


Article Figures & Data
Figures
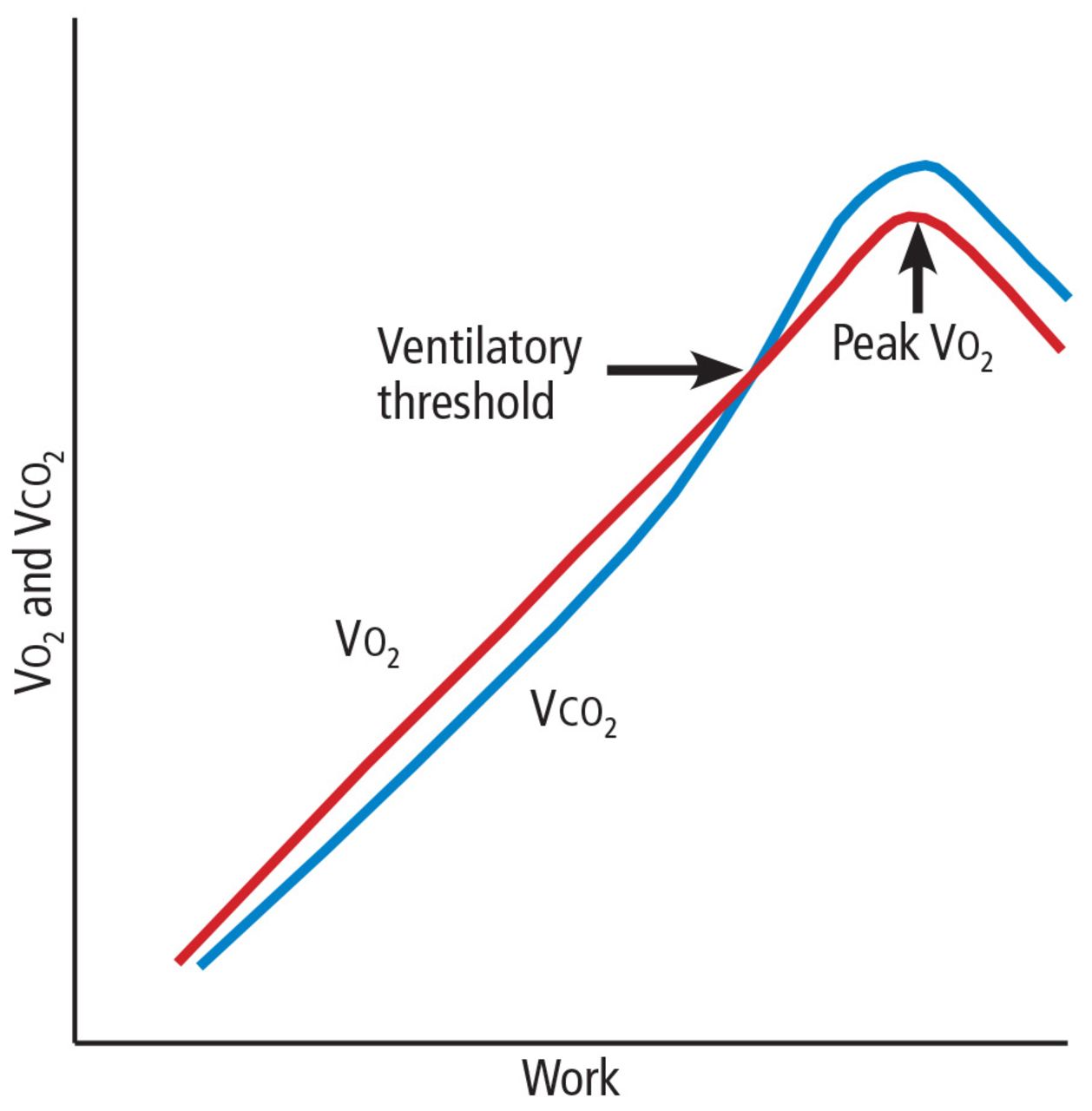
- FIGURE 1
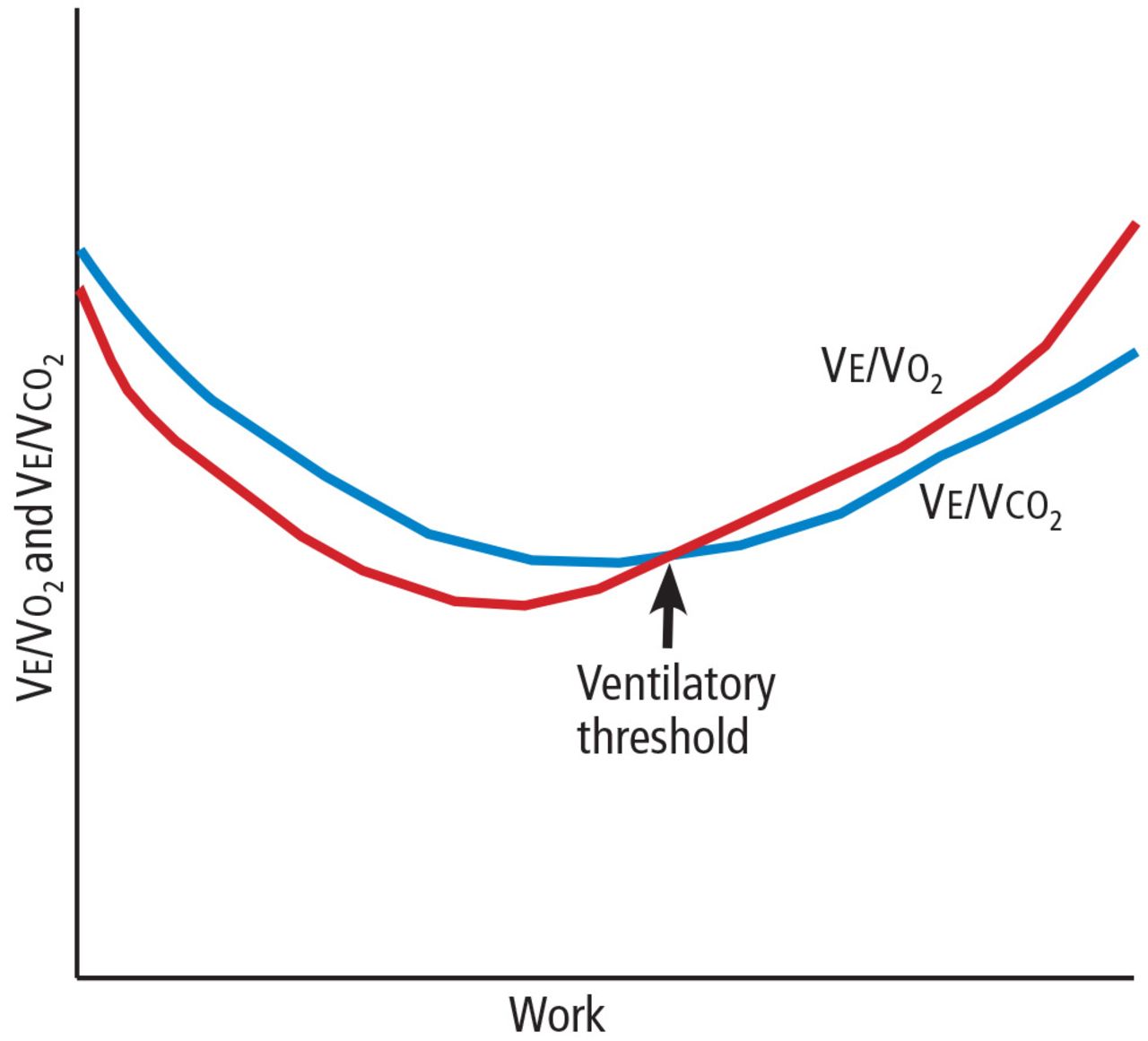
Diagram of response to work. Impairment from any cause will lower the peak Vo2 and ventilatory threshold.
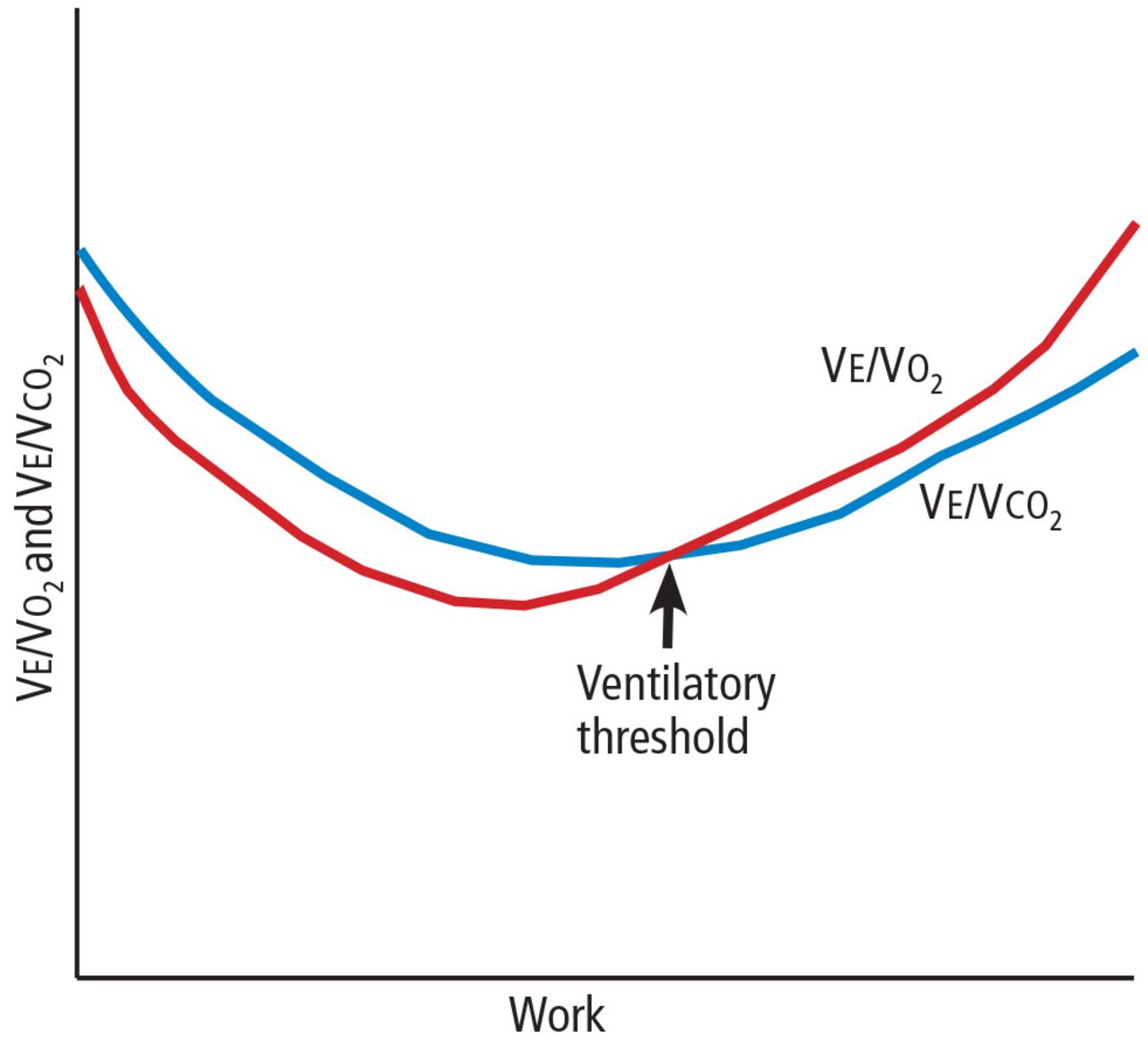
- FIGURE 2
One method of determining the ventilatory threshold is to determine the intersection of the Ve/Vo2 and Vco2 curves.
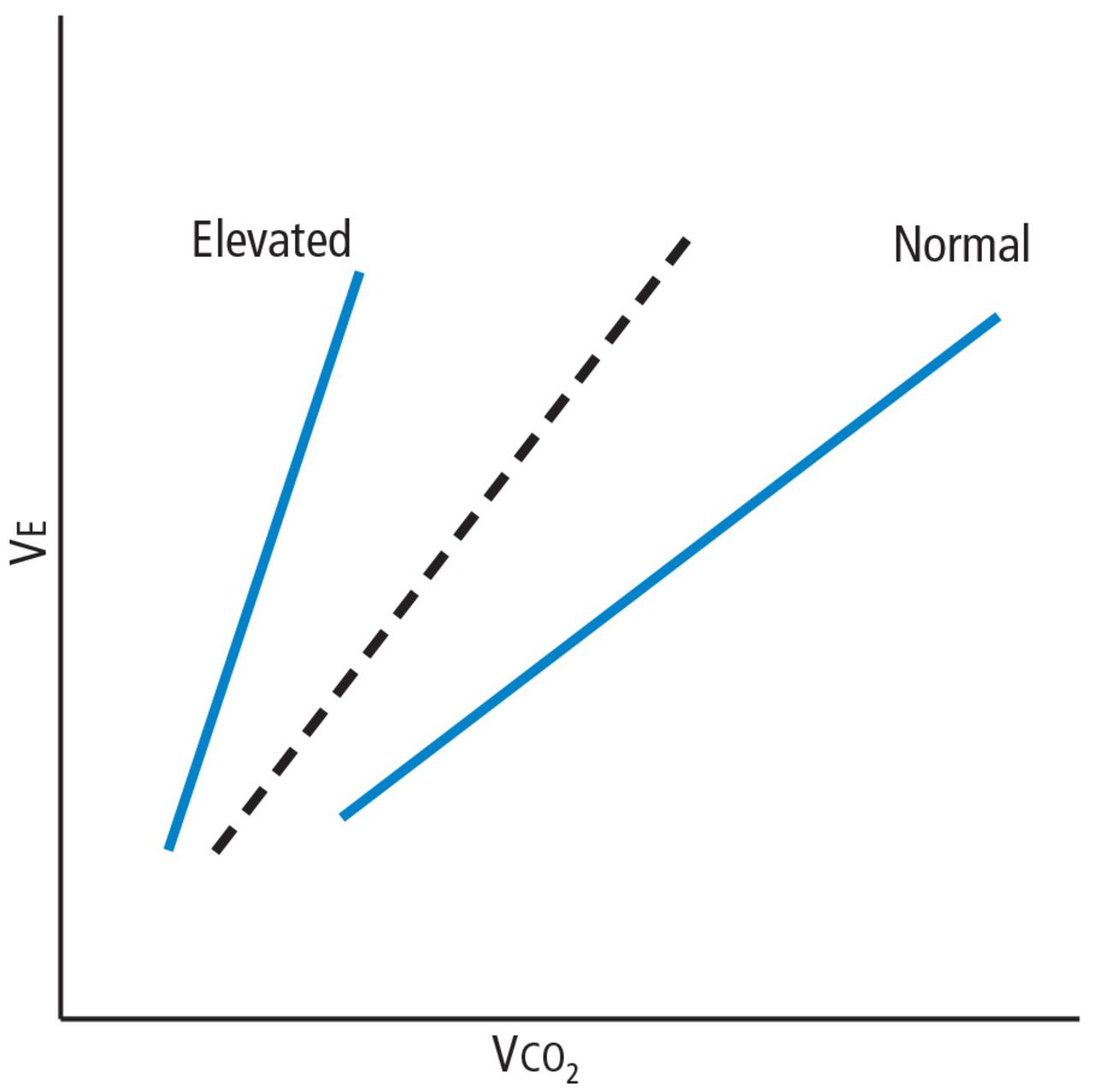
- FIGURE 3
The Ve/Vco2 slope is elevated in advanced heart failure and other hemodynamically significant cardiopulmonary conditions.


Tables
Peak Vo2
Highest oxygen uptake obtained (aerobic capacity)
Values vary widely with age, sex, activity level, weight, and disease (< 20 mL/kg/min in elderly; > 90 in elite athletes)
Nonspecific but starting point for interpretation and stratification
Peak Vo2 ≥ 85% of predicted is generally favorable; ≤ 14 mL/kg/min carries a poor prognosis in heart failure (≤ 10 if on beta-blockers)
Ventilatory threshold
Point at which anaerobic metabolism increases
Vo2 at ventilatory threshold typically is 40%–60% of peak Vo2
A low value is consistent with deconditioning or disease; a high value is consistent with athletic training
VE/Vco2 slope
Ventilatory volume/carbon dioxide output; reflects ventilatory efficiency
Normal 25–30
May be slightly elevated in isolation in otherwise healthy elderly patients
Elevated value reflects ventilatory inefficiency or ventilation-perfusion mismatch
Values ≥ 34 indicate clinically significant cardiopulmonary disease (heart failure, pulmonary hypertension, chronic obstructive pulmonary disease
Higher values = worse prognosis
Peak respiratory exchange ratio (VCO2/Vo2)
Reflects substrate metabolism
Normal < 0.8 at rest; progressively increases during exercise
Value > 1.1 signifies physiologically maximal response; lower value suggests submaximal effort
Peak heart rate
Varies with age, fitness level, use of beta-blockers Should increase linearly with ramped increase in work Peak rate ≥ 85% of predicted is generally favorable
Heart rate reserve
(Maximum heart rate – resting heart rate) divided by (predicted maximum heart rate – resting heart rate)
Reflects chronotropic competence
Normal ≥ 80% if not on beta-blocker; ≥ 62% if on beta-blocker; less than this = chronotropic incompetence
Heart rate recovery
Maximum heart rate minus rate at 1 minute recovery
Recovery ≥ 12 bpm is normal; < 12 is abnormal across all populations; < 6 is threshold in heart failure scoring systemVo2/work slope
Oxygen uptake per unit of work
Normal is 10 ± 1.5 mL/min/watt
Validated with cycle ergometry; not valid with treadmill exercise, as unable to calculate specific unit of work
A high slope reflects increased anaerobic demand or high oxygen cost, eg, in obesity or hyperthyroidism; low slope reflects increased anaerobic work, eg, in heart failure or coronary artery disease
O2-pulse
Oxygen delivered per heart beat; a surrogate for stroke volume
Curvilinear increase with exercise
Norms based on predicted peak Vo2 and peak heart rate; value ≥ 85% of predicted is favorable
Blunted response or decline suggests ventricular failure; response can be falsely high if heart rate is blunted
End-tidal Pco2
Reflects perfusion: better cardiac output = better CO2 diffusion
In heart failure, values > 33 mm Hg at rest and > 36 mm Hg at ventilatory threshold are favorable; low values = poor prognosis
Exercise oscillatory breathing
Abnormal breathing pattern often seen in heart failure; no universal definition
Sustained visible fluctuations in ventilations support a poorer prognosis
Oxygen uptake efficiency slope
Additional logarithmic model of ventilatory efficiency In heart failure, values < 1.4 carry a poor prognosis
Peak respiratory rate
Rarely exceeds 50/min
High value suggests pulmonary limitation or exceptional effort
Value < 30 suggests submaximal effort
Peak Ve/Mvv
Ventilatory reserve: peak exercise ventilations (VE) divided by predicted or measured maximum voluntaryventilations (Mvv)
Normal: 15%–20% reserve in most people
May be reduced or absent in elite athletes; reduced reserve suggests pulmonary limitation; excessive value suggests submaximal effortAdapted from information in references 4–7.
Nonspecific: suggest significant cardiopulmonary or metabolic impairment of any sort
Peak Vo2 < 80% of predicted
Ve/Vco2 slope > 34
Ventilatory (anaerobic) threshold < 40% of peak Vo2Deconditioning
Low-normal peak Vo2
Low ventilatory (anaerobic) threshold
Absence of any other abnormal responsesObesity
Increased Vo2/work slope
Indexed peak Vo2 (mL/kg/min) less than predicted
Absolute Vo2 (L/min) normal or greater than predicted
Oxygen indexed to lean body mass normal or greater than predictedCardiac limitations
Oxygen pulse (O2 -pulse) < 80% predicted or flattened or falling curve Chronotropic incompetence
Heart rate recovery ≤ 12 beats per minute after 1 minute of recovery Standard electrocardiographic criteria for ischemiaPulmonary limitations
Peak exercise respiratory rate > 50 per minute
Ventilatory reserve (peak Ve /Mvv) < 15%
Oxygen desaturation by pulse oximetry
Abnormal results on pretest screening spirometry
Abnormal exercise flow-volume loopsMuscular disease
Submaximal cardiac and respiratory responses
Ventilatory (anaerobic) threshold < 40% of peak Vo2
Elevated lactate at any given level of submaximal workVariable Value Points Ventilation/carbon dioxide (Ve/Vco2) slope ≥ 34 7 Heart rate recoverya ≤ 6 bpm 5b Oxygen uptake efficiency slope ≤ 1.4 2 Peak Vo2 ≤ 14 mL/kg/min 2 Score > 15 points: annual mortality rate 12.2%; relative risk > 9 for transplant, left ventricular assist device, or cardiac death.
Score < 5 points: annual mortality rate 1.2%.
↵a Maximum heart rate minus heart rate at 1 minute in recovery.
↵b 2 points if on a beta-blocker.
Information from reference 24.
History and clinical context
Relevant medical history, specifics of exercise intolerance, prior exercise test results, relevant studies (eg, echocardiography, pulmonary function tests, complete blood cell count), relevant medications (eg, beta-blockers)Resting data
Weight, body mass index, percent body fat, heart rate, blood pressure, pulse oximetry, screening spirometry, hemoglobin, electrocardiogramExercise protocol
Treadmill, cycle, or arm geometry; rate of ramp increase; peak workloadReason for test termination
Fatigue, symptoms, abnormal electrocardiographic findingsSubjective responses
Peak rating of perceived exertion
Specific symptoms and comparison to index symptomsValidity of test
Peak respiratory exchange ratio ≥ 1.1, rating of perceived exertion≥17Oxygen responses
Peak Vo2 relative to norms, Vo2 per ideal weight, Vo2 at ventilatory thresholdSpecific cardiac responses
Reflected in exercise and recovery heart rate, blood pressure, O2-pulse, electrocardiogramSpecific pulmonary responses
Peak respiratory rate, ventilations; ventilatory reserve , (Ve/Mvv) pulse oximetry, blood gasesMarkers of central cardiopulmonary inefficiency Ve/Vco2 slope, end-tidal Pco2 responses, exercise oscillatory breathing, oxygen uptake efficiency slope Summary statement
The bottom line for referring provider; normal vs abnormal; if abnormal, suggest differential diagnoses; CPET score for heart failure (see Table 3)Recommendations
To guide referring provider
Reassurance if normal
Formal exercise program for fitness or weight loss
Suggest adjunctive tests if abnormal (eg, formal spirometry, right heart catheterization, chest computed tomography, natriuretic peptide measurement)
Beta-blocker modification or pacemaker if chronotropically incompetent




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.