


Article Figures & Data
Figures
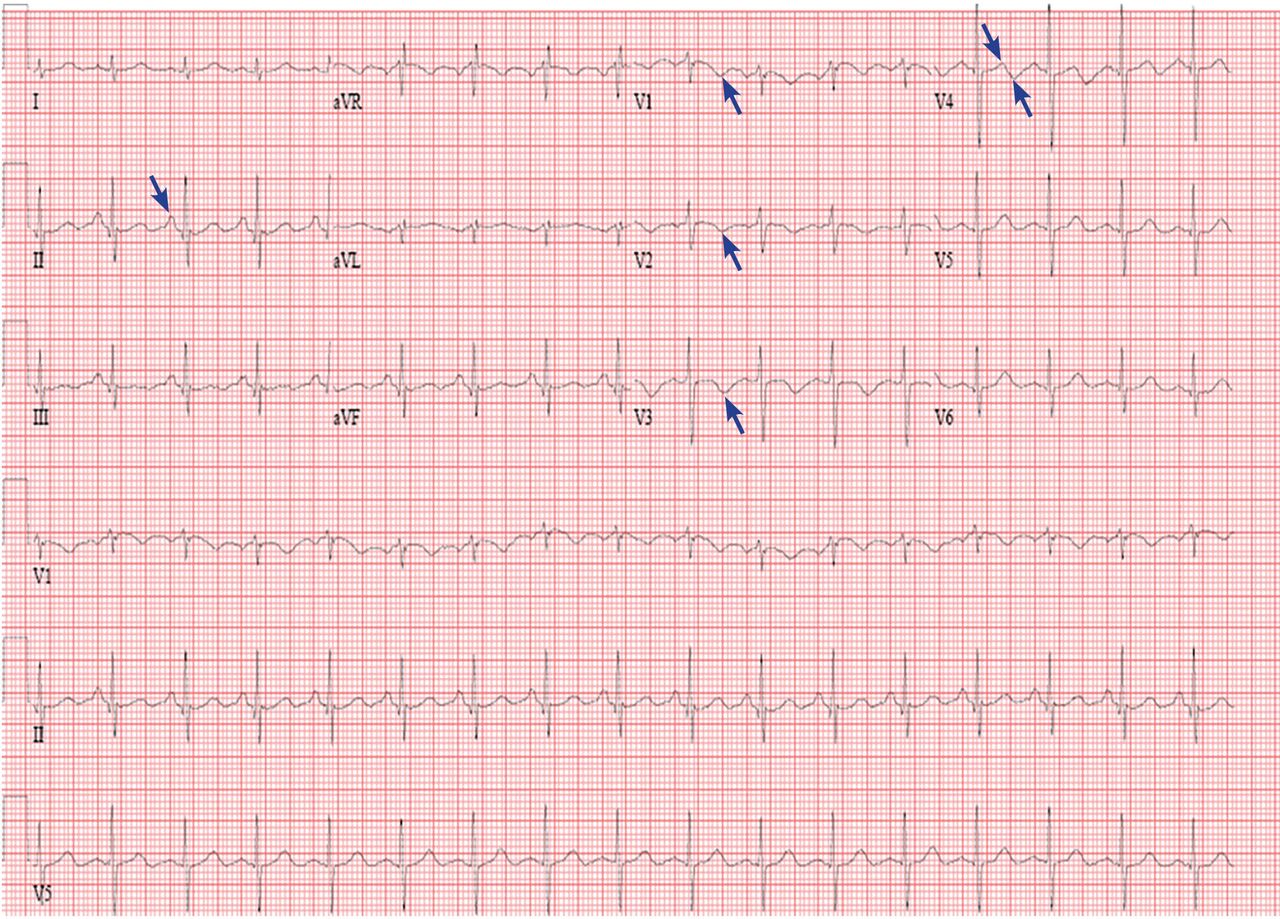
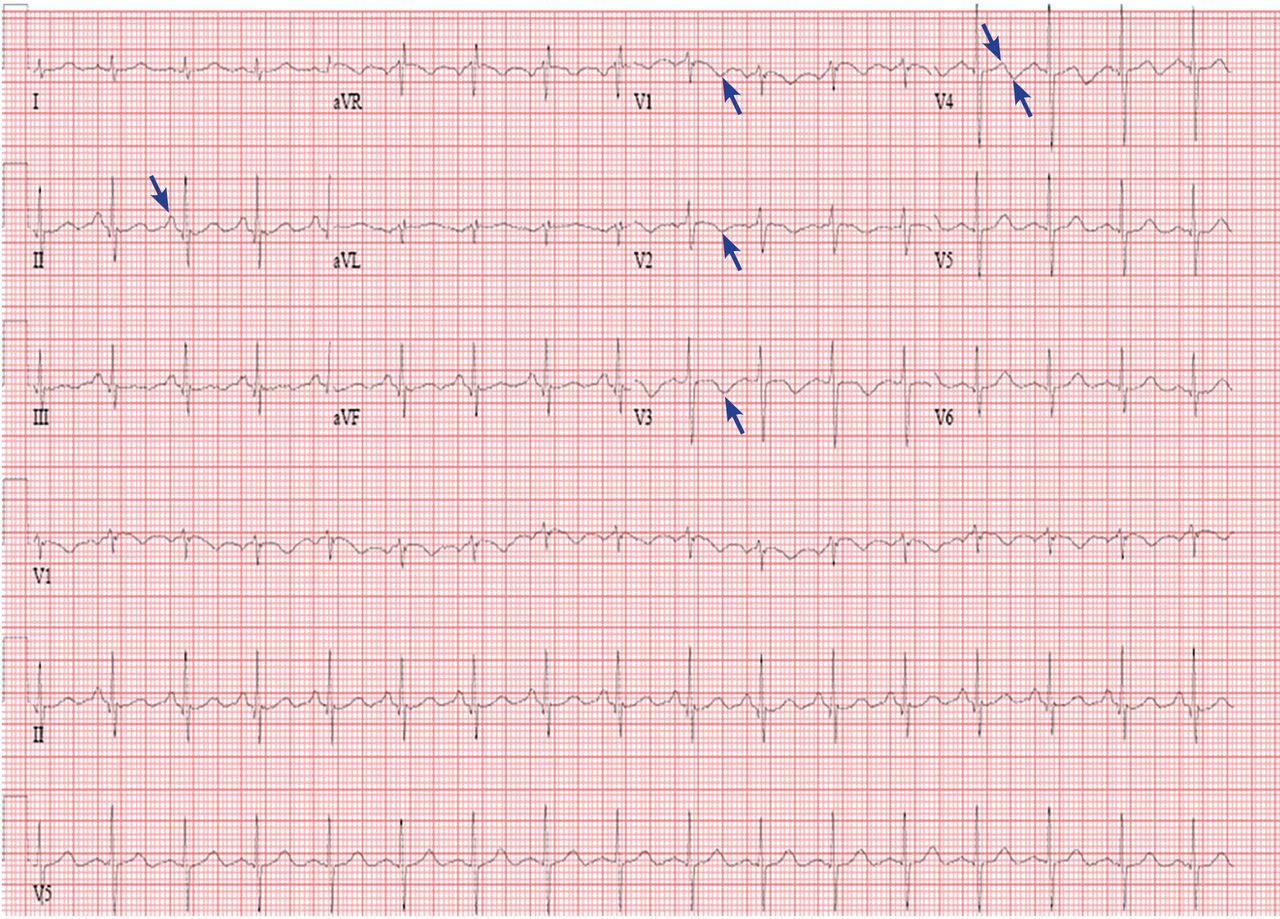
- Figure 1
The patient’s electrocardiogram on presentation. Arrows point to notable features (see text).
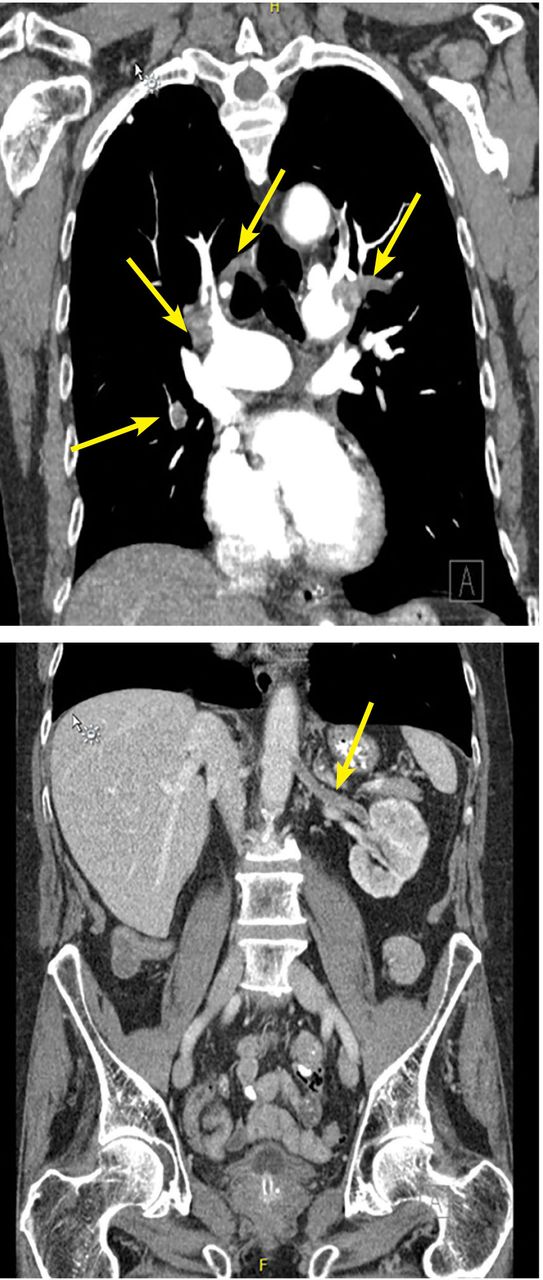
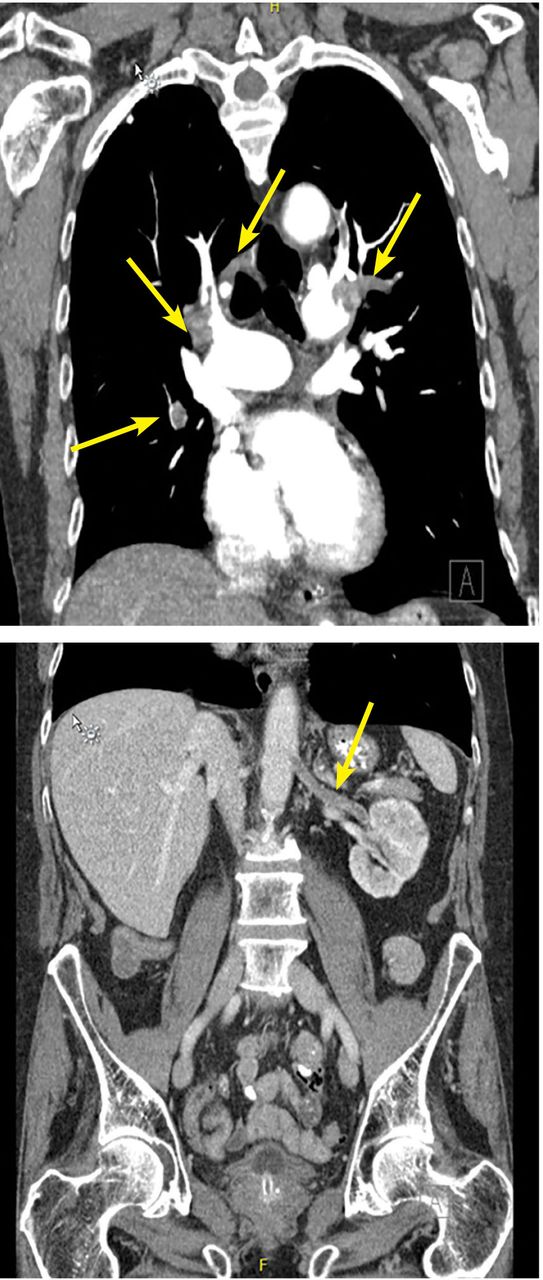
- Figure 2
Computed tomography (CT) with a chest pulmonary embolism protocol (top) showed filling defects (arrows). CT of the abdomen and pelvis showed renal artery thrombosis (arrow).
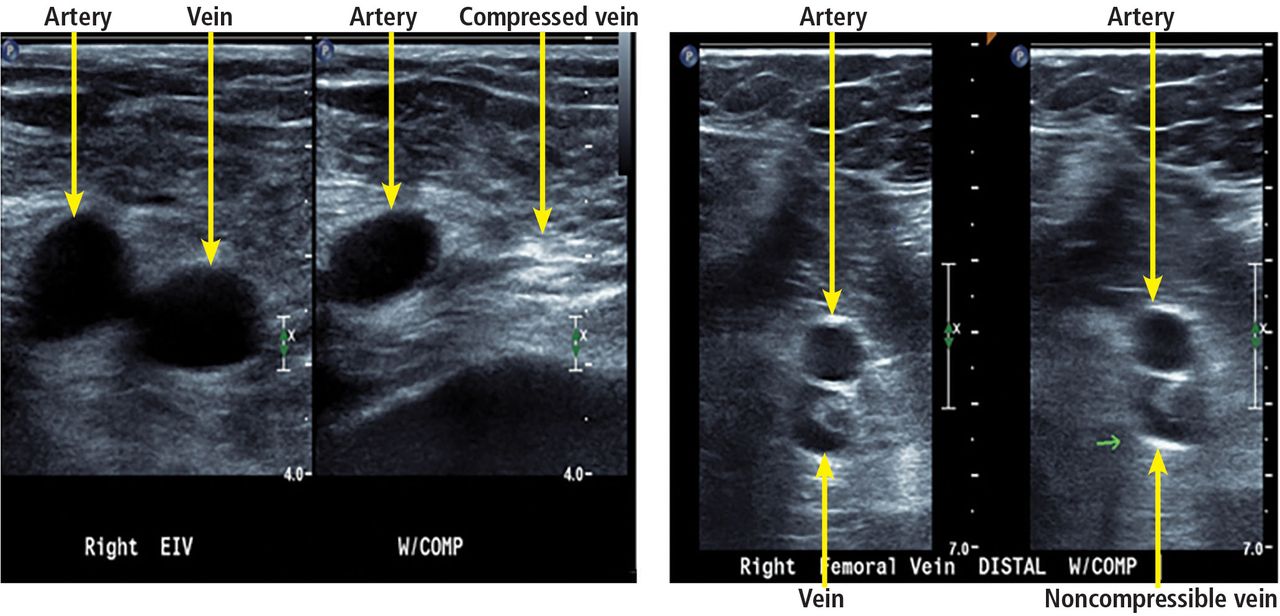
- Figure 3
Example of lower-extremity duplex ultrasonography. Arteries and veins are labeled. Veins with-out deep vein thrombosis are compressible, as seen on the left. A vein is shown that is not compressible, suggesting deep vein thrombosis.
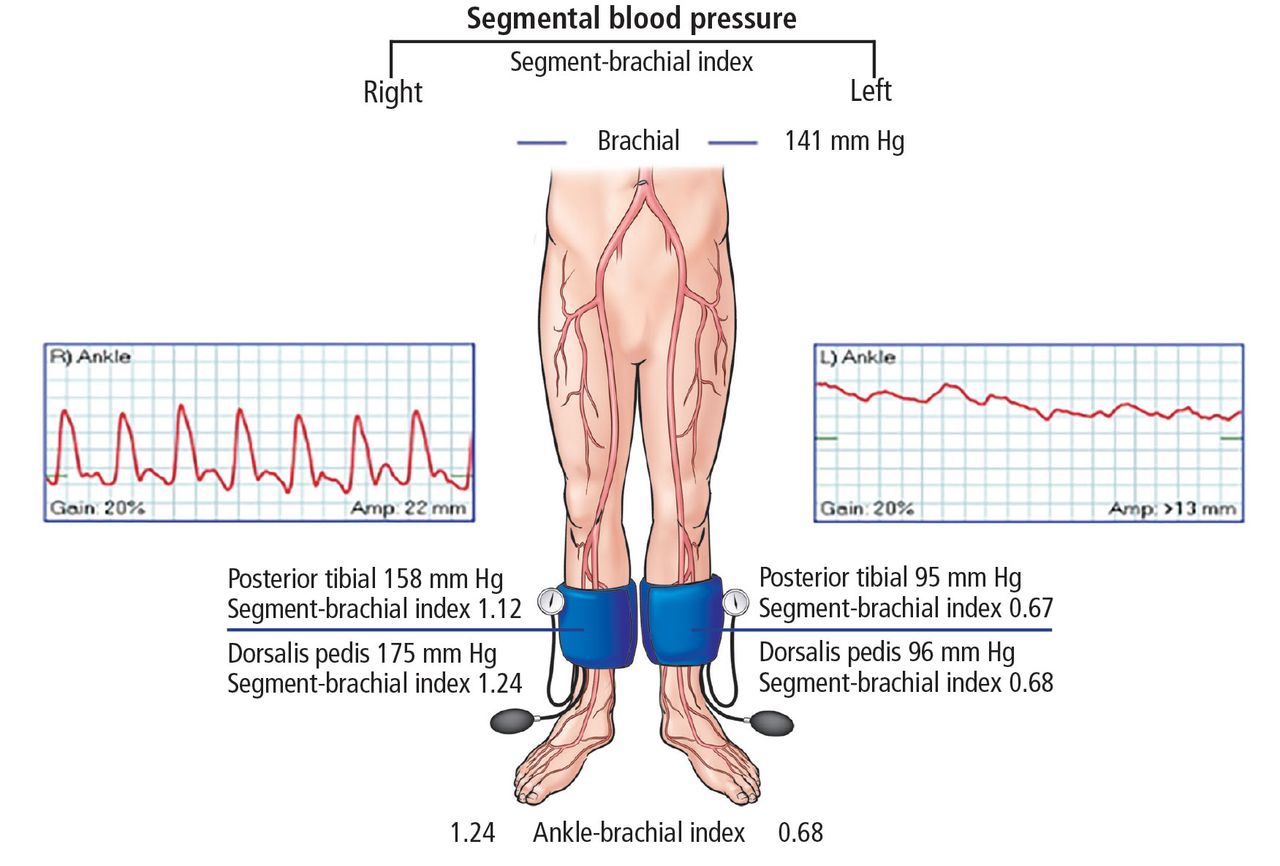
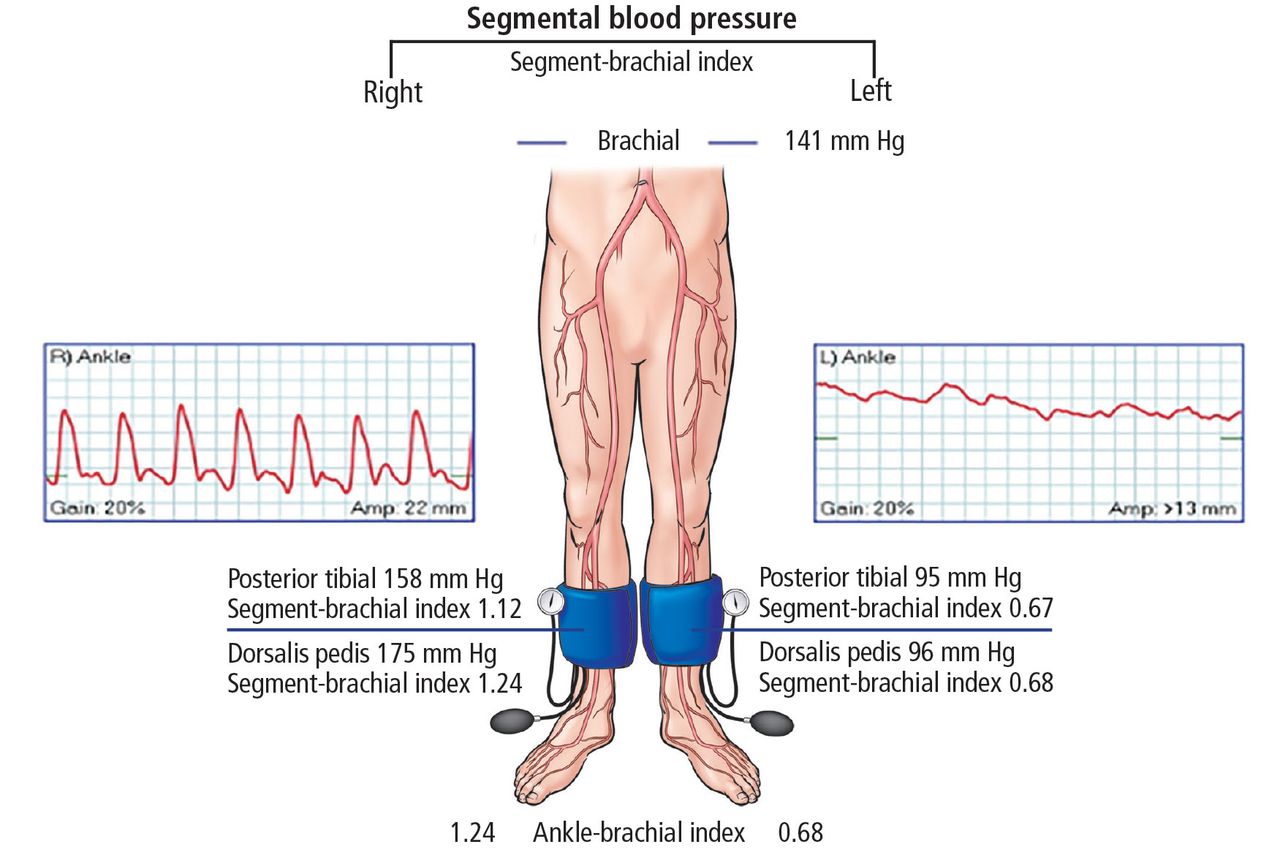
- Figure 4
The patient’s ankle-brachial index and pulse-volume recordings. Right side 1.24, left side 0.68. This suggests moderate disease on the left and normal vessels on the right.
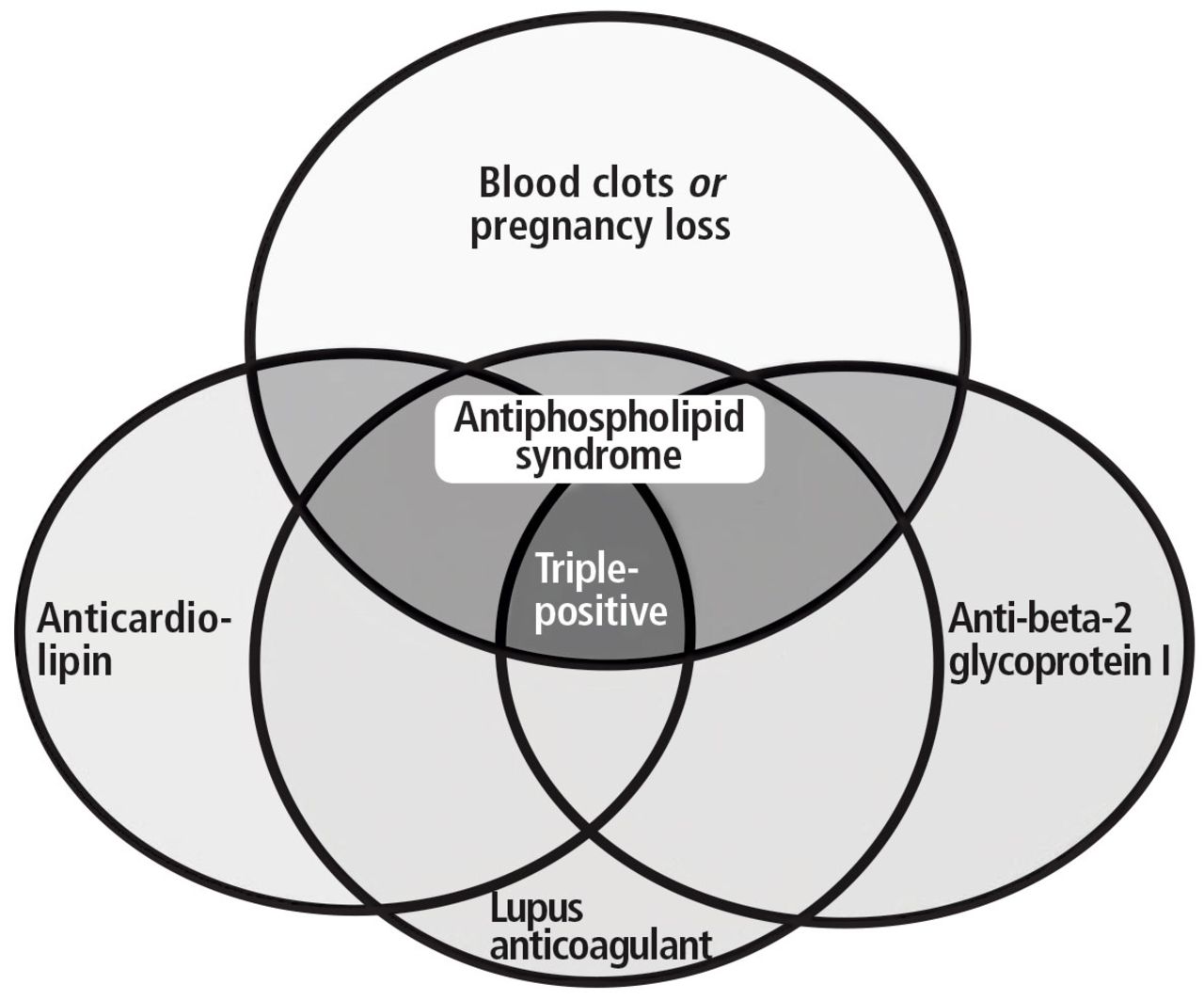
- Figure 5
Antiphospholipid antibody tests and terminology.
From Houghton DE, Moll S. Antiphospholipid antibodies. Vasc Med 2017; 22:545–550.


Tables
Test Valuea Reference range Complete blood cell count White blood cell count 15.37 3.70–11.00 × 109/L Red blood cell count 4.45 4.20–6.00 × 109/L Hemoglobin 13.7 13.0–17.0 g/dL Hematocrit 41.2 39.0%–51.0% Mean corpuscular volume 92.6 80.0–100.0 fL Mean corpuscular hemoglobin 30.8 26.0–34.0 pg Mean corpuscular hemoglobin concentration 33.3 30.5–36.0 g/dL Red blood cell distribution width 13.8 11.5%–15.0% Platelet count 204 150–400 × 109/L Mean platelet volume 11.8 9.0–12.7 fL Complete metabolic panel Protein, total 6.7 6.0–8.4 g/dL Albumin 3.1 3.5–5.0 g/dL Calcium 8.4 8.5–10.5 mg/dL Bilirubin, total 0.2 0.0–1.5 mg/dL Alkaline phosphatase 118 40–150 U/L Aspartate aminotransferase 70 7–40 U/L Glucose 112 65–100 mg/dL Blood urea nitrogen 24 10–25 mg/dL Creatinine 1.67 0.70–1.40 mg/dL Sodium 140 135–146 mmol/L Potassium 4.9 3.5–5.0 mmol/L Chloride 100 98–110 mmol/L Carbon dioxide 27 23–32 mmol/L Anion gap 13 0–15 mmol/L Alanine aminotransferase 57 5–50 U/L Estimated glomerular filtration rate 40 > 90 mL/min Cardiac biomarkers NT-proBNP 11,336 < 450 pg/mL Troponin T 0.081 0–0.029 ng/mL Creatine kinase 94 30–220 U/L Creatine kinase MB 6.4 0.0–8.8 ng/mL Coagulation profile Activated partial thromboplastin time 27.2 23.0–32.4 sec Prothrombin time 10.7 8.4–13.0 sec Prothrombin time INRx 1.1 0.8–1.2 Urinalysis Color Yellow Yellow Clarity Slightly cloudy Clear Glucose, urine Negative Negative Bilirubin, urine Negative Negative Ketones Negative Negative Specific gravity < 1.005 1.005–1.030 Hemoglobin/blood 2+ Negative pH 5.0 4.5–8.0 Protein 30 0 mg/dL Uribilinogen Normal Normal Nitrites Negative Negative Leukocyte esterase Negative Negative White blood cells 0–5 0–5/high-power field Red blood cells 6–10 0–3/high-power field ↵a Abnormal values are shown in bold. INR = international normalized ratio; NT-proBNP = N-terminal pro-B-type natriuretic peptide
Massive Sustained hypotension: systolic blood pressure < 90 mm Hg for at least 15 minutes OR requiring inotropes (cannot be due to another cause) Pulseless Persistent bradycardia (≤ 40 beats per minute with signs or symptoms of shock) Submassive Systolic blood pressure ≥ 90 mm Hg Right ventricular dysfunction or myocardial necrosis Low risk Normal blood pressure Normal biomarker levels No right ventricular dysfunction Adapted from information in reference 3.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- PREVIOUS HOSPITALIZATION
- CURRENT PRESENTATION
- WHAT DOES HIS ELECTROCARDIOGRAM SHOW?
- CLASSIFICATION OF ACUTE PULMONARY EMBOLISM
- ULTRASONOGRAPHY FOR DIAGNOSIS OF DEEP VEIN THROMBOSIS
- RISK STRATIFICATION IN ACUTE PULMONARY EMBOLISM
- ASSESSING PERIPHERAL ARTERY DISEASE
- WHAT CAN CAUSE BOTH ARTERIAL AND VENOUS THROMBOSIS?
- ANTIPHOSPHOLIPID ANTIBODY SYNDROME
- ANTIPHOSPHOLIPID ANTIBODIES ARE NOT ALL THE SAME
- PARADOXICAL EMBOLISM
- SUMMARY OF CASE
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics