


Article Figures & Data
Figures
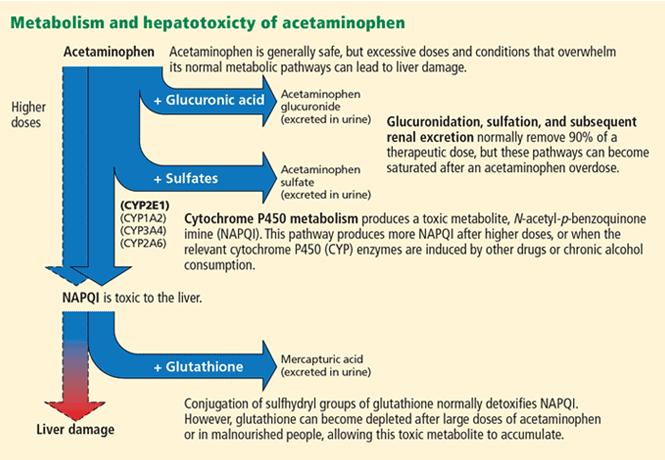
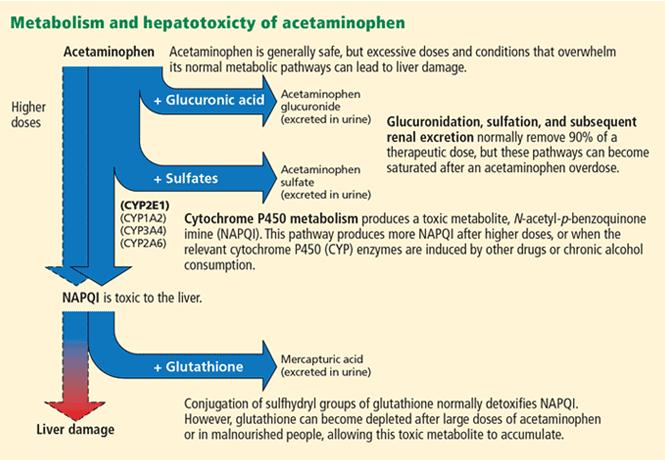
- FIGURE 1
Reprinted from Schilling A, Corey R, Leonard M, Eghtesad B. Acetaminophen: old drug, new warnings. Cleve Clin J Med 2010; 77:19–27.

Tables
Acetaminophen is used to treat pain and fever. Overall, it is safe, but if you take too much (more than 4,000 mg per day), it can damage the liver. If you are taking it, please do the following: Read the label. Many medicines contain acetaminophen, so you could be taking too much without knowing. Don’t drink. Drinking alcohol increases the likelihood of acetaminophen-induced liver toxicity. Get help. If you or your child may have taken too much acetaminophen, call the American Association of Poison Control Centers hotline at 1-800-222-1222 right away. Keep acetaminophen (and all drugs) out of the hands of children. - TABLE 2
Mechanism of toxicity of drugs and herbal supplements known to cause acute liver failure
Drug or supplement Pattern of injury Terbinafine Cholestatic and mixed Sulfasalazine Cholestatic or mixed Trimethoprim-sulfamethoxazole Cholestatic or mixed Isoniazid Hepatocellular Carbamazepine Hepatocellar, cholestatic, or mixed Valproic acid Hepatocellular Phenytoin Hepatocellular, cholestatic, or mixed Herbalife Hepatocellular Hydroxycut Hepatocellular, cholestatic, or mixed Kava kava Hepatocellular OxyElite Pro Hepatocellular Transfer the patient to the intensive care unit in a tertiary care center with facilities for liver transplant Neurologic complications Grade 2–3 encephalopathy: order computed tomography of the brain to rule out secondary causes of encephalopathy; avoid hyponatremia and use of sedatives Grade 3–4 encephalopathy: intubate; elevate the head end of bed to 30 degrees; consider giving mannitol or hypertonic saline Infectious complications Give a broad-spectrum antibiotic if infection is suspected, and add an antifungal agent if there is no improvement with initial antibiotic coverage Gastrointestinal complications Give a histamine H2 receptor blocker or a proton pump inhibitor to prevent upper gastrointestinal bleeding Determining the cause of acute liver failure Obtain a thorough history of ingestion of drugs from the patient and family Laboratory testing, including toxicology screen, acetaminophen or acetaminophen-protein adduct levels; serologic testing for hepatitis A, hepatitis B, hepatitis C, herpes simplex virus, autoimmune hepatitis, and serum and urine copper and serum ceruloplasmin levels Factor King’s College criteria37,66,67 Clichy criteria66,69 MELD score68 APACHE score Age Yes Yes No Yes Cause of acute liver failure Yes No No No Presence of encephalopathy Yes Yes No No Presence of coagulopathy Yes Yes Yes No Serum bilirubin level Yes No Yes No Serum creatinine level Yes No Yes Yes Sensitivity to predict poor outcome without liver transplant Acetaminophen-induced acute liver failure 69% 75% 60% 68% Acute liver failure from other causes 68% 69% 87% Specificity to predict poor outcome without liver transplant Acetaminophen-induced acute liver failure 82% 56% 69% 87% Acute liver failure from other causes 92% 50% 65% APACHE II = Acute Physiology and Chronic Health Evaluation II; MELD = Model for End-State Liver Disease




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.