


Article Figures & Data
Figures
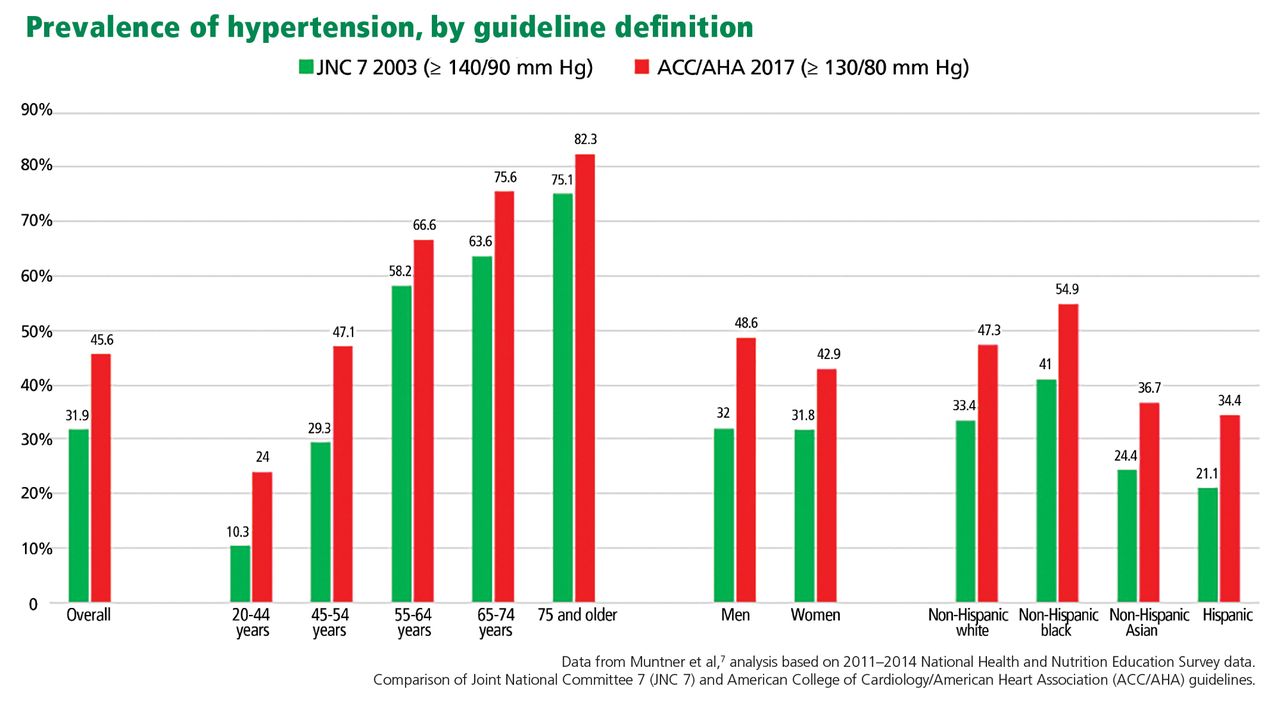
- Figure 1
With the 2017 guideline definition, the prevalence of hypertension is higher.

Tables
Systolic BP (mm Hg) Diastolic BP (mm Hg) JNC 7 (2003) ACC/AHA (2017) < 120 and < 80 Normal Normal 120–129 and < 80 Prehypertension Elevated BP 130–139 or 80–89 Prehypertension Stage 1 hypertension 140–159 or 90–99 Stage 1 hypertension Stage 2 hypertension ≥ 160 or ≥ 100 Stage 2 hypertension Stage 2 hypertension ACC = American College of Cardiology; AHA = American Heart Association; BP = blood pressure; JNC = Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure
Guideline Blood pressure goals (mm Hg) Initial drug therapy JNC 7 (2003)3 General population < 140/90 Thiazide Chronic kidney disease < 130/80 ACE inhibitor or ARB Diabetes mellitus < 130/80 Thiazide, CCB, beta-blocker, ACE inhibitor, or ARB
With proteinuria: ACE inhibitor or ARBNICE (2011)25 General population < 140/90 Black or age > 55: CCB, thiazide
Nonblack or age ≤ 55: ACE inhibitor or ARB
With proteinuria: ACE inhibitor or ARBElderly (age ≥ 80) < 150/90 Chronic kidney disease < 140/90 Diabetes mellitus < 140/90a Black: ACE inhibitor or ARB + CCB or thiazide
Nonblack: ACE inhibitor or ARB
With proteinuria: ACE inhibitor or ARBKDIGO (2012)29 Chronic kidney disease with albuminuria
< 30 mg/24 hoursb≤ 140/90 ≥ 30 mg/24 hoursb ≤ 130/80 ACE inhibitor or ARB ESH/ESC (2013)24 General population < 140/90 Thiazide, CCB, beta-blocker, ACE inhibitor or ARB Elderly (age ≥ 80) < 150/90 Chronic kidney disease < 140/90 Thiazide, CCB, beta-blocker, ACE inhibitor, or ARB
With proteinuria: ACE inhibitor or ARBDiabetes mellitus < 140/85 ASH/ISH (2014)28 General population < 140/90 Black: CCB or thiazide
Nonblack, age < 60: ACE inhibitor or ARB
Nonblack, age ≥ 60: CCB or thiazideElderly (age ≥ 80) < 150/90 Chronic kidney disease < 140/90 ACE inhibitor or ARB Diabetes mellitus < 140/90 ACE inhibitor or ARB
Black: acceptable to start with CCB or thiazideJNC 8 (2014)5 General population < 140/90 Black, including those with diabetes: thiazide, CCB
Nonblack, including those with diabetes: thiazide, CCB, ACE inhibitor, or ARBOlder patients (age ≥ 60) < 150/90 Diabetes mellitus < 140/90 Chronic kidney disease < 140/90 ACE inhibitor or ARB Hypertension Canada (2018)12 General population < 140/90 Thiazide, CCB, beta-blocker (in age < 60), ACE inhibitor (in nonblack), or ARB Chronic kidney disease < 140/90 With proteinuria: ACE inhibitor or ARB Diabetes mellitus < 130/80 Thiazide, CCB, ACE inhibitor, or ARB
With proteinuria or renal disease: ACE inhibitor or ARBACC/AHA (2017)1 General population < 130/80 Thiazide, CCB, ACE inhibitor, or
ARB Black including diabetes, but no heart failure or chronic kidney disease: CCB, thiazideOlder patients (age ≥ 65) < 130/80c Chronic kidney disease < 130/80 Thiazide, CCB, ACE inhibitor, or ARB
With proteinuria: ACE inhibitor or ARBDiabetes mellitus < 130/80 ACP/AAFP (2017)27 Older patients (age ≥ 60) < 150/90 ADA (2017)30 Diabetes mellitus < 140/90 Thiazide, CCB, ACE inhibitor, or ARB
With proteinuria: ACE inhibitor or ARB↵a < 130/80 if chronic kidney disease and diabetes mellitus;
↵b Or equivalent;
↵c Unless alternative goal determined by physician.
AAFP = American Academy of Family Physicians; ACC = American College of Cardiology; ACE = angiotensin-converting enzyme; ACP = American College of Physicians; ADA = American Diabetes Association; AHA = American Heart Association; ARB = angiotensin II receptor blocker; ASH = American Society of Hypertension; CCB = calcium channel blocker; ESC = European Society of Cardiology; ESH = European Society of Hypertension; ISH = International Society of Hypertension; JNC = Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; KDIGO = Kidney Disease: Improving Global Outcomes; NICE = National Institute for Health and Care Excellence




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.