


A 23-year-old woman presented with hematuria. Her blood pressure was normal, and she had no rash, joint pain, or other symptoms. Urinalysis was positive for proteinuria and hematuria, and urinary sediment analysis showed dysmorphic red blood cells (RBCs) and red cell casts, leading to a diagnosis of glomerulonephritis. She had proteinuria of 1.2 g/24 hours. Laboratory tests for systemic diseases were negative. Renal biopsy study revealed stage III immunoglobulin A (IgA) nephropathy.
See related editorial, page 22
GLOMERULAR HEMATURIA
Glomerular hematuria may represent an immune-mediated injury to the glomerular capillary wall, but it can also be present in noninflammatory glomerulopathies.1
The type of dysmorphic RBCs (crenated or misshapen cells, acanthocytes) may be of diagnostic importance. In particular, dysmorphic red cells alone may be predictive of only renal bleeding, while acanthocytes (ring-shaped RBCs with vesicle-shaped protrusions best seen on phase-contrast microscopy) appear to be most predictive of glomerular disease.2 For example, in 1 study,3 the presence of acanthocytes comprising at least 5% of excreted RBCs had a sensitivity of 52% for glomerular disease and a specificity of 98%.3
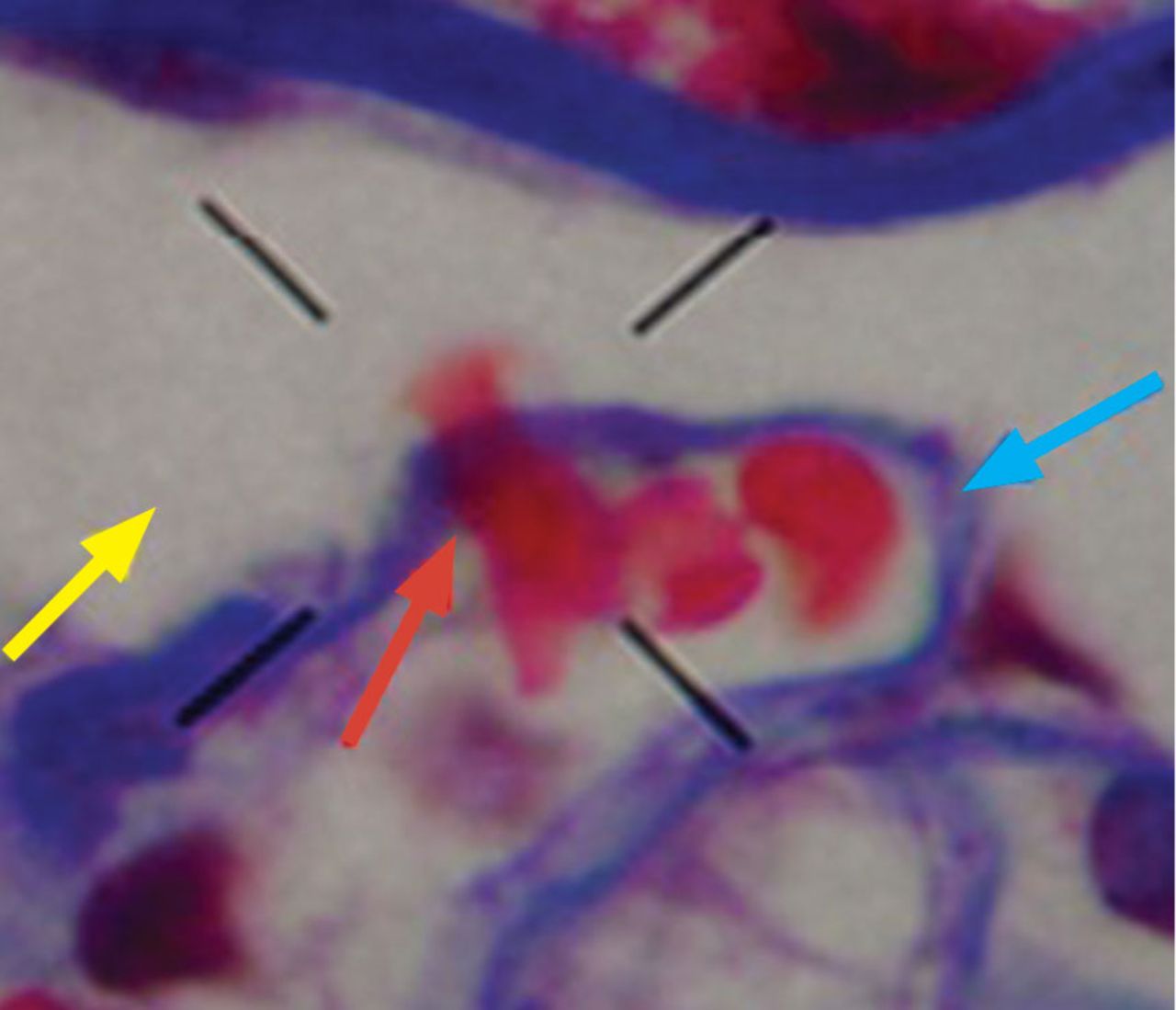
How erythrocytes become dysmorphic is not entirely known.4 In vitro, changes in osmolality or pH do not produce dysmorphism, but it can occur along the different tubular segments.5,6 In addition, RBCs can lose their shape when crossing the glomerular basement membrane (Figure 1) and during passage along the tubular system.4
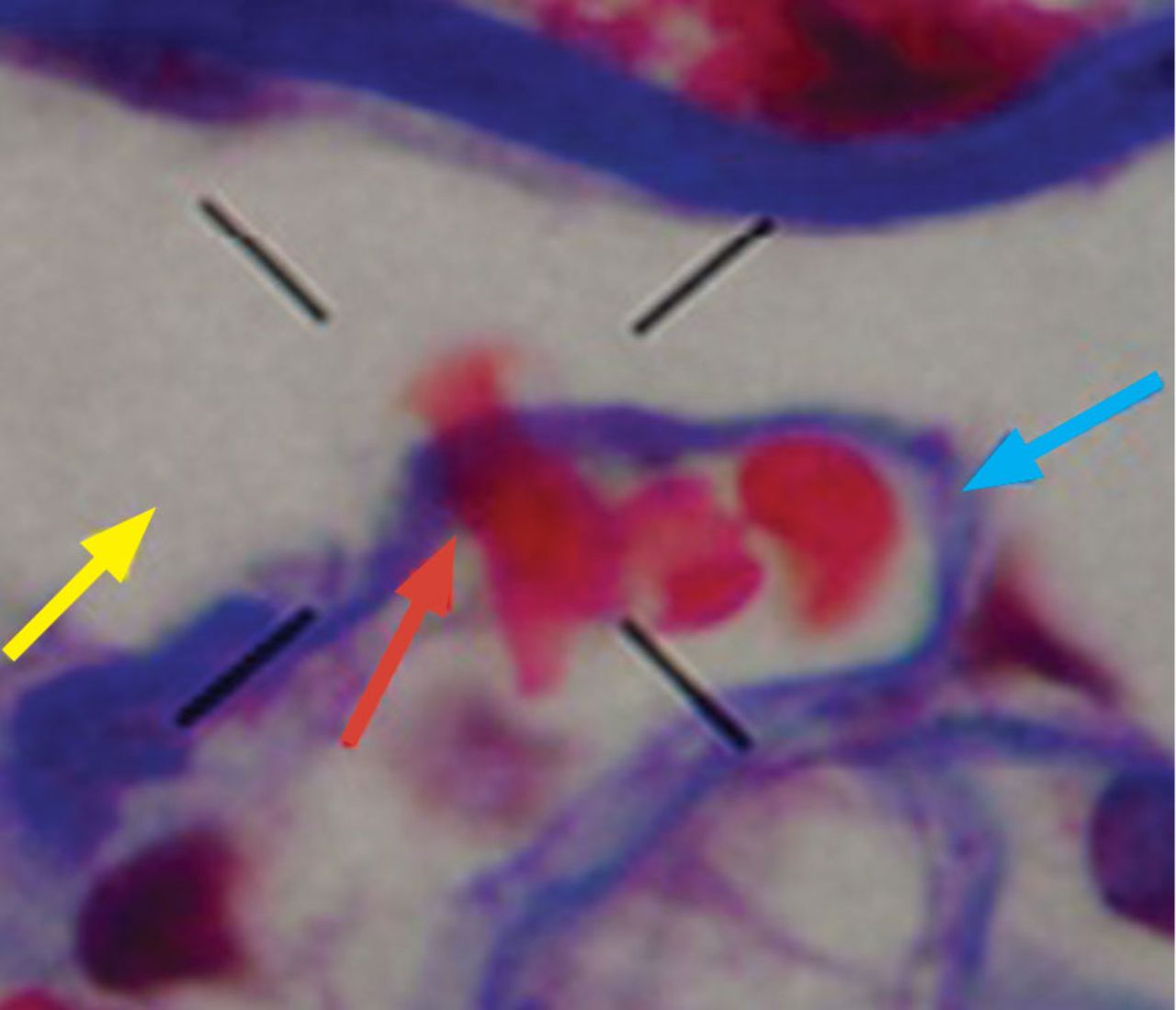
A red blood cell (red arrow) is seen crossing the basement membrane (blue arrow) and losing its shape, one of the mechanisms proposed for acanthocyte formation; the yellow arrow points to the urinary space (Masson trichrome stain, × 1,000.
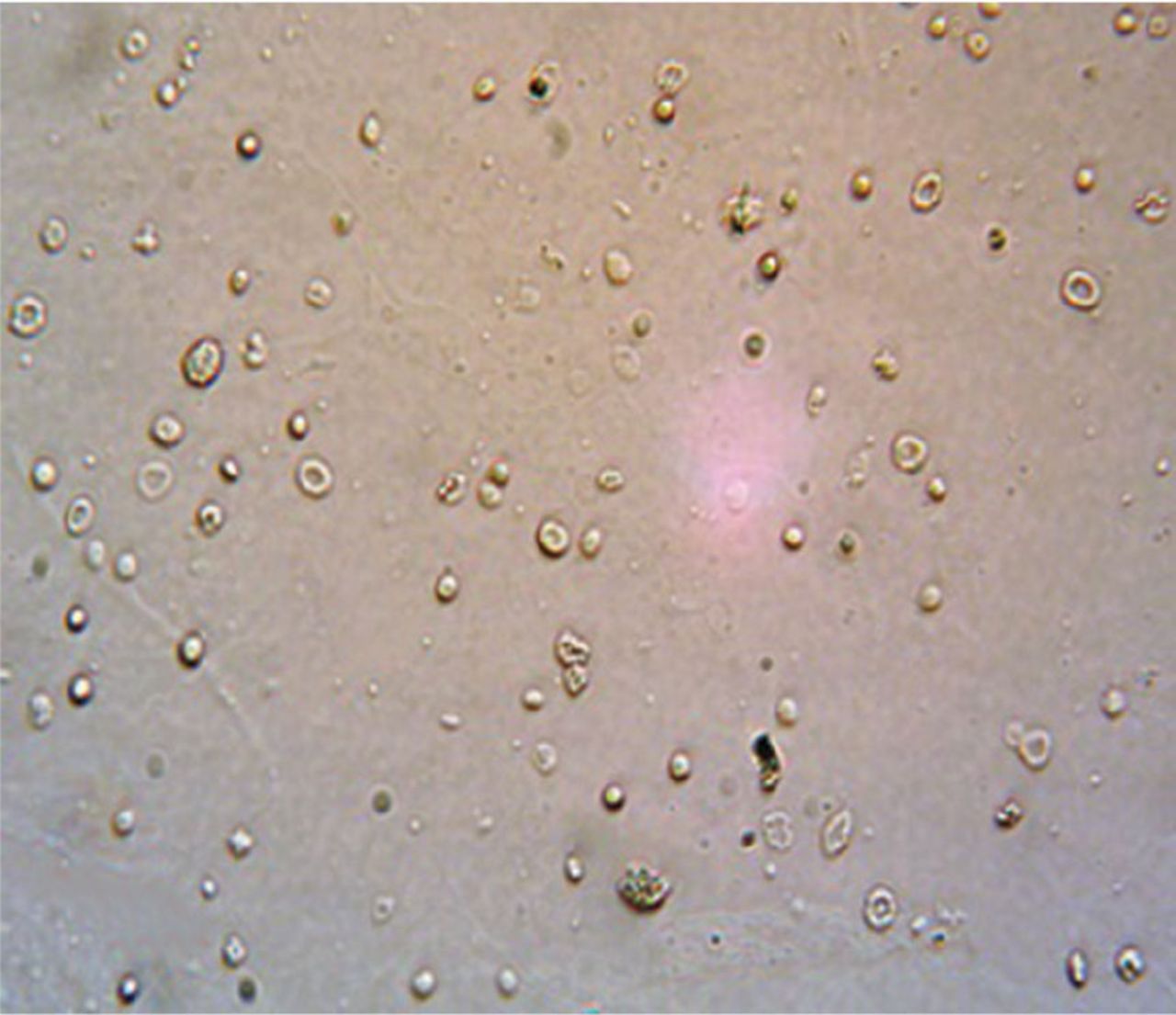
Dysmorphic urinary RBCs have been regarded as an indicator of glomerular pathology,7 and dysmorphic RBCs in urinary sediment (Figure 2) are also considered to represent renal pathology. On electron microscopy, the glomerular basement membrane is usually 300 to 400 nm wide, whereas the diameter of the red blood cell is 7 μm. The change in RBC shape is manifested as blebs, budding, and segmental loss of membrane, resulting in marked variability in shape and in a reduction in mean cell size. These changes may be due to mechanical trauma as the cells pass through rents in the glomerular basement membrane and to osmotic trauma as cells flow through the nephron.8
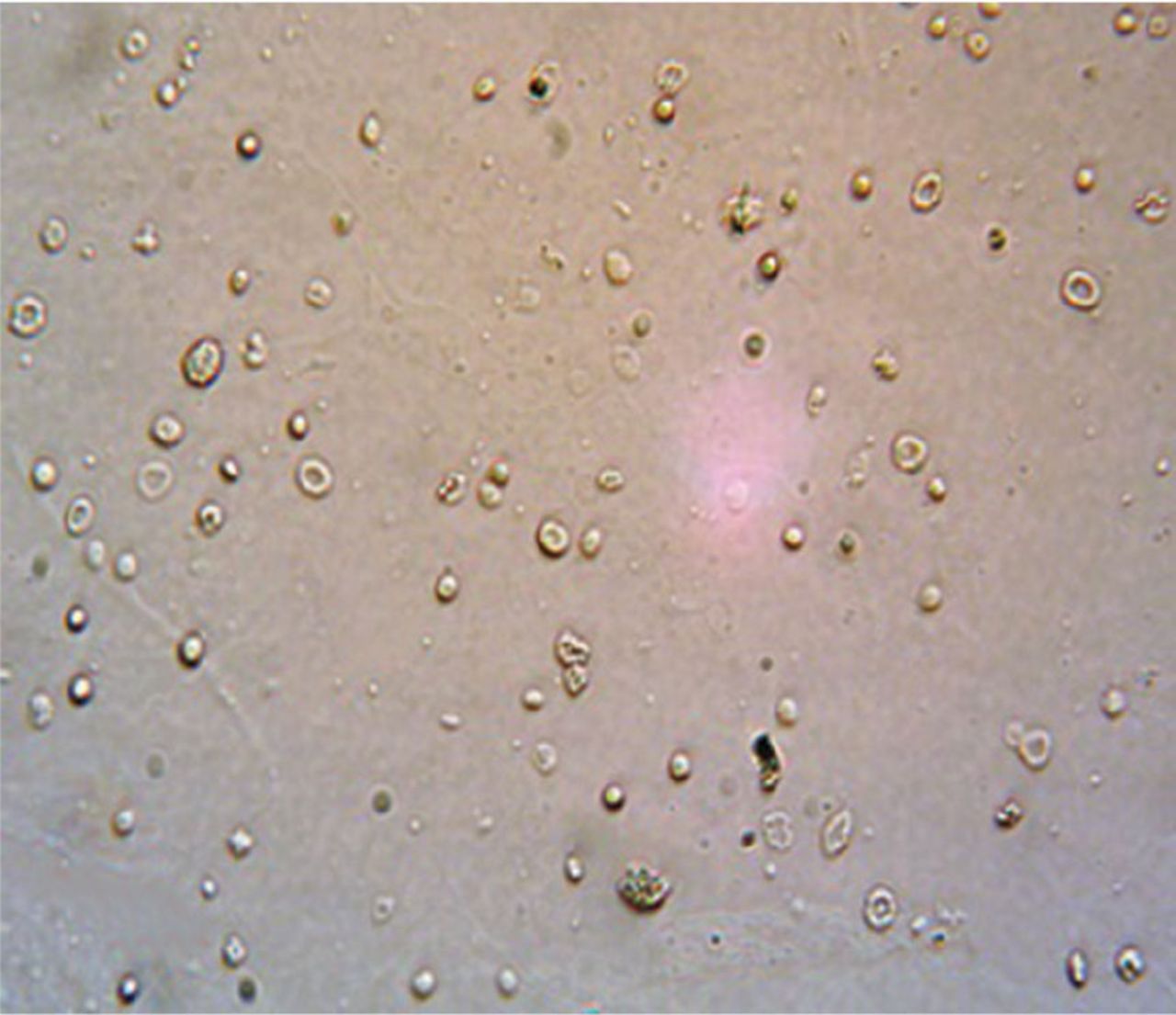
Examination of urinary sediment shows typical dysmorphic hematuria with acanthocytes (× 400).
- Copyright © 2018 The Cleveland Clinic Foundation. All Rights Reserved.



{kind=link}
{kind=link}