


ABSTRACT
To improve outcomes with robotically assisted mitral valve surgery, Cleveland Clinic conducted a study evaluating outcomes in 1,000 consecutive cases. Primary areas of interest were to determine whether increased surgical experience with robotic techniques improved outcomes and to identify opportunities that could improve procedural processes. Results showed that these surgeries were effective and safe in terms of improvements in procedure time, transfusion rates, stroke risk, number of mitral valve replacements, and number of conversions to sternotomy. The development and implementation of a patient-selection algorithm halfway through the study further improved outcomes by refining patient eligibility criteria. This study showed that use of a focused preoperative assessment with an algorithm-driven patient selection process combined with increased technical expertise can enhance outcomes with robotic mitral valve surgery.
Surgeon competence with robotic techniques, which can be improved through experience, is a key to improving outcomes.
This patient-selection algorithm provides an evidence-based approach to identifying patients who are the best candidates for the robotic approach.
This study showed that increased surgical competence and improved patient selection improved patient outcomes for the primary end points.
In the years since the introduction of robotically assisted mitral valve surgery, surgeons have looked for ways to improve techniques and procedures. A study from Cleveland Clinic presented at the American Association for Thoracic Surgery in 2016 assessed efficacy and safety outcomes associated with 1,000 consecutive robotically assisted mitral valve surgeries at Cleveland Clinic.1 The purpose of the study was to assess the clinical outcomes from these cases and analyze whether the outcomes changed over time as surgeons became more competent with robotic techniques. This analysis was also designed to identify procedural processes that improved outcomes during the trial.
STUDY METHODS
Data were collected from January 2006 through November 2013. Baseline characteristics showed a relatively young patient population, mostly male, with a reasonably preserved ejection fraction (Table 1).
Baseline characteristics
Nearly all cases (96%) were classified as degenerative mitral valve disease (N = 960). Of those, most had posterior leaflet prolapse (68%), about one-third (29%) had bileaflet prolapse, and only 3% had anterior leaflet involvement.
All surgeries were performed through right port incisions and used femoral cannulation for peripheral bypass. The aorta was occluded with either a Chit-wood transthoracic clamp or a balloon.
STUDY RESULTS
It is important to remember that with femoral artery perfusion, the blood flow is opposite to the normal direction; thus, it goes up the aorta into the head vessels, which presents its own risks and challenges. Also, during retrograde perfusion, there is a risk of dislodging atherosclerotic plaque leading to brain embolus and stroke.
Nevertheless, outcomes data showed that these procedures were safe, with just 1 death in the 1,000 cases (Table 2). There was an overall 1.4% stroke rate, with a 0.8% permanent stroke rate. Atrial fibrillation occurred in 18.9%, approximately 12% required a transfusion, and 2.5% needed re-exploration for bleeding.
Safety of robotically assisted mitral valve surgery
In these 1,000 cases, 997 were planned mitral valve repairs, 2 were mitral valve replacements, and 1 was resection of a mitral valve fibroelastoma. Results for the mitral valve repairs were excellent, with postoperative mitral regurgitation occurring in less than 1% of patients.
There were 20 conversions to sternotomy, mainly during the earlier stages of this study. Table 3 lists the causes of conversions. Most were from residual mitral valve regurgitation, bleeding, or exposure difficulties.
Cases converted to sternotomy (N = 20)
PROCEDURAL IMPROVEMENTS
A primary point of interest was to identify procedural improvements that occurred during the course of the study. The areas evaluated in robotically assisted mitral valve surgery were the efficacy of the procedure in time, transfusion rates, stroke risk, how many mitral valve replacements occurred, and how many required conversion to sternotomy. These were assessed to determine whether surgical experience resulted in improvement.
Results showed that those efficiencies improved during the study. Cardiopulmonary bypass time decreased from about 140 minutes to 130 minutes. Cross-clamp time improved more dramatically from about 110 minutes to 90 minutes. And the percentage of cases requiring postoperative or intraoperative blood transfusion improved from about 24% to 10%.
PATIENT SELECTION CRITERIA: ALGORITHM
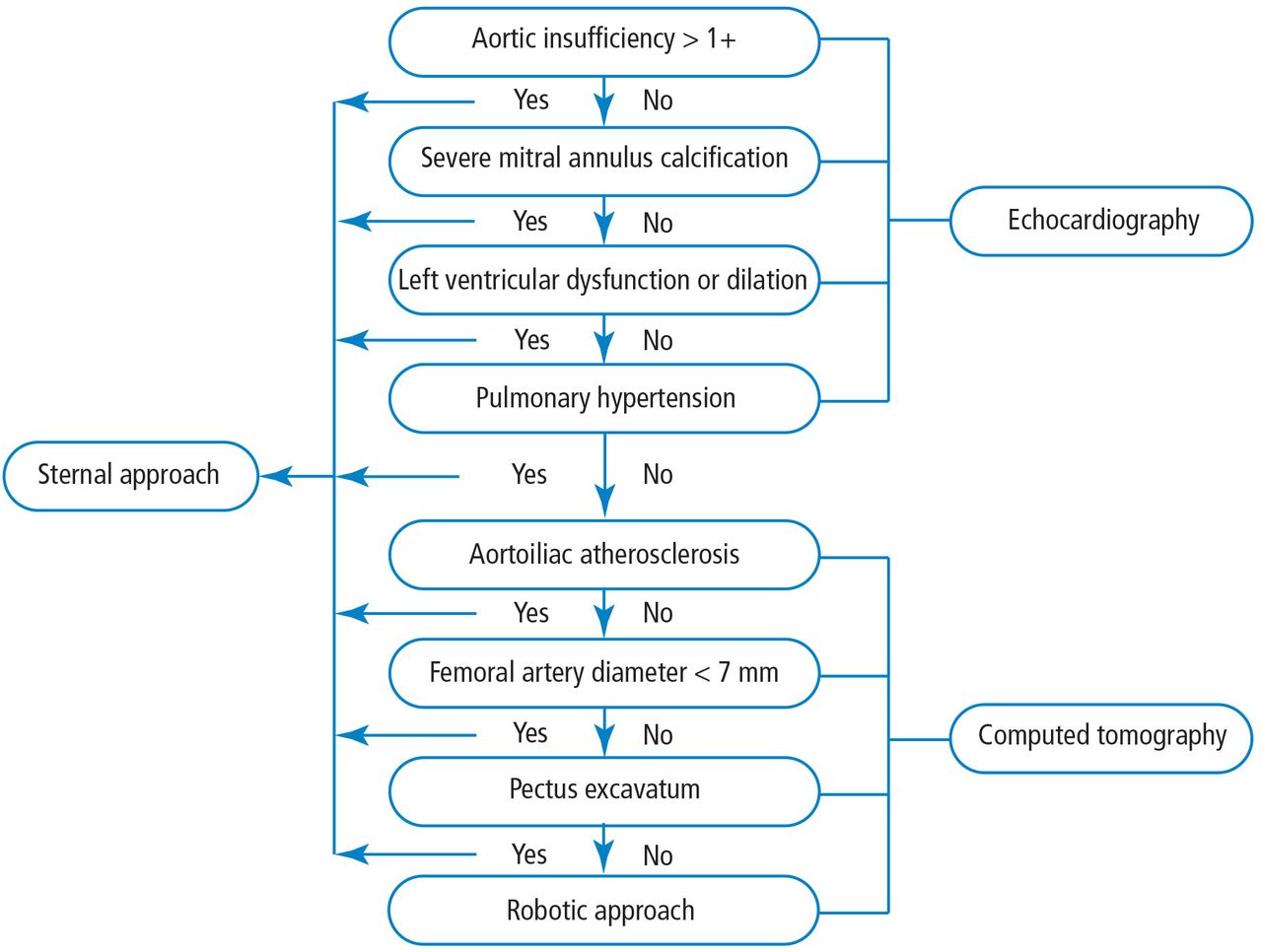
After 500 cases, enough data had been collected to create an algorithm for determining which patients would be eligible for mitral valve repair via the robotic approach vs a sternotomy-based approach. Use of the algorithm (Figure 1) relies on results from echocardiography and computed tomography (CT) for most of the selection process. Echocardiography results that indicate a sternal approach would be preferred include significant aortic insufficiency, which complicates cardioplegia delivery, severe mitral annulus calcification, left ventricular dysfunction, and pulmonary hypertension. CT results are important in assessing patients for aortoiliac atherosclerosis, femoral artery diameter, and pectus excavatum. The existence of any of these indicates a patient more appropriate for the sternal approach than the robotic approach.

Algorithm for determining patient eligibility for the robotic approach to mitral valve repair.1
ALGORITHM IMPACT
What was the effect of this algorithm? In the 500 cases after its implementation, the stroke rate decreased by more than half—from 10 incidents before to 4 incidents after—and mitral replacements dropped from 4 to 0. The rate of conversion from robotic repair to conventional sternotomy in this patient series also improved, although this likely reflects surgical experience more than the algorithm. The conversion rate initially increased as surgeons gained experience with the robotic techniques. It rose to 4% during the first 300 to 400 cases, then dropped to 2% at the 500-case mark. It leveled off for the next 300 cases before dropping to 0 toward the end of the series.
Other metrics improved as well, which were attributed to a combination of surgical experience with robotic assistance and use of the patient-selection algorithm. The stroke risk declined to 0.8%, ischemic and cardiopulmonary bypass times declined, and the transfusion rate declined. No mitral replacements were done in the last 500 cases, and the conversion to conventional sternotomy rate declined to 1%.
In conclusion, this Cleveland Clinic study showed that a combination of a focused preoperative assessment using the patient-selection algorithm and increased surgical experience with robotic techniques enhanced clinical outcomes and improved procedural efficiency associated with robotically assisted mitral valve surgery.
- Copyright © 2017 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCE
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.