


Article Figures & Data
Figures
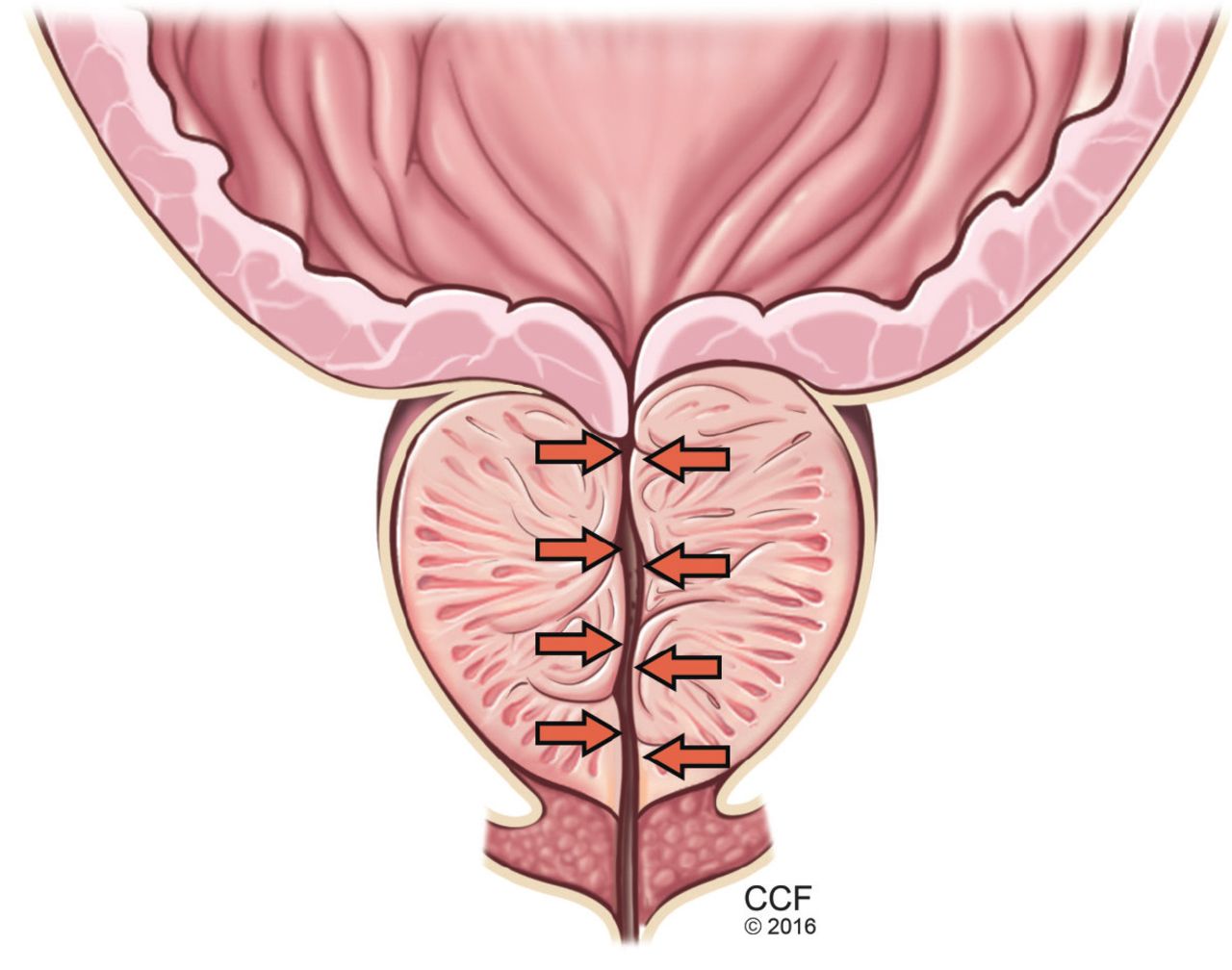
- FIGURE 1
The static component of benign prostatic hyperplasia and lower urinary tract symptoms, with hyperplasia leading to urethral compression.
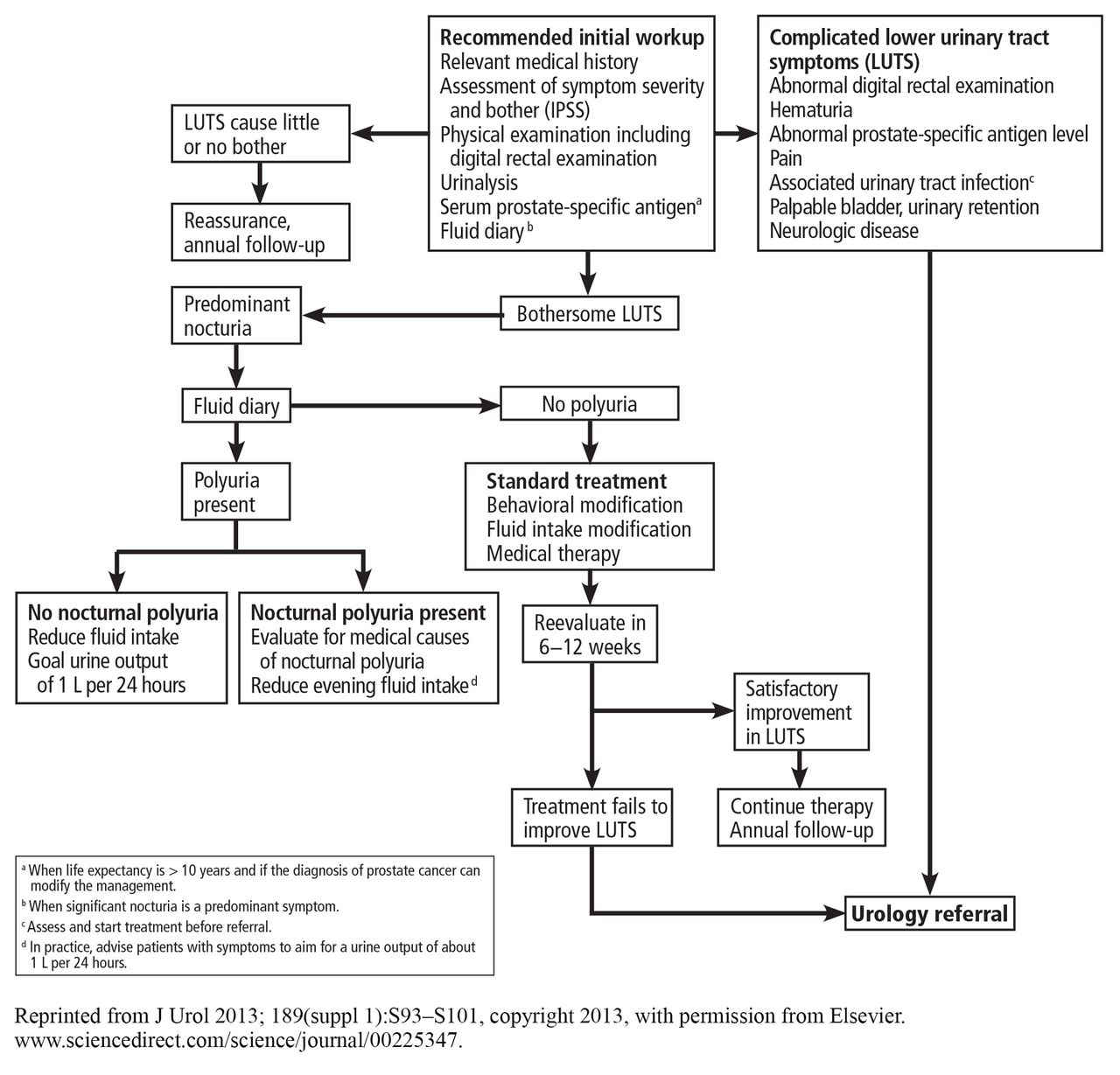
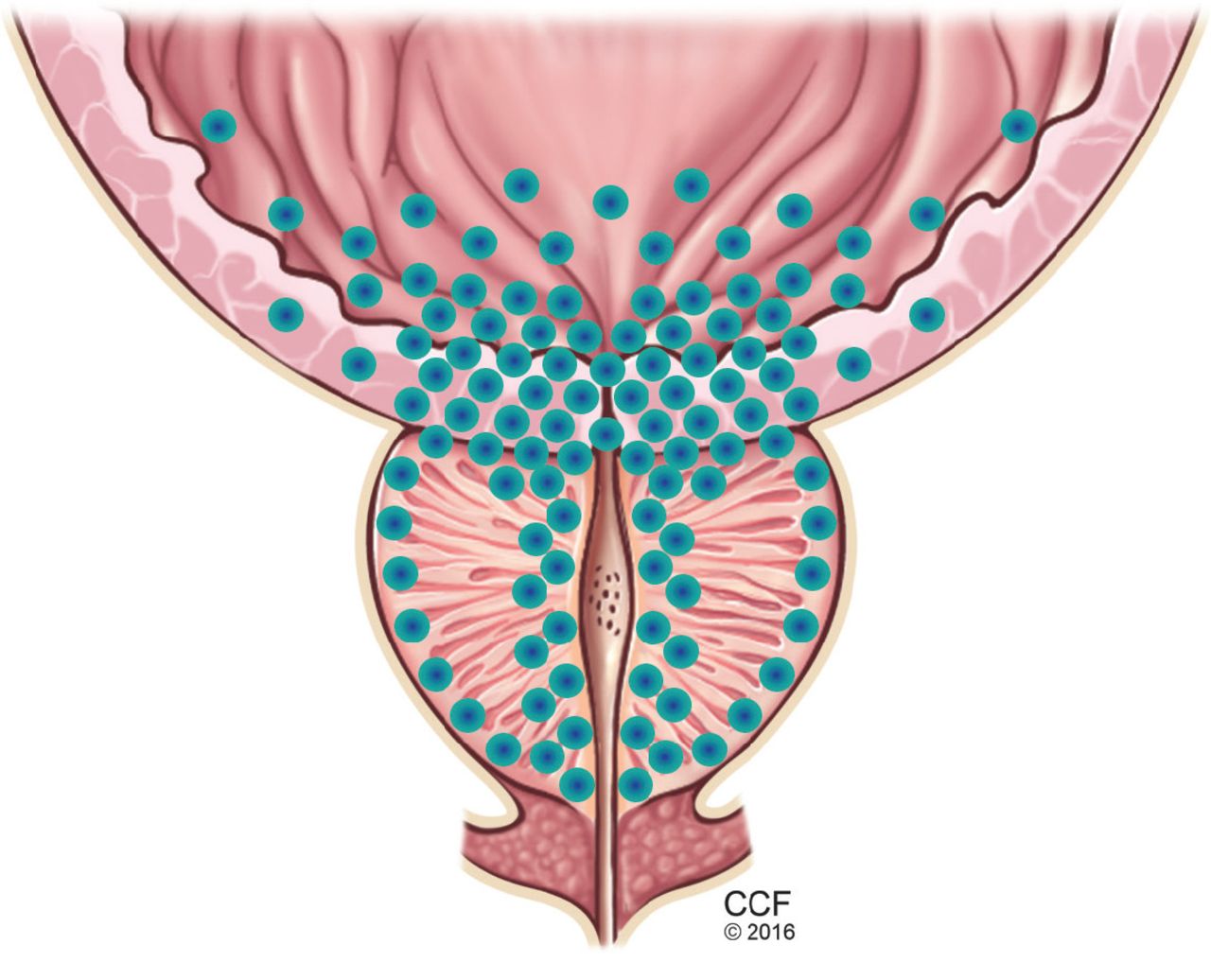
- FIGURE 2
The dynamic component of benign prostatic hyperplasia. The bladder outlet and prostate are richly supplied with alpha-1 receptors (their distribution represented by blue dots), which increase smooth muscle tone, promoting obstruction to the flow of urine. Alpha-1 adrenergic blockers counteract this effect.
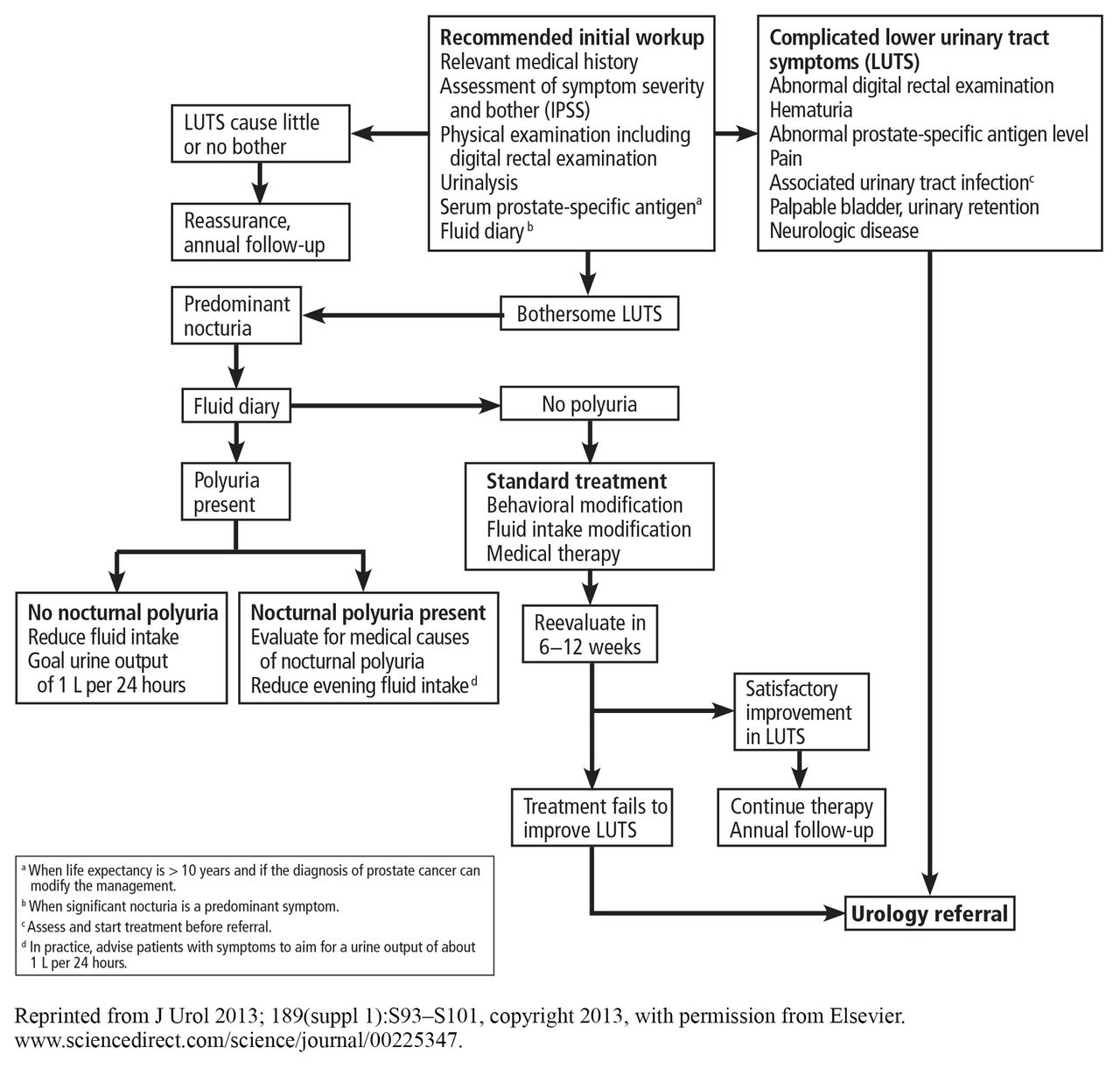
- FIGURE 3
An algorithm for diagnosing and managing benign prostatic hyperplasia.

Tables
Hematuria Recurrent urinary tract infection Prior urologic surgery Elevated prostate-specific antigen Bladder stone Abnormal digital rectal examination Clinical suspicion of a neurologic cause Urinary retention History of urinary instrumentation or trauma Lower urinary tract symptoms refractory to medical management Desire for urologic evaluation Drug class Drug Brand name Dosage form and strength Package size Brand name SWP Generic SWP Alpha-blockers Alfuzosin Uroxatral 10-mg capsules 100 capsules NA $421.78 Doxazosin Cardura 1-mg tablets 100 tablets NA $134.86 Silodosin Rapaflo 4-mg capsules(ER) 30 capsules $249.47 NA Tamsulosin Flomax 0.4-mg capsules (ER) 100 capsules NA $421.36 Terazosin Hytrin 1-mg capsules 100 capsules NA $160.50 5-Alpha reductase inhibitors Dutasteride Avodart 0.5-mg capsules 30 capsules $201.70 $181.53 Finasteride Proscar 5-mg tablets 100 tablets $558.65 $313.07 Phosphodiesterase-5 inhibitor Tadalafil Cialis 2.5-mg tablets 30 tablets $281.74 NA Anticholinergic Oxybutynin Ditropan 5-mg tablets 100 tablets N/A $76.03 Beta-3 agonist Mirabegron Myrbetriq 25-mg tablets (ER) 90 tablets $1,068.28 NA ER = extended-release; SWP = suggested wholesale price, as listed in Amerisource Bergen
Drug Titration required?a Dose range (mg) Difference in peak urinary flowb (mL/sec) Difference in IPSSb Terazosin28,29 Yes 2–10 +0.6 to +1.9 −1.0 to −4.0 Doxazosin30,31 Yes 1–8 +1.4 to +3.5 −2.1 to −4.7 Alfuzosin32,33 Noc 10 +0.9 to +1.8 −1.0 to −2.0 Tamsulosin34,35 No 0.4–0.8 +0.6 to +2.6 −1.3 to −3.2 Silodosin36 No 4–8 +0.8 to +1.4 −2.3 to −3.0 - TABLE 4
Absolute increase in incidence of the most common adverse effects of alpha-blockers compared with placebo
Adverse effect Terazosin28,29 Doxazosin30 Alfuzosin38 Tamsulosin34,35 Silodosin39 Dizziness 5.9% 15%–20% 2% 5% 0.6–2.1% Fatigue 4.6% 8%–10% — 2–3% — Peripheral edema 3.1% — — — — Orthostatic hypotension 1.4% 8% 0.7% — 1.1% Ejaculatory dysfunction 1.2% — — 6%–11% 22%–27% Transurethral resection of prostate (TURP) Transurethral microwave therapy Photovaporization of prostate Simple prostatectomy Technique description Endoscopic resection of the prostate under direct visualization using monopolar or bipolar loop electrocautery Ablation of the prostate using a specialized catheter with a microwave antenna Endoscopic vaporization of the prostate using high-powered laser energy Surgical removal of prostatic tissue using an open, laparoscopic, or robotic approach Anesthesia Spinal or general Local Spinal or general Spinal or general Typical postoperative catheterization 24–48 hours (longer if hematuria) Several days < 24 hours Several days Common complications Retrograde ejaculation
Blood loss anemia
Urinary tract infection
Urinary retention
Bladder neck contractureUrinary retention
Urinary tract infection
Retrograde ejaculationIrritative urinary symptoms
Hematuria
Urinary tract infectionHematuria
Blood loss anemia
Urinary tract infectionAdvantages Gold standard
Mean 70% reduction in International Prostate Symptom Score (IPSS) and mean 12-mL/sec improvement in peak urinary flow 1 year after surgeryOffice procedure
Same-day dischargeSafe to perform while on antiplatelet therapy
Can typically remove catheter and discharge home on day of surgery
Similar improvement in peak urinary flow and IPSS relative to TURPExcellent option for men with prostates > 75 g
Allows concurrent treatment of bladder diverticula or stones
Reduced morbidity with robotic approach
Similar improvement in peak urinary flow and IPSS relative to TURPDisadvantages Higher risk of hematuria than other surgical options
Often requires postoperative hospitalizationLess durable results, high rate of retreatment
Less symptom improvement than with other surgical therapies
Higher incidence of urinary retention requiring prolonged catheterization
Not available in all urology practicesRequires long operative time for large prostate volumes More invasive procedure with longer convalescence
Urologists experienced in this procedure not available in all practices
High rate of blood transfusion (lower risk with robotic approach)
Requires postoperative hospitalizationInformation from reference 50.



{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.