


A 69-year-old man was referred to our hospital with a 6-month history of progressive swelling in the right middle finger without systemic symptoms. There was no previous trauma or surgery to the finger. The patient had previously been diagnosed with rheumatoid arthritis treated with methotrexate and hypertension treated with cilnidipine (a calcium channel blocker).
Physical examination revealed non-tender, sausage-like swelling of the right middle finger (Figure 1) with no nail abnormality or rash suggestive of psoriasis. Laboratory testing revealed a white blood cell count of 5.4 × 109/L (reference range 4.5–10.9) and a C-reactive protein level of 0.07 mg/dL (reference range 0.0–0.5). Hand radiography revealed soft-tissue swelling of the right middle finger without joint erosions or periostitis.

At presentation, the patient’s right middle finger was swollen, with a sausage-like appearance.
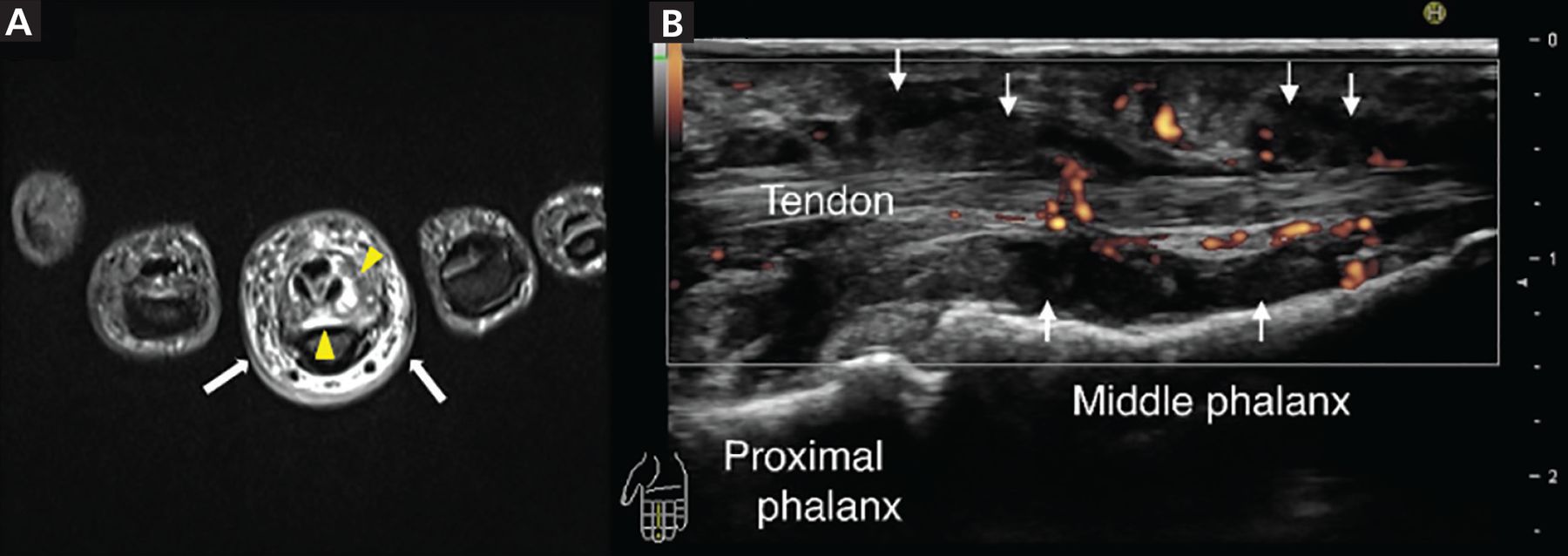
Magnetic resonance imaging (MRI) revealed soft-tissue swelling and thickening around the digital flexor tendon showing high intensity on short time inversion recovery (Figure 2A), and ultrasonography revealed low echoic area and power Doppler signals around the digital flexor tendon (Figure 2B), consistent with inflammation. Dactylitis is rare in patients with rheumatoid arthritis, and thus, the examination differed from that of typical rheumatoid arthritis. The patient did not show signs of other inflammatory diseases associated with dactylitis. We performed a biopsy around the digital flexor tendon of the affected finger to exclude infection.

(A) Axial magnetic resonance imaging set on short time inversion recovery showed a high signal around the digital flexor tendon of the right middle finger (yellow arrowheads) and in the subcutaneous tissue (white arrows). (B) Ultrasonography of the right middle finger (sagittal view) showed a low echoic area (white arrows) and power Doppler signals around the digital flexor tendon.
Histology revealed exudative synovitis with lymphocyte and plasma cell infiltration. Tissue culture initially yielded no bacteria; however, mycobacterial culture was positive for Mycobacterium intracellulare. The patient was diagnosed with dactylitis due to M intracellulare infection and treated with rifampin, ethambutol, and clarithromycin. The finger swelling markedly improved over 6 months.
DACTYLITIS
Dactylitis is the inflammation of a finger or toe with swelling of the entire digit rather than just a knuckle joint.1 Dactylitis can be classified based on the involved tissue of the digit, ie, bone only, bone and soft tissue, or soft tissue only. In addition, dactylitis may be classified according to the etiology as noninflammatory, inflammatory infectious, and inflammatory noninfectious.1
Spondyloarthritis dactylitis has been described as sausage-like in appearance and involves pain and swelling of the fingers or toes, mostly along the flexor tendons.1 Related disorders include psoriatic arthritis, ankylosing spondylitis, enteropathic arthritis, and reactive arthritis.1
MRI and ultrasonography2–4 show an increase in the volar bone-to-skin distance in dactylitic fingers that can be due to synovial thickening around the flexor tendons and may also show fluid collection in the tendon sheaths, indicating flexor tenosynovitis and adjacent soft-tissue swelling with small-joint synovitis.2–4
Although rare, tuberculous dactylitis can be the result of extrapulmonary tuberculosis with involvement of the digit and soft tissue.5 Radiographs typically show bone erosion (spina ventosa),6 and MRI shows that the lesion often extends to the soft tissue of the digit through cortical defects forming a sinus tract.5
The differential diagnosis of dactylitis includes syphilitic dactylitis, a manifestation of congenital syphilis; sarcoid dactylitis, with infiltration of the phalangeal soft tissue by noncaseating granulomas; sickle cell dactylitis, or “hand-foot syndrome,” associated with infarction of bone marrow, usually in children; and reactive distal dactylitis of the anterior fat pad, mostly due to group A beta-hemolytic streptococci.1 Dactylitis can also be associated with gout, resulting from deposition of monosodium urate crystals in the soft tissue of the involved digits1 and from infection.
MYCOBACTERIUM INTRACELLULARE INFECTION OF A FINGER
Nontuberculous mycobacteria (NTM) cause pulmonary disease in 90% of cases.7 NTM musculoskeletal infection is uncommon,7–9 but NTM tenosynovitis has been repeatedly reported.10–12 Wrists and hands are the most frequently reported sites of tenosynovitis, and some have described the presence of multiple granulomatous “rice bodies.”10–13 As seen in our patient, M intracellulare can infect a single digit and cause tenosynovitis-associated dactylitis.
Use of anti-tumor necrosis factor agents, high-dose corticosteroids, leflunomide, cyclophosphamide, azathioprine, cyclosporine, mycophenolate, and chlorambucil have been associated with NTM infection of soft tissue or joints.14
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}