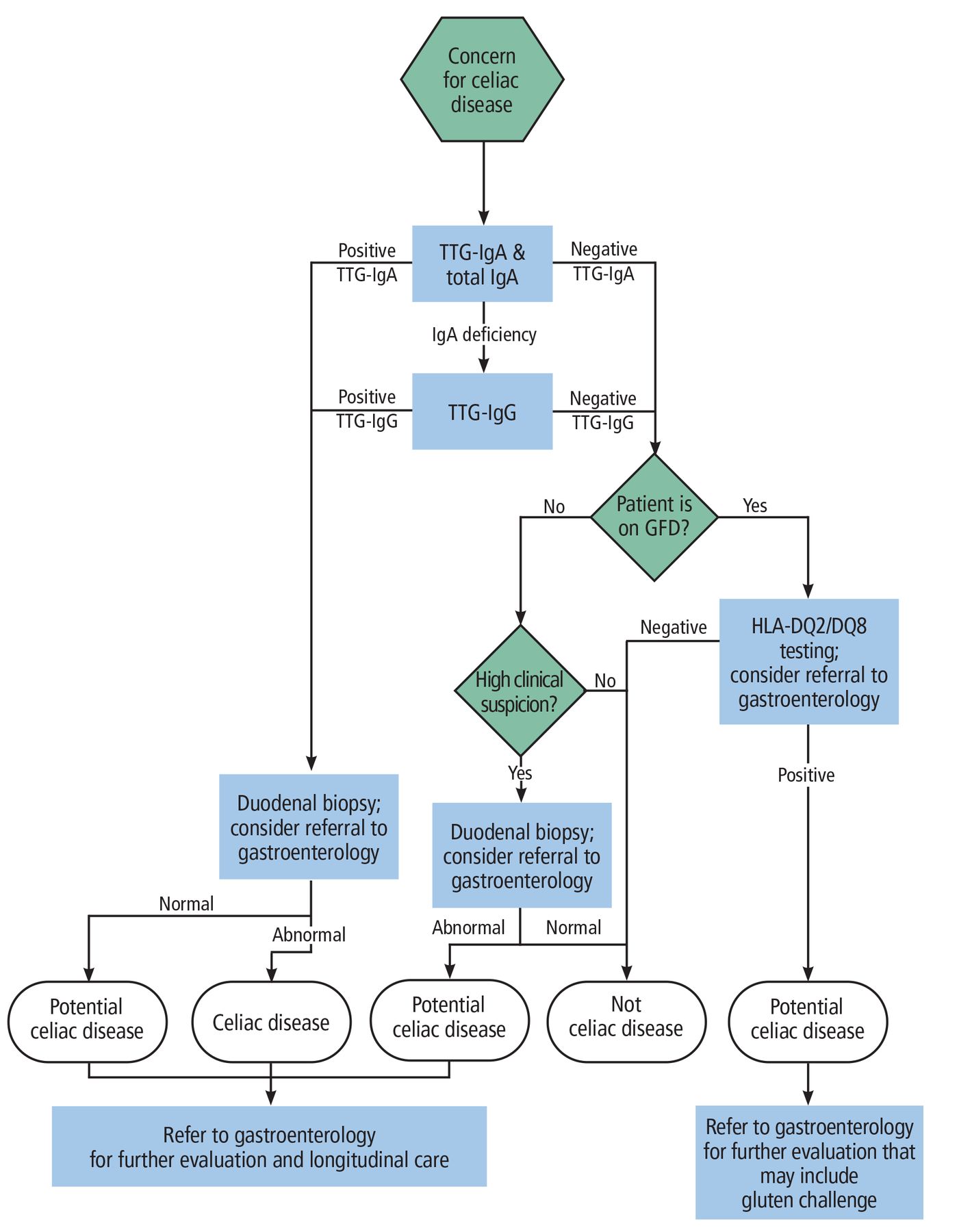
There is no gold standard for the diagnosis of CD. The diagnostic process considers the clinical picture, serology, and histology together (Figure 1) because no symptom or sign is specific for CD. Even symptomatic improvement on a gluten-free diet has a diagnostic precision as low as 30%, and this outcome is common in other disorders such as nonceliac gluten sensitivity, food intolerance, and irritable bowel syndrome. Serology and histology also have limitations.

Diagnostic strategy for suspected celiac disease.
GFD = gluten-free diet; HLA = human leukocyte antigen; IgA = immunoglobulin A; IgG = immunoglobulin G; TTG = tissue transglutaminase
Serology
Testing for CD should begin with a TTG-IgA antibody and a total IgA level. The TTG-IgA has about 95% sensitivity and specificity.6,9 The higher the TTG-IgA titer, the more likely the result is a true positive. The total IgA level is valuable because patients with CD have an increased risk of having IgA deficiency and a falsely low TTG-IgA. If a patient is found to be IgA-deficient with a low TTG-IgA, then the sensitivity and specificity of TTG-IgG becomes excellent, making it the best antibody test to order next.10
A positive TTG-IgA or TTG-IgG result is an indication for upper endoscopy with multiple biopsies of the duodenum, specifically 1 or 2 from the bulb and 4 or more from the distal duodenum.6 Use of comprehensive CD panels is discouraged as they sacrifice considerable specificity for minimal added sensitivity. Further, interpretation of mixed results poses a challenge that can result in overdiagnosis and unnecessary testing, including invasive and costly endoscopy.
Among the limitations of serologic testing, sensitivity decreases significantly in patients who are on a gluten-free diet.11 Moreover, some patients have seronegative CD. If the index of suspicion for CD is sufficiently high, further evaluation is recommended despite negative serology.6
Biopsy and histopathology
The best next step in patients with suspected CD is referral to a gastroenterologist for endoscopic small-bowel biopsy to establish the diagnosis and rule out alternative diagnoses.6 There has been impressive interest and success in validating the confirmation of CD diagnosis without biopsy, particularly in children with concordantly positive, high-titer antibodies (ie, > 10 times the upper limit of normal for TTG-IgA), but this strategy is not yet recommended for adults. Typical confirmatory biopsy results are notable for increased intraepithelial lymphocytes, crypt hyperplasia, and villous atrophy as described by the Marsh or the Corazza and Villanacci criteria.12–14 Biopsy may be considered in a seronegative patient if the index of suspicion for CD remains high, as in patients with chronic diarrhea and evidence of malabsorption, in patients with gluten intolerance and other features of CD, or in symptomatic patients with a family history of CD.
Biopsy has limitations. Histologic abnormalities that correlate with CD can be patchy. There can be interprovider (gastroenterologist) variability in obtaining biopsies or in reading biopsies (pathologist) under a microscope. The results can also be equivocal in the presence of only 1 or 2 of the typical histologic features noted above: for example, CD is confirmed in only 10% of patients with isolated increased intraepithelial lymphocytes. The specificity of the biopsy increases if villous atrophy is identified, but it remains limited. Many enteropathies can mimic CD on biopsy, including autoimmune enteropathy, common variable immunodeficiency, and olmesartan-associated enteropathy.12 As with serology, the sensitivity of the biopsy decreases significantly in patients already on a gluten-free diet. Lastly, endoscopic biopsy is an invasive procedure with procedure-related risks.
Role of genetic testing
CD occurs only in individuals who are genetically predisposed. The genetic permissiveness for CD is human leukocyte antigen (HLA)-DQ2/DQ8. However, genetic testing has no role in the routine initial diagnosis of CD as it has little positive predictive value for CD. HLA-DQ2/DQ8 can be found in about 30% of the general population.15 The utility of genetic testing is its high negative predictive value: if a patient is negative for HLA-DQ2/DQ8, then CD can be ruled out, with rare exceptions.15 Genetic testing can be useful in patients who have discrepant clinical, serologic, and histologic findings. It can also be useful in patients on a gluten-free diet in whom the diagnosis of CD is questioned (Figure 1).
LONG-TERM FOLLOW-UP
CD is a chronic disorder with significant morbidity and mortality that can be obviated with gluten avoidance. Treatment is a lifelong gluten-free diet with regular medical and dietitian follow-up. Ideally, patients are referred to a center that specializes in the care of CD with an integrated multidisciplinary team that includes gastroenterologists, gastrointestinal pathologists, and dietitians with expertise in the gluten-free diet. Patients should be monitored for dietary adherence, serologic and histologic improvement, symptom resolution, and early detection of associated complications over time. Monitoring for improvement beyond symptom resolution can be accomplished by checking serology at 3 to 6 months, then every 6 months until seroconversion, and then annually.6 Recent guidelines suggest considering intestinal healing as a goal that can be assessed by follow-up intestinal biopsy after 2 years on a gluten-free diet.6
DISCLOSURES
Dr. Jansson-Knodell has disclosed ownership interest (stock, stock options in a publicly owned company) for ClearPoint Neuro, DarioHealth, Derm-Tech, DiaMedica Therapeutics, Exact Sciences, Inari Medical, Nano-X Imaging, Outset Medical, PAVmed, and Transmedics. The other authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2023 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}