


A 96-year-old woman with hypertension, diabetes, and dementia was found unresponsive in her nursing home and was transferred to the hospital.
At presentation to the hospital, her blood pressure was 76/43 mm Hg, heart rate 42 beats per minute, rectal temperature 31.6°C (88.8°F), and blood glucose 36 mg/dL.
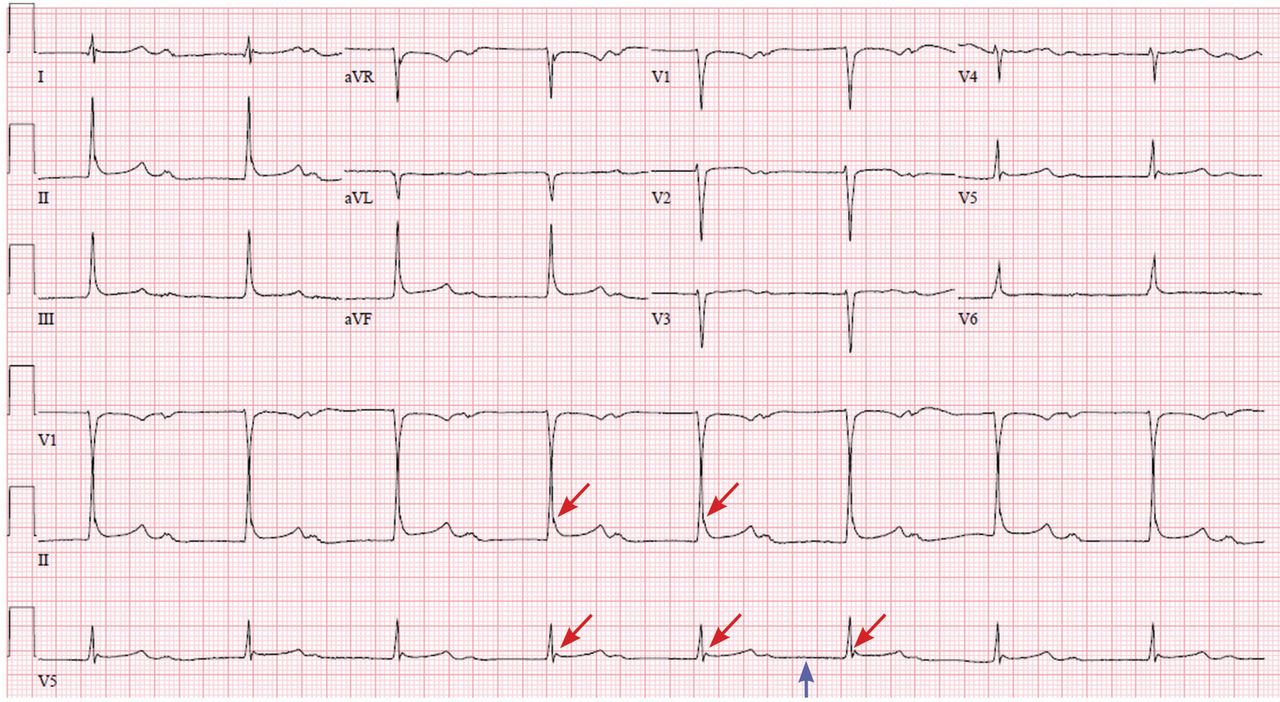
The initial electrocardiogram (ECG) (Figure 1) showed sinus bradycardia with first-degree atrioventricular block and a PR interval of 704 ms. The QRS interval was mildly increased, and the corrected QT interval was mildly prolonged at 476 ms. There was also evidence of probable small Osborn waves in leads II and V5, and leads aVF and aVL seemed reversed, as was confirmed in successive ECGs.
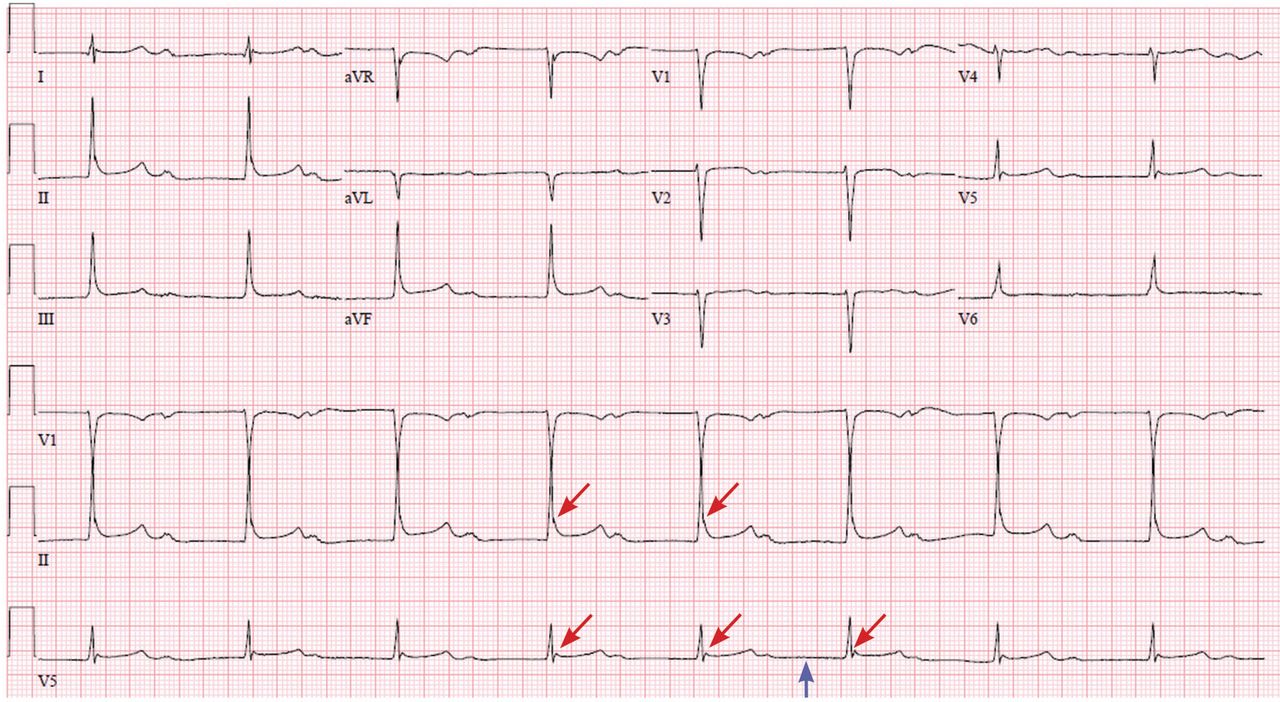
The initial electrocardiogram showed sinus bradycardia with first-degree atrioventricular block, a PR interval of 704 ms (blue arrow), a mildly increased QRS interval, a mildly prolonged corrected QT interval, and evidence of Osborn waves in leads II and V5 (red arrows). Leads aVF and aVL seemed reversed.
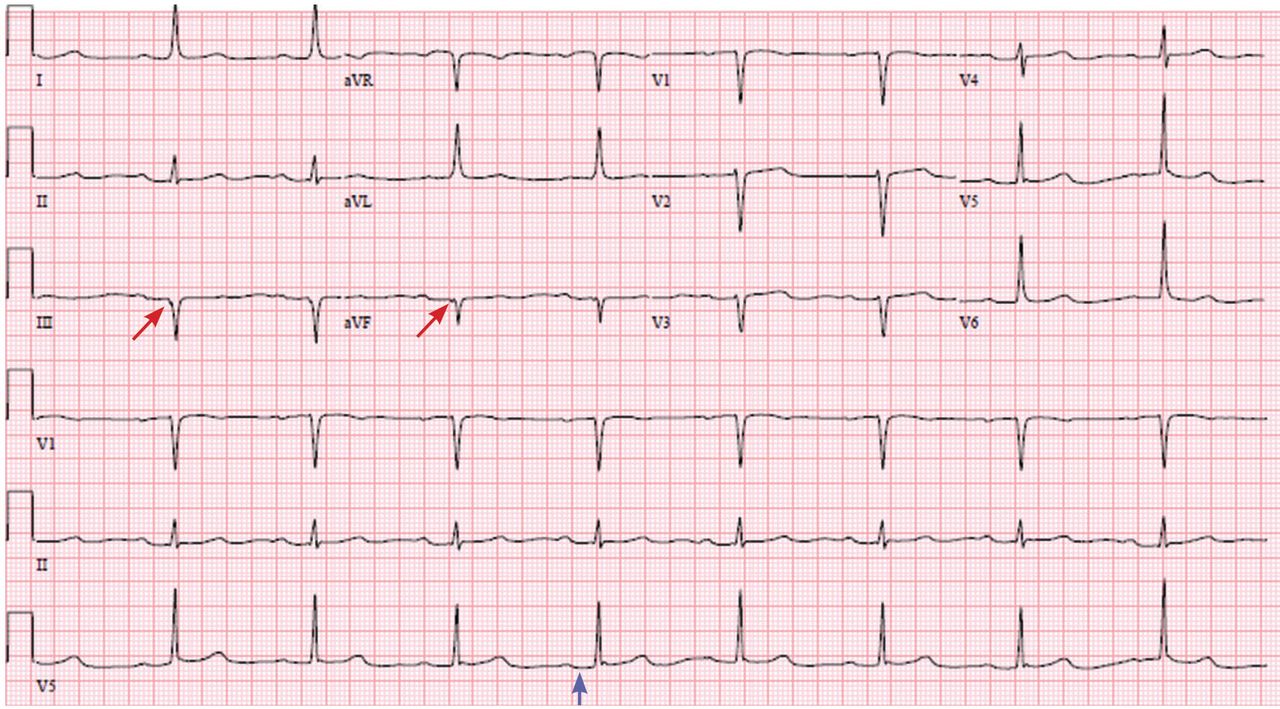
The patient was resuscitated with intravenous fluids and glucose and was rewarmed. Repeat ECG 3 hours later (Figure 2) revealed sinus bradycardia with first-degree atrioventricular block and a PR interval of 216 ms with a rate of 52. This time the leads were confirmed in correct position, with aVF showing negative QRS deflection. Q waves were also noted in leads III and aVF, as in previous ECGs, and suggested an old inferior wall infarction. This was not seen on the first ECG because of probable lead reversal, and the suspected Osborn waves were also less prominent in V5 and absent in lead II. The corrected QT interval was now 465 ms, and her body temperature at this time was 32.8°C (91.0°F).

After 3 hours of resuscitation and rewarming, the electrocardiogram showed a near-normal PR interval of 216 ms (blue arrow). Q waves noted in leads III and aVF (red arrows) suggested an old inferior wall infarction.
Causes of secondary hypothermia were sought. Blood and urine cultures were negative. Computed tomography of the head showed no acute intracranial abnormalities. Tests for adrenal insufficiency and hypothyroidism were negative.
HYPOTHERMIA AND THE ECG
Hypothermia can produce a number of changes on the ECG. At the start of hypothermia, a stress reaction is induced, resulting in sinus tachycardia. But when the temperature goes below 32°C, sinus bradycardia ensues,1 resulting in various degrees of heart block.2 In our patient, a severely prolonged PR interval resulted in first-degree heart block.
Other findings on ECG associated with hypothermia include atrial fibrillation, widening of the P and T waves, prolonging of the QT interval, and widening of the QRS interval. Progressive widening of the QRS interval can predispose to ventricular fibrillation.1,3
An Osborn or J wave is a wave found between the end of the QRS and the beginning of the ST segment and is usually seen on the inferior and lateral precordial leads. It is found in as many as 80% of patients when the body temperature is below 30°C.1,3,4
Although Osborn waves are a common finding in hypothermia, they are also seen in electrolyte imbalances such as hypercalcemia and in central nervous system diseases.5,6 Hypothermia-associated changes on ECG are usually readily reversible with rewarming.1
TAKE-HOME MESSAGES
The ECG should always be interpreted in the proper clinical context and, whenever possible, compared with a previous ECG. It is prudent to always consider potentially reversible triggers of hypothermia other than environmental exposure such as hypothyroidism, infection, adrenal insufficiency, ketoacidosis, medication side effects, and alcohol use.
Hypothermia, especially in elderly patients with multiple comorbidities, can lead to bradycardia and varying degrees of heart block.
- Copyright © 2018 The Cleveland Clinic Foundation. All Rights Reserved.



{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.