


My 68-year-old patient is hospitalized for treatment of community-acquired pneumonia. There is no history of hypertension, but at a 2 AM check of vital signs, the patient’s supine blood pressure (BP) was 178/96 mm Hg. Heart rate is 68 beats per minute, respiratory rate 16 breaths per minute, and oxygen saturation 96% on oxygen delivered by nasal cannula at 2 L per minute. There is no evidence of acute end-organ damage. Do I need to treat this patient’s elevated BP?
In this hospitalized patient, antihypertensive treatment should not be considered without evaluating for changes in the orthostatic BP.
Inpatients’ vital signs are most commonly checked with the patient supine at various degrees of head-of-bed elevation, despite guidelines recommending against this technique (Table 1).1,2 A study showed that 50% to 70% of inpatients have at least 1 elevated BP measurement (> 140/90 mm Hg) during their hospitalization.3 Several aspects of elevated supine BP should be considered.
Criteria for blood pressure (BP) measurement
In the nonacute setting, BP measurement done in the supine and seated positions gives small but statistically different readings, with diastolic BP 5 mm Hg higher in the seated position and systolic BP 8 mm Hg higher in the supine position.1 In the hospital setting, several factors not associated with long-term consequences may cause elevated BP. These elevations have been termed reactive rather than significant.4,5 Most important, the hospitalized patient should be evaluated for orthostatic changes before treatment is considered.
A sequence of steps is appropriate for our patient with supine pressure of 178/96 mm Hg:
Confirm the pressure in the seated position
If BP elevation is confirmed, then determine whether the patient has a preexisting diagnosis of hypertension and is receiving pharmacologic treatment; if the patient is already being treated for hypertension, then in-hospital intravenous treatment or intensification of the oral regimen is associated with more adverse events and worse outcomes4,5
If the patient is not being treated, the elevated value should be noted and follow-up guided by standard recommendations2
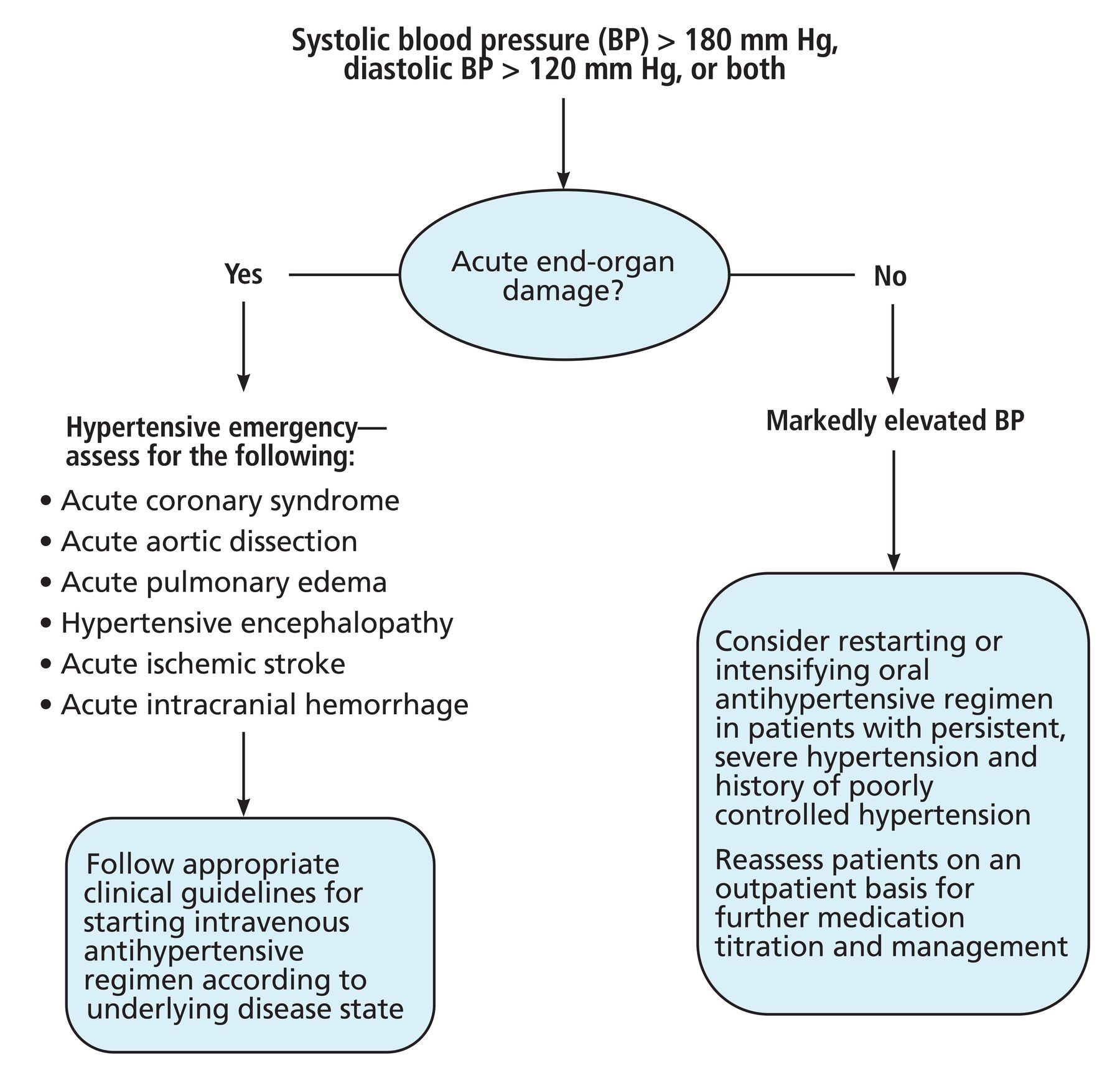
The absence of acute end-organ damage should also be noted (eg, no evidence of acute coronary syndrome, aortic dissection, pulmonary edema, hypertensive encephalopathy, ischemic stroke, or intracranial hemorrhage).
WHAT IS ORTHOSTATIC HYPOTENSION?
Orthostatic hypotension is sustained reduction of systolic BP of 20 mm Hg or more or diastolic BP of 10 mm Hg or more, or both, within 3 minutes of standing.6 In the standing position, blood pools in gravity-dependent body compartments, resulting in reduced venous return, cardiac output, and BP. In healthy patients, these posture-induced hemodynamic alterations precipitate compensatory sympathetic activation to increase peripheral vascular resistance and cardiac output.6,7
Orthostatic hypotension may be neurogenic or nonneurogenic; the former is associated with greater morbidity and mortality.6 Neurogenic orthostatic hypotension is often present in patients with dysfunction of the compensatory autonomic reaction. Reflexive increases in sympathetic neurocirculatory tone in these patients fail to compensate for decreased venous return to the heart, and, as a result, the postural response of the heart rate is insufficient to maintain BP.6,7
Neurogenic orthostatic hypotension can often be attributed to age-related degeneration of sympathetic output. It is also prominent in neurodegenerative disorders such as Parkinson disease, multiple system atrophy, and peripheral neuropathic disorders such as diabetes mellitus, amyloidosis, and human immunodeficiency virus infection.7,8 Conversely, nonneurogenic orthostatic hypotension may be seen in patients with hypovolemia, heart failure, severe venous stasis, and chronic illness with deconditioning, or it may be related to medications.8,9
NEXT STEPS: 3 SCENARIOS
No history of hypertension, no confirmed orthostatic hypotension
If the patient does not have a history of hypertension and does not have orthostatic hypotension, the first step is to recheck the patient’s BP in the seated position. Causes for reactive BP elevation such as pain, anxiety, urinary retention, or withdrawal from medications or substance use should be considered. Ultimately, achieving complete BP control during an acute hospitalization is not an appropriate goal, and in-hospital BP readings of 140/90 mm Hg or higher should not suffice to label a patient as hypertensive. Indeed, in the absence of acute end-organ damage, treating isolated inpatient hypertension may lead to harm.4,5 Instead, note the elevated reading and follow current guidelines for detecting high BP in the outpatient setting.2
History of hypertension, on medical therapy, no orthostatic hypotension
The benefits of controlling chronic hypertension in the outpatient setting, including reduction in cardiovascular events and mortality, are well defined.1,2 In the inpatient setting, however, there is little role for intensification of the antihypertensive regimen or use of intravenous agents. In the absence of acute end-organ damage, use of intravenous medications for inpatient BP elevation should be discouraged. Intravenous medications may precipitate sudden drops in BP and have been associated with higher risk of adverse clinical outcomes such as acute kidney injury, cardiac injury, and transfer to an intensive care unit.5
There is rarely an indication to intensify an established oral regimen for BP control in the inpatient setting. Observational studies suggest patients discharged with intensification did not experience better BP control in the following year.4 However, the question of whether to treat elevated BP in the hospital setting depends on context. Figure 1 identifies situations in which inpatient antihypertensive treatment may be warranted.2,4,5 Regardless, these patients require outpatient BP follow-up.

Supine hypertension, confirmed orthostatic hypotension
In established orthostatic hypotension, the next step is evaluation for reversible causes; the most common are hypovolemia and drug effects.6 In the absence of reversible causes, the patient should be evaluated for supine hypertension with orthostatic hypotension. This hemodynamic dichotomy poses a unique therapeutic challenge, as pharmacologic treatment to normalize standing BP frequently worsens supine hypertension and vice versa.7 Patients with autonomic dysfunction often experience supine hypertension because they lack baroreceptor function that buffers changes in BP in both directions.6 There are no epidemiologic data on the cardiovascular consequences of isolated supine hypertension.10
APPROACH TO ISOLATED SUPINE HYPERTENSION
In isolated supine hypertension, BP is elevated at night and often low-normal during the day. Therefore, the average BP over a 24-hour period may be only moderately elevated, even in patients who have severe supine hypertension. Pharmacologic treatment of supine hypertension may increase fall risk during nocturnal ambulation, as many patients with autonomic insufficiency also experience nocturia. Conversely, emerging studies suggest that supine hypertension may be associated with end-organ dysfunction parameters such as left ventricular hypertrophy, increased arterial stiffness, increased carotid intima-media thickness, and microalbuminuria.9,10 Ultimately, there is insufficient evidence to assess risk or prognostic impact associated with supine hypertension independently of the associated neurogenic orthostatic hypotension.9
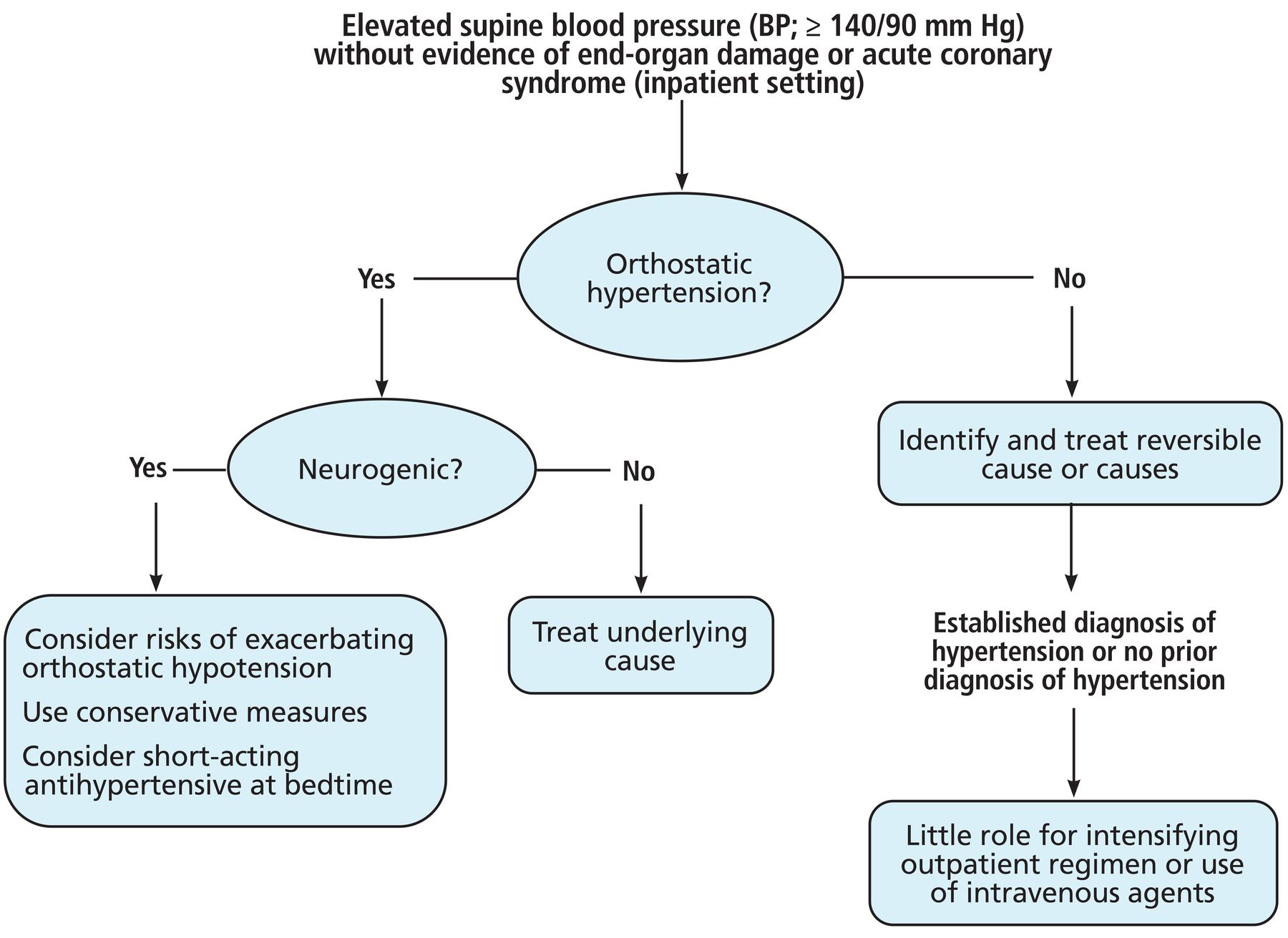
Supine BP lower than 180/110 mm Hg in the setting of orthostatic hypotension and in the absence of acute end-organ damage should be monitored, but treatment is not warranted. It may respond to conservative measures, such as small, frequent meals to avoid postprandial hypotension and nocturnal head-of-bed elevation (6–7 cm, or 30 degrees).9 For recurrent higher BP measurements, clinicians may consider a short-acting antihypertensive agent before bedtime, such as captopril, clonidine, hydralazine, or nitroglycerin patch.6,8 The potential benefits of antihypertensive medications must be balanced against the risks associated with side effects on a case-by-case basis.
THE BOTTOM LINE
Supine hypertension in a hospitalized patient who is asymptomatic, has no acute end-organ damage, and was admitted with noncardiovascular diagnoses usually does not require treatment with intravenous agents or intensification of an oral antihypertensive regimen. There is benefit to evaluating for orthostatic hypotension, however, because identifying orthostatic changes can have a major impact on the safety of acute treatment (Figure 2).6–10 Persistently elevated BP in inpatient settings warrants close outpatient follow-up after the patient recovers from their acute illness.

DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2025 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.