


Article Figures & Data
Figures
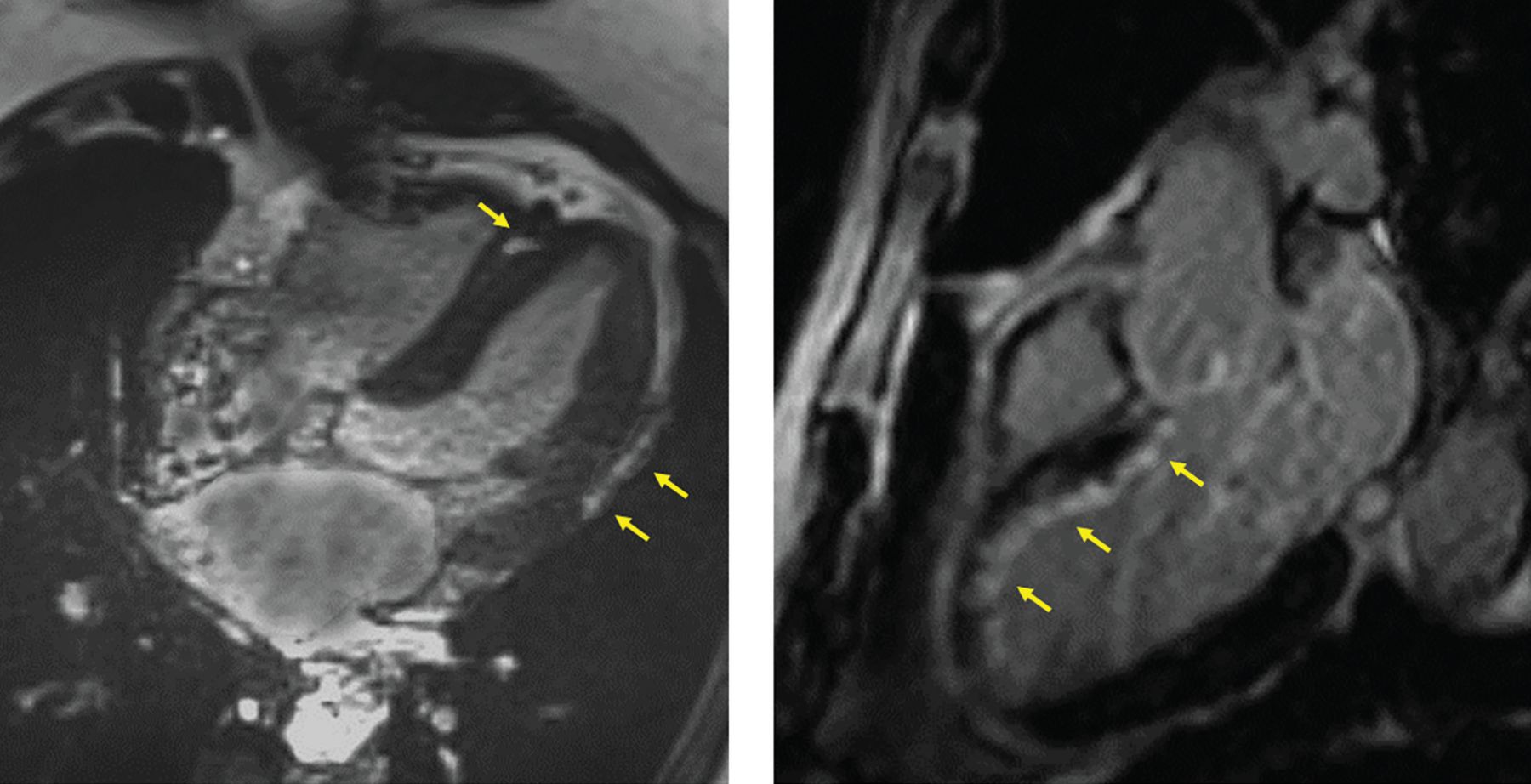
- Figure 1
Cardiac magnetic resonance imaging can reliably distinguish between myocarditis and coronary ischemic events in patients presenting with myocardial infarction with nonobstructive coronary arteries. Left panel, gadolinium enhancement (arrows) in the middle of the myocardium in the septum and below the epicardium in the lateral wall is a distribution pattern consistent with inflammatory disease or myocarditis. Right panel, enhancement (arrows) beneath the endocardium along the anterior septum and the anterior apex is a distribution consistent with an acute coronary injury likely originating from disease of the left anterior descending artery.
- Figure 2
Optical coherence tomography can define the underlying pathophysiology of the coronary event in myocardial infarction with nonobstructive coronary arteries. (A) Relatively mild angiographic disease of the proximal left anterior descending artery (arrow) in a patient with acute chest pain, abnormal biomarkers, and anterior T-wave inversions. (B) Optical coherence tomography demonstrates significant luminal narrowing and intraluminal thrombosis (asterisk). In that frame, the thrombus is shielding underlying plaque structure, but a few millimeters distally (C), the thrombus is still apparent and there is a disruption of the underlying intima. (D) Further distally, some thrombus is adherent, and there is an ulcer crater (X) after release of plaque content downstream.
- Figure 3
Optical coherence tomography can define subtle findings beyond the resolution of angiography. In the left panel, angiography in a patient with myocardial infarction with nonobstructive coronary arteries shows minimal haziness in the proximal circumflex artery (arrow). In the right panel, optical coherence tomography demonstrates a small thrombus with intact underlying plaque, representing plaque erosion.
- Figure 4
Provocative acetylcholine testing for coronary spasm. In the left panel, a young female patient with a long history of smoking presenting with myocardial infarction with nonobstructive coronary arteries has mild luminal irregularities in the left anterior descending artery. The right panel shows that intracoronary injection of escalating doses of acetylcholine provokes anginal symptoms, ST depression in precordial leads, and epicardial spasm in the mid segment of the anterior descending artery (arrows). Calcium channel blockers, nitrates, or both can be used to control spasm and vasospastic angina, and aggressive risk factor control is also needed.
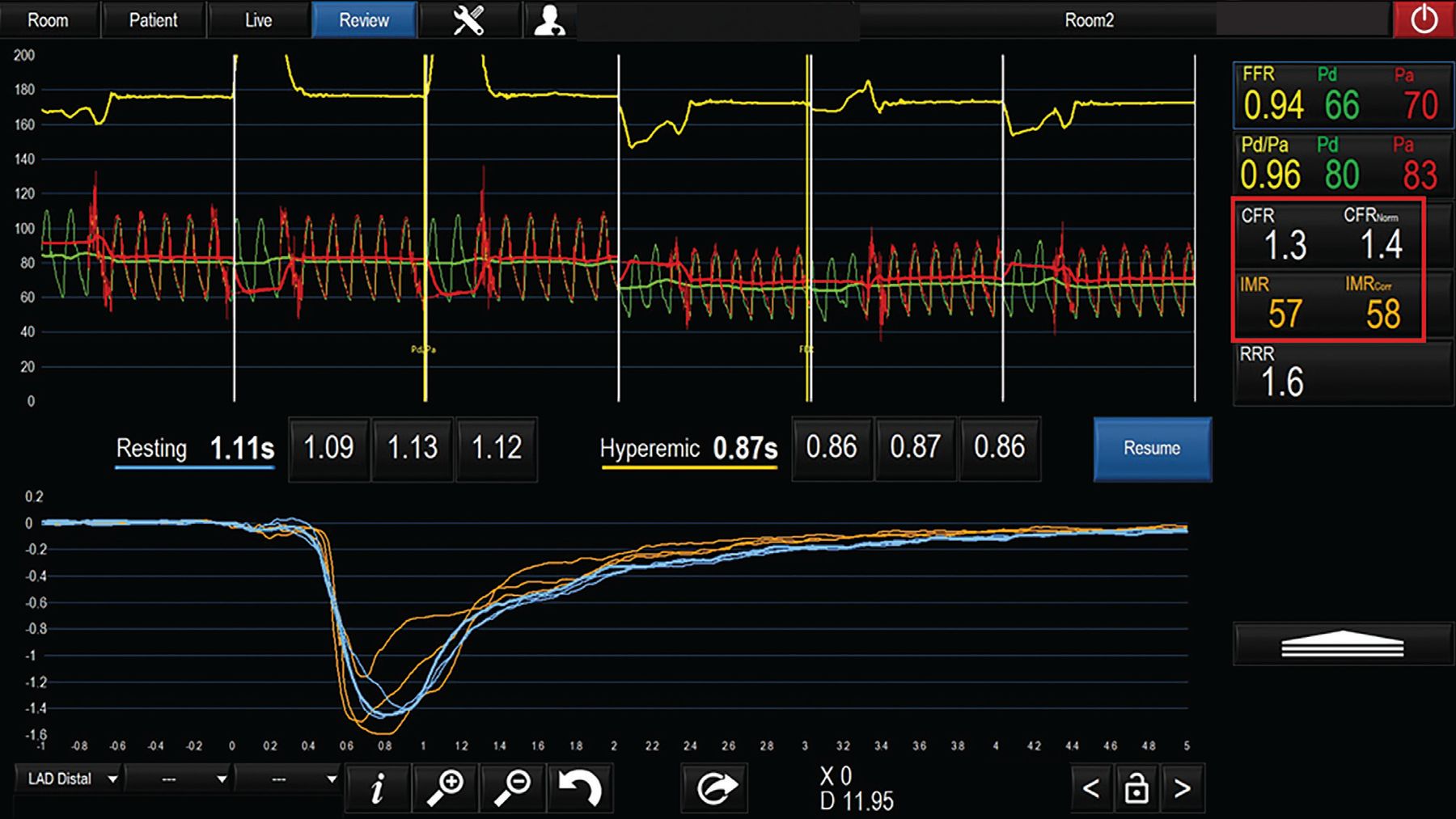
- Figure 5
Microvascular testing using thermodilution for assessment of coronary flow reserve (CFR). A patient presenting with myocardial infarction with nonobstructive coronary arteries and giving a history of exertional angina has no evidence of obstructive lesions. Thermodilution assessment based on transit time at rest and with hyperemia reveals abnormally low CFR and a high index of microcirculatory resistance (IMR; abnormal values in red box). Microvascular angina is diagnosed, and the patient can be treated with beta-blockers and ranolazine in addition to risk factor management.
FFR = fractional flow reserve; Pd = pressure measured distal to the stenosis; Pa = aortic pressure; RRR = resistive reserve ratio





In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- INVASIVE VS NONINVASIVE IMAGING
- MINOCA IS A WORKING DIAGNOSIS THAT NEEDS TO BE NARROWED DOWN
- CARDIAC MRI CAN POINT TO ETIOLOGY
- ADVANTAGES OF INVASIVE ANGIOGRAPHY AND INTRAVASCULAR IMAGING
- BEYOND IMAGING: TESTING FOR VASOSPASM AND MICROVASCULAR DYSFUNCTION
- TREATMENT SHOULD BE INDIVIDUALIZED
- NOVEL TOOLS ARE IMPROVING DIAGNOSIS AND TREATMENT
- DISCLOSURES
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.