


A 46-year-old man with poorly controlled hypertension presented with the sudden onset of chest pain and shortness of breath. His blood pressure was 158/96 mm Hg and his left ventricular ejection fraction was less than 20%. He was admitted to the hospital for newly diagnosed heart failure.
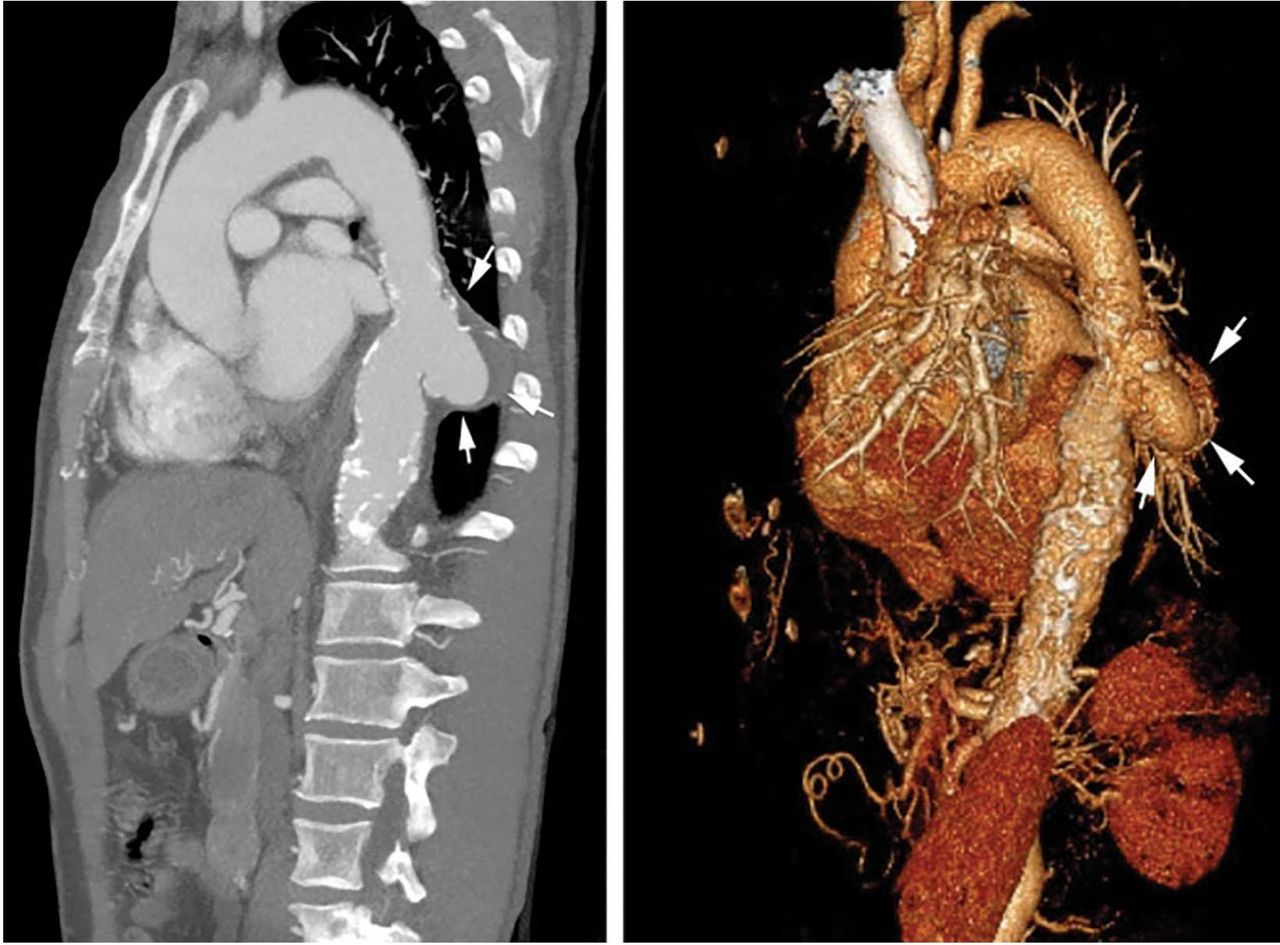
Chest radiography showed cardiomegaly, bilateral pleural effusions, and a retrocardiac masslike opacity (Figure 1). Computed tomographic angiography revealed the opacity to be a saccular aneurysm of the descending thoracic aorta measuring 6.3 × 3.7 cm, with intimal calcifications and chronic intramural hemorrhage (Figure 2). The descending thoracic aorta was heavily calcified.

Radiography showed cardiomegaly, bilateral pleural effusions, and a retrocardiac masslike opacity (arrows).
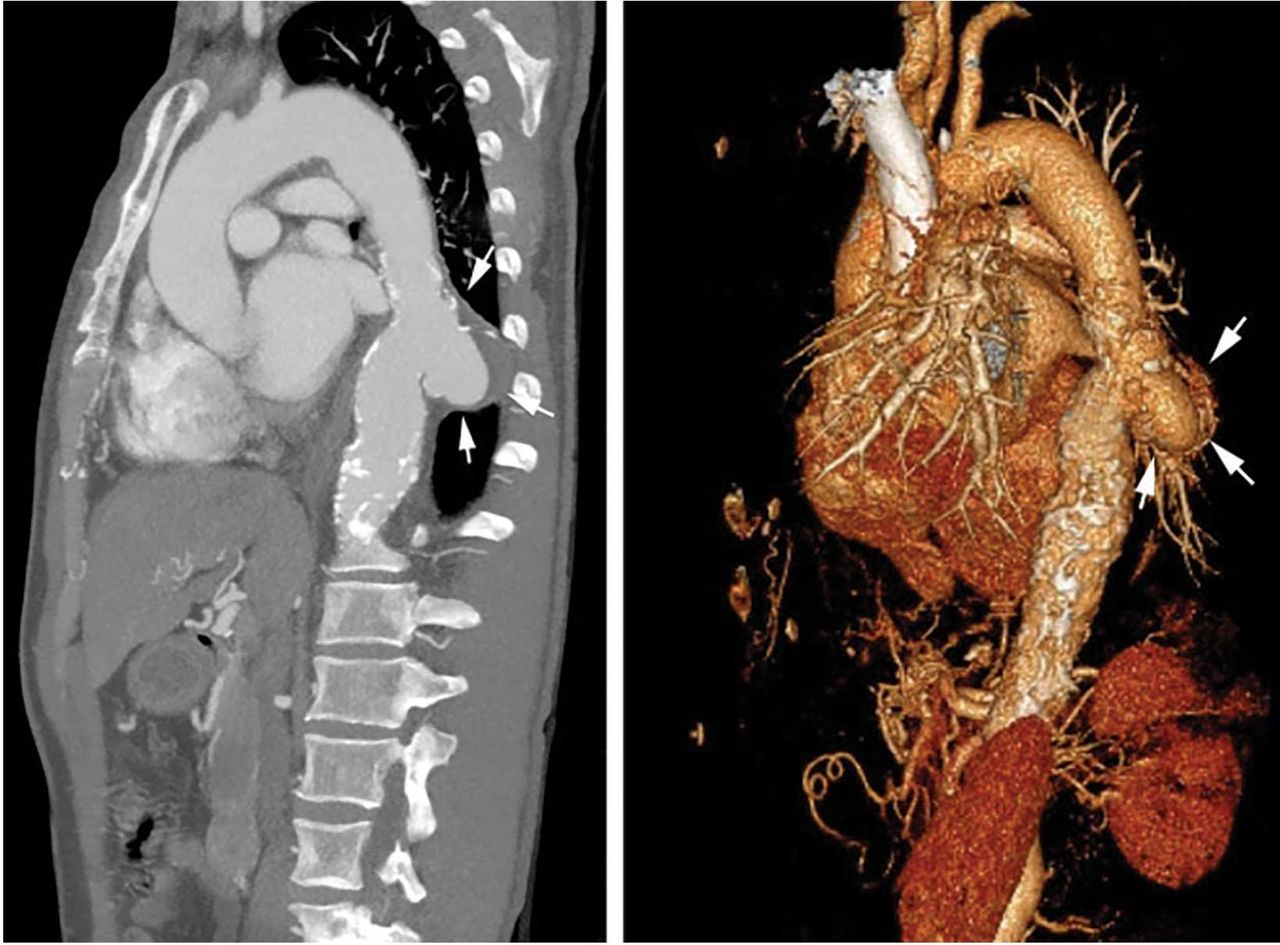
Computed tomographic angiography (sagittal view) and a 3-dimensional rendering show an aorta with intimal calcifications and chronic intramural hemorrhage (arrows).
The patient then underwent cardiac catheterization, which revealed triple-vessel coronary artery disease. A cardiothoracic surgeon recommended coronary artery bypass grafting with aneurysm repair. However, the patient declined surgery and instead chose medical therapy. His blood pressure was under control at the time of discharge.
SACCULAR AORTIC ANEURYSMS
This case shows the value of carefully examining the chest radiograph, especially behind the heart.
Saccular aneurysms of the descending thoracic aorta are rare and can be easily missed if asymptomatic. They are less common than fusiform aneurysms and may be more prone to rupture. Shang et al1 identified atherosclerosis as the most frequent cause of saccular aneurysms of the thoracic aorta. However, they can be caused by other inflammatory conditions and infections.1
Without surgical repair, thoracic aortic aneurysms larger than 6 cm have higher rates of expansion and rupture (a 20% 6-year cumulative risk) than smaller ones.2 Mid-descending aortic aneurysms expand faster than those of the ascending aorta.3
Indications for surgery include rupture, severe chest pain, compressive symptoms, large size (eg, ≥ 5.5 cm for asymptomatic descending thoracic aneurysms), and rapid growth rate (≥ 10 mm per year), all of which are associated with a higher mortality rate.4
Endovascular grafting should be strongly considered in patients who have significant comorbidities, but this approach may have poorer long-term outcomes compared with open surgery. Blood pressure should be lowered as far as the patient can tolerate without adverse effects, usually with a beta-blocker along with either an angiotensin-converting enzyme inhibitor or an angiotensin receptor blocker.4
Statin therapy to lower the low-density lipoprotein cholesterol level to less than 70 mg/dL is also needed to reduce the risk of complications and cardiovascular disease.
All patients with saccular aortic aneurysm should be followed closely and be evaluated for surgery.
- Copyright © 2018 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.