


Article Figures & Data
Figures
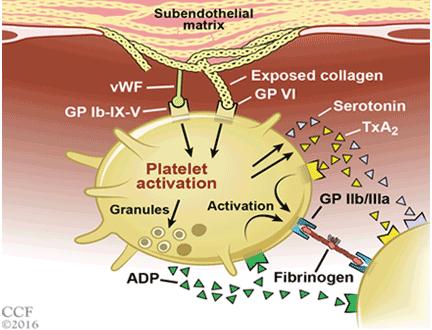
- FIGURE 1
The platelet aggregation cascade. Exposure of subendothelial matrix leads to adhesion of platelets to the vessel wall, activation, and aggregation.
ADP = adenosine diphosphate; GP = glycoprotein; TxA2 = thromboxane A2; vWF = von Willebrand factor
- FIGURE 2
Mechanism of action of antiplatelet agents.
AC = adenyl cyclase; cAMP = cyclic adenosine monophosphate; Ca2+ = calcium; CYP = cytochrome P450; Gs, Gi, Gq = G proteins; PDEIII = phosphodiesterase III, PGR, P2Y12, P2Y1, P2X1 = platelet receptors; PKA= protein kinase A; VASP = vasodilator-stimulated phosphoprotein; VASP-P = phosphorylated VASP


Tables
Drug Metabolic activation Reversibility Time to peak activity Elimination half-life Duration of effect Elimination Dosage Aspirin By esterases in gastrointestinal mucosa No 1–2 hours 3 hours 7–10 days Renal 162–325 mg loading dose, then 81–162 mg daily Clopidogrel By CYP450 No 2–6 hours 6 hours 5–7 days Renal and gastrointestinal 300–600 mg loading dose, then 75 mg daily Prasugrel By CYP450 No 0.5–4 hours 2–15 hours 5–9 days Renal and gastrointestinal 60 mg loading dose, then 10 mg daily Ticagrelor No Yes 0.5–2 hours 7–9 hours 3–5 days Gastrointestinal and renal 180 mg loading dose, then 90 mg twice a day Cangrelor No Yes 2–30 minutes 3–5 minutes 0–30 minutes Renal and gastrointestinal 4 μg/kg/min intravenous infusion - TABLE 2
ACC/AHA recommendations for initial antiplatelet therapy for patients with likely or definite non-ST-elevation myocardial infarction
Antiplatelet drug Initial therapy (class of recommendation, level of evidence)a Continued therapy (class of recommendation, level of evidence)a General recommendations for non-ST-elevation myocardial infarction Aspirin 162–325 mg of nonenteric coated aspirin for all patients promptly after presentation (I, A) 81–162 mg/day indefinitely as maintenance dose (I, A) P2Y12 inhibitors 300–600 mg loading dose clopidogrel in patients with gastrointestinal intolerance or aspirin hypersensitivity (I, B)
300–600 mg loading dose of clopidogrel or 180 mg loading dose of ticagrelor in addition to aspirin in patients treated with an early invasive or ischemiaguided strategy (I, B)
It is reasonable to use ticagrelor in preference to clopidogrel for patients treated with an early invasive or ischemia-guided strategy (IIa, B)Clopidogrel 75 mg/day as maintenance dose in patients with gastrointestinal intolerance or aspirin hypersensitivity (I, B)
Clopidogrel 75 mg/day or ticagrelor 90 mg twice daily in addition to aspirin as maintenance dose for up to 12 months in patients treated with an early invasive or ischemia-guided strategy (I, B)Recommendations for percutaneous coronary intervention (PCI) Aspirin 81–325 mg nonenteric coated aspirin before PCI in patients already taking aspirin (I, B)
325 mg nonenteric coated aspirin as soon as possible before PCI in patients not taking aspirin (I, B)81–325 mg/day to be continued indefinitely after PCI (I, B)
It is reasonable to use 81 mg/day in preference to a higher maintenance dose (IIa, B)P2Y12 inhibitors A loading dose before PCI in patients undergoing stenting (I, A):
Clopidogrel 300–60 mg (I, B) or
Prasugrel 60 mg (I, B) or
Ticagrelor 180 mg (I, B)
It is reasonable to use ticagrelor in preference to clopidogrel for patients treated with an early invasive strategy or coronary stenting (IIa, B)
It is reasonable to use prasugrel in preference to clopidogrel for patients who undergo PCI and are not at high risk of bleeding (IIa, B)
Prasugrel should not be given to patients with a history of stroke or transient ischemic attack (III, B)Maintenance dose to be continued for at least 12 months in patients receiving a bare-metal or drugeluting stent. Options include:
Clopidogrel 75 mg/day (I, B) or
Prasugrel 10 mg/day (I B) or
Ticagrelor 90 mg twice a day (I, B)
If the morbidity of bleeding outweighs the anticipated benefit of duration of P2Y12 inhibitor therapy after stent implantation, early discontinuation (ie, < 12 months) of P2Y12 therapy is reasonable (IIa, C)
Continuation of dual antiplatelet therapy beyond 12 months may be considered in patients undergoing stent implantation (IIb, C)↵a Class of recommendation: I = treatment should be given, IIa = treatment is reasonable, IIb = treatment may be considered, III = treatment is not recommended or may harm. Level of evidence: A = multiple populations evaluated, B = limited populations evaluated, C = very limited populations evaluated.
Based on information in reference 2.
- TABLE 3
ACC/AHA recommendations for antiplatelet therapy for patients with ST-elevation myocardial infarction (STEMI)
Antiplateletdrug Initial therapy (class of recommendation, level of evidence)a Continued therapy (class of recommendation, level of evidence)a Antiplatelet therapy adjunctive to primary percutaneous coronary intervention (PCI) Aspirin 162–325 mg should be given to all patients before primary PCI (I, B) 81–325 mg maintenance dose indefinitely (I, A)
81 mg as preferred maintenance dose with ticagrelor (I, B)P2Y12 inhibitors Loading dose should be given as early as possible or at the time of primary PCI in patients with STEMI.
Options:
Clopidogrel 300–600 mg (I, B)
Prasugrel 60 mg (I, B)
Ticagrelor 180 mg (I, B)Maintenance dose should be continued for 1 year following a drug-eluting or bare metal stent placement.
Options:
Clopidogrel 75 mg daily (I, B)
Prasugrel 10 mg daily (I, B)
Ticagrelor 90 mg twice daily (I, B)Prasugrel should not be given to patients with a history of stroke or transient ischemic attack (III, B) Continuation of P2Y12 inhibitor beyond 1 year may be considered in patients with drug-eluting stent placement (IIb, C) Antiplatelet therapy adjunctive to PCI after fibrinolytic therapy Aspirin 162–325 mg should be given to all patients who receive fibrinolytic therapy (I, A) 81–325 mg maintenance dose indefinitely (I, A)
81 mg is preferred maintenance dose (IIa, B)P2Y12 inhibitors Clopidogrel loading dose based on age in all patients
who receive fibrinolytic therapy (I, A)
Age ≤ 75: 300 mg
Age > 75: 75 mgIf drug-eluting stent placed:
Continue P2Y12 inhibitor for at least 1 year with either:
Clopidogrel 75 mg daily (I, C)
Prasugrel 10 mg daily (IIa, B)For patients who received loading dose during fibrinolytic therapy: clopidogrel 75 mg daily without an additional loading dose (I, C) If bare-metal stent placedb:
Continue therapy for at least 30 days and up to 1 year with either of the following:
Clopidogrel 75 mg daily (I, C)
Prasugrel 10 mg daily (IIa, B)For patients who did not receive loading dose during fibrinolytic therapy: If PCI performed ≤ 24 hours after fibrinolytic therapy: clopidogrel 300 mg before or at the time of PCI (I, C) If PCI performed > 24 hours after fibrinolytic therapy: clopidogrel 600 mg before or at the time of PCI (I, C) If PCI performed > 24 hours after treatment with a fibrinspecific agent or > 48 hours after a non–fibrin-specific agent: prasugrel 60 mg at the time of PCI (IIa, B) Prasugrel should not be given to patients with a history of stroke or transient ischemic attack (III, B) ↵a Class of recommendation: I = treatment should be given, IIa = treatment is reasonable, IIb = treatment may be considered, III = treatment is not recommended or may harm. Level of evidence: A = multiple populations evaluated, B = limited populations evaluated, C = very limited populations evaluated.
↵b Balloon angioplasty without stent placement may be used in selected patients. It may be reasonable to provide P2Y12 inhibitor therapy to patients with ST-elevation myocardial infarction undergoing balloon angioplasty after fibrinolysis alone according to the recommendations listed for bare-metal stents (level of evidence C).
Based on information in reference 1.
- TABLE 4
Randomized controlled trials of extended dual antiplatelet therapy after stent placement
Trial (No. of patients) Design Follow-up Stent thrombosis (study vs control) MACE (study vs control) Bleeding events (study vs control Conclusion DAPT3 (9,961) DAPT vs aspirin alone beyond 12 months 18 months 0.4% vs 1.4%a 4.3% vs 5.9%a 2.5% vs 1.6%a DAPT > 1 year decreased risk of stent thrombosis and MACE ARCTIC–Interruption46 (1,259) DAPT vs aspirin alone beyond 12 months 17 months 0% vs 1% 4% vs 4% 1% vs < 0.5% No benefit of DAPT beyond 12 months DES-LATE47 (5,045) DAPT vs aspirin alone beyond 12 months 24 months 0.5% vs 0.3% 2.4 vs 2.6% 1.1% vs 1.4% No benefit of DAPT for 24 more months at end of 1 year CREDO20 (2,116) DAPT vs aspirin and placebo up to 12 months 12 months Not reported 8.5% vs 11.5%a 8.8% vs 6.7%a,b Significant benefit of DAPT vs placebo at 1 year OPTIMIZE42 (3,118) DAPT for 3 vs 12 months 12 months 0.3% vs 0.1% 2.6% vs 2.6% 0.2% vs 0.4% Noninferiority of 3 vs 12 months of DAPT RESET43 (2,117) DAPT for 3 vs 12 months 12 months 0.2% vs 0.3% 4.7% vs 4.7% 0.5% vs 1% Noninferiority of 3 vs 12 months DAPT EXCELLENT41 (1,493) DAPT for 6 vs 12 months 12 months 0.9% vs 0.1% 8% vs 8.5% 0.3% vs 0.6% Noninferiority of 6 vs 12 months of DAPT PRODIGY45 (1,970) DAPT for 6 vs 12 months 12 months 3.9% vs 4.7% 10.1% vs 10% 1.6% vs 0.6%a No significant benefit of 24 vs 6 months of DAPT with clopidogrel SECURITY40 (1,399) DAPT for 6 vs 12 months 24 months 0.3% vs 0.4% 4.5% vs 3.7% 0.2% vs 0.3% Noninferiority of 6 vs 12 months of DAPT ↵a P < .05.
DAPT = dual antiplatelet therapy; MACE = major adverse cardiac event




{kind=link}
{kind=link}
Jump to section
- Article
- ABSTRACT
- PLATELETS IN ACUTE CORONARY SYNDROMES AND STENT THROMBOSIS
- PERCUTANEOUS INTERVENTION, RESTENOSIS, AND STENT THROMBOSIS
- ANTIPLATELET AGENTS: MECHANISM OF ACTION
- WHY DUAL ANTIPLATELET THERAPY?
- RECOMMENDATIONS FOR DOSING
- WOULD SHORTER THERAPY AFTER STENTING WORK AS WELL?
- WOULD LONGER THERAPY BE BETTER?
- BALANCING RISK AND BENEFIT
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.