


Article Figures & Data
Figures
- Figure 1
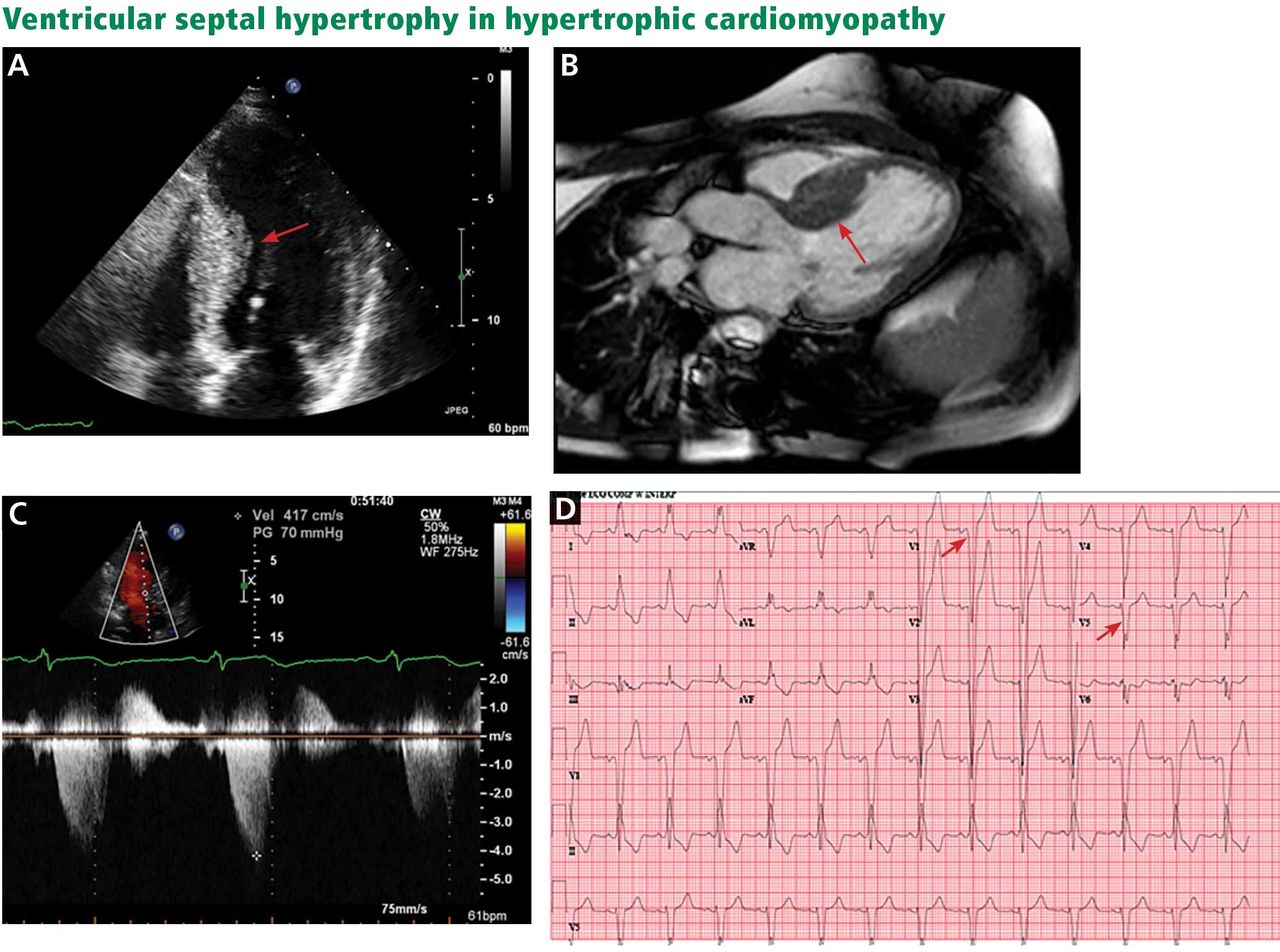
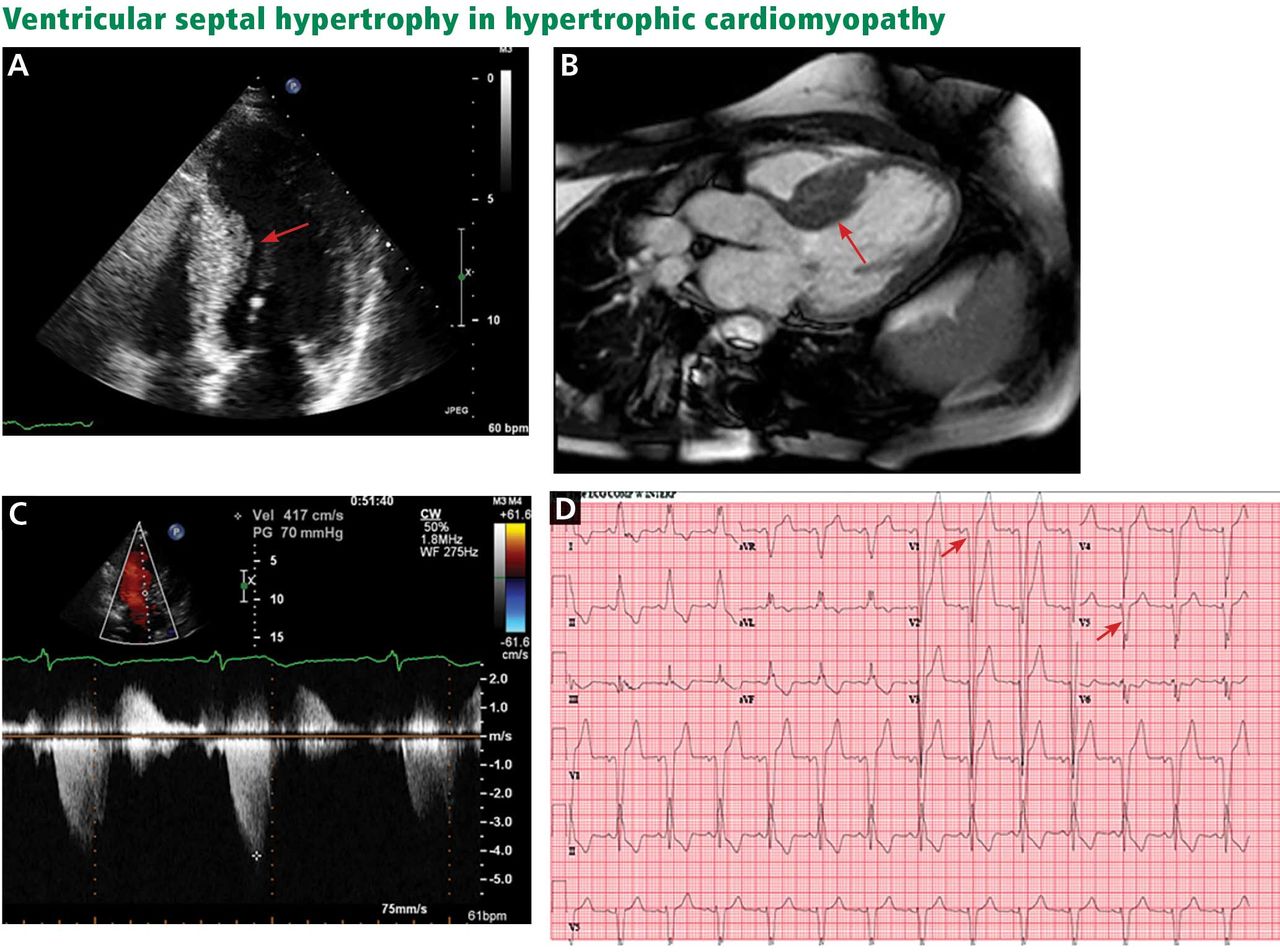
A, echocardiography, apical 4-chamber view, demonstrates septal hypertrophy (arrow). B, cardiac magnetic resonance imaging of the left ventricular outflow tract also demonstrates septal hypertrophy (arrow). C, echocardiography with continuous-wave Doppler across the left ventricular outflow tract demonstrates a gradient of 70 mm Hg, consistent with obstruction. D, electrocardiography reveals signs of left ventricular hypertrophy by Sokolov-Lynon criteria with S wave depth in V1 plus R wave height in V5 > 35 mm (arrows).
- Figure 2
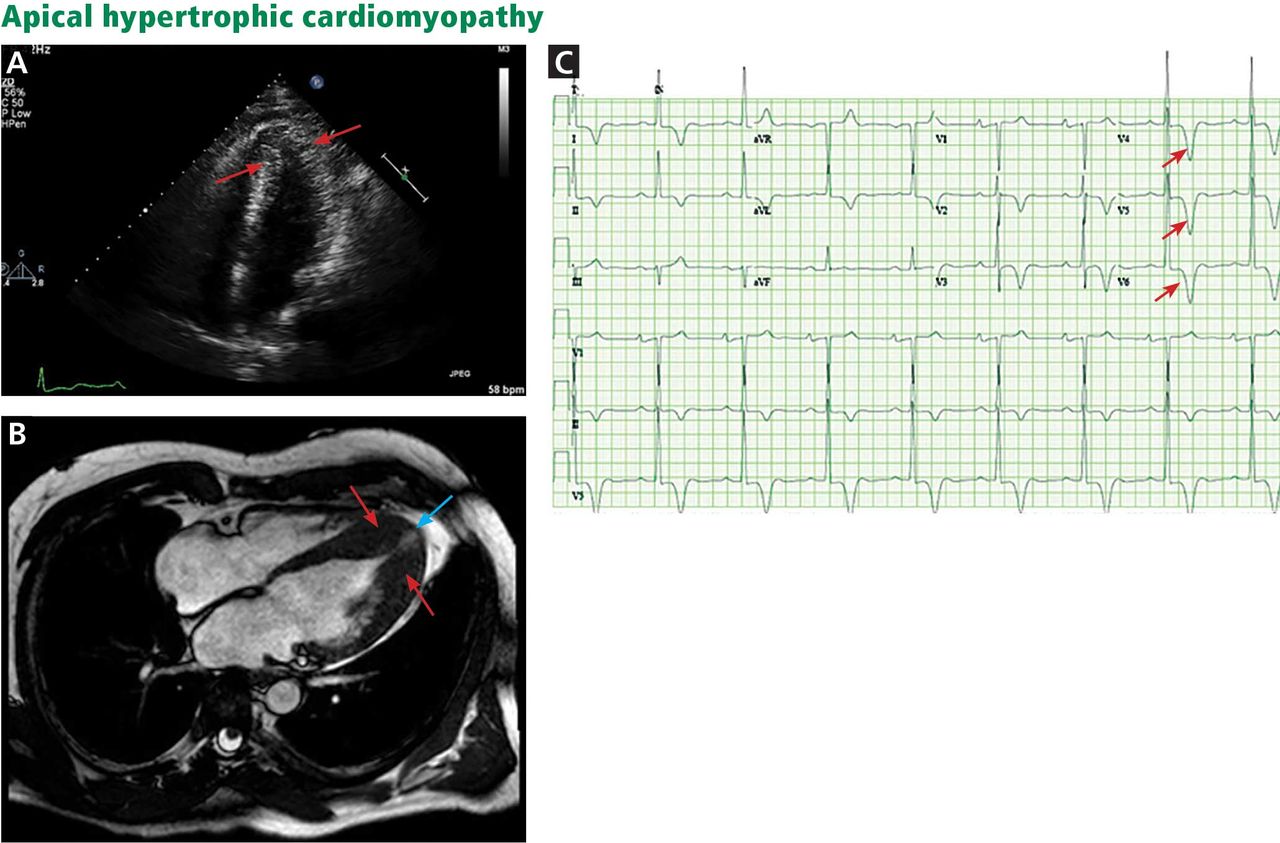
A, echocardiography, apical 4-chamber view, shows apical hypertrophy (arrows). B, cardiac magnetic resonance imaging (4-chamber view) shows apical hypertrophy (red arrows), as well as an apical aneurysm (blue arrow). C, electrocardiography demonstrates giant T-wave inversions in the left precordial leads, characteristic of apical hypertrophic cardiomyopathy (arrows).
- Figure 3
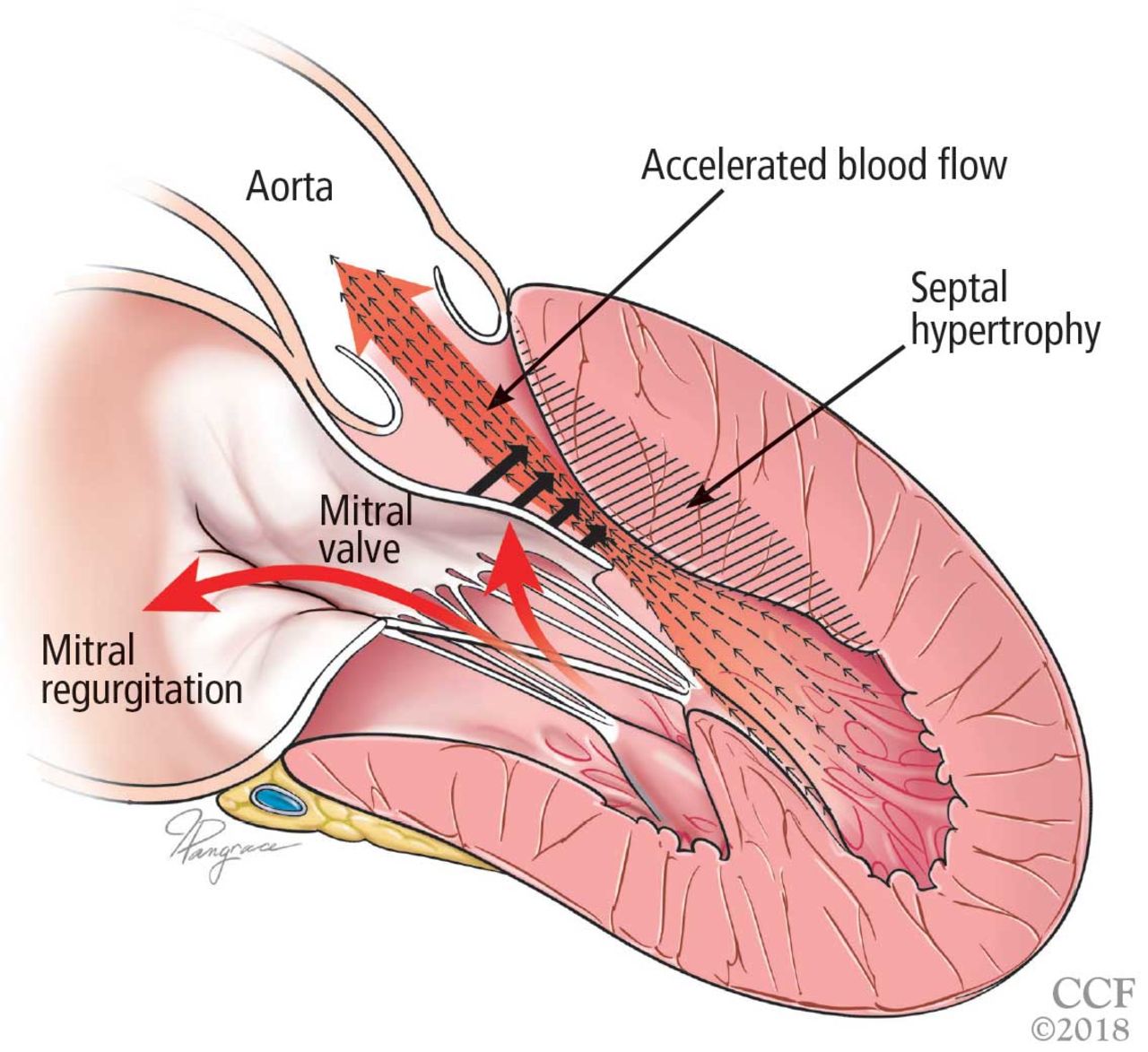
Left ventricular outflow tract obstruction due to ventricular septal hypertrophy. The obstruction is dynamic, as the blood flow sweeps the mitral valve toward the septum.
- Figure 4
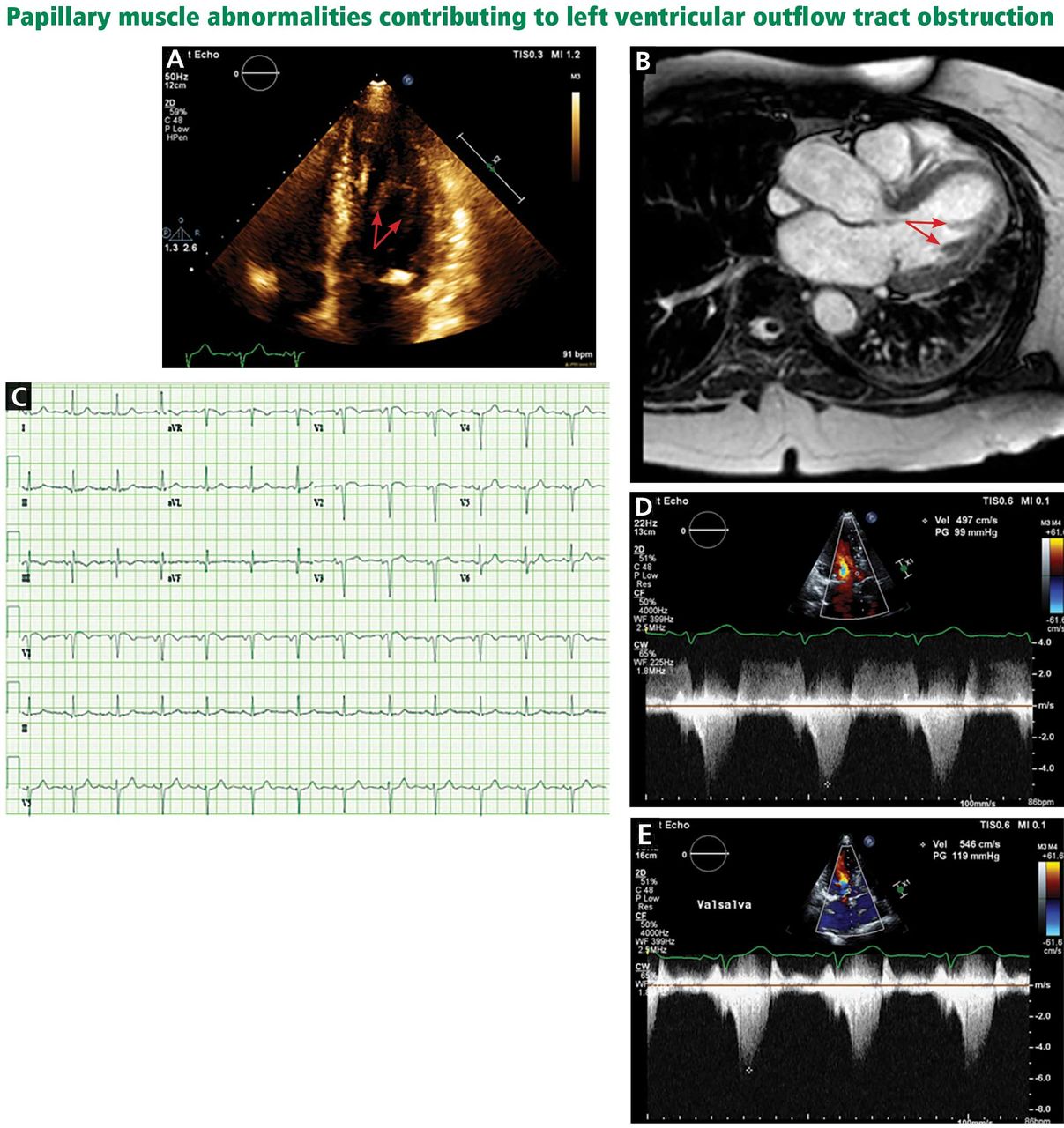
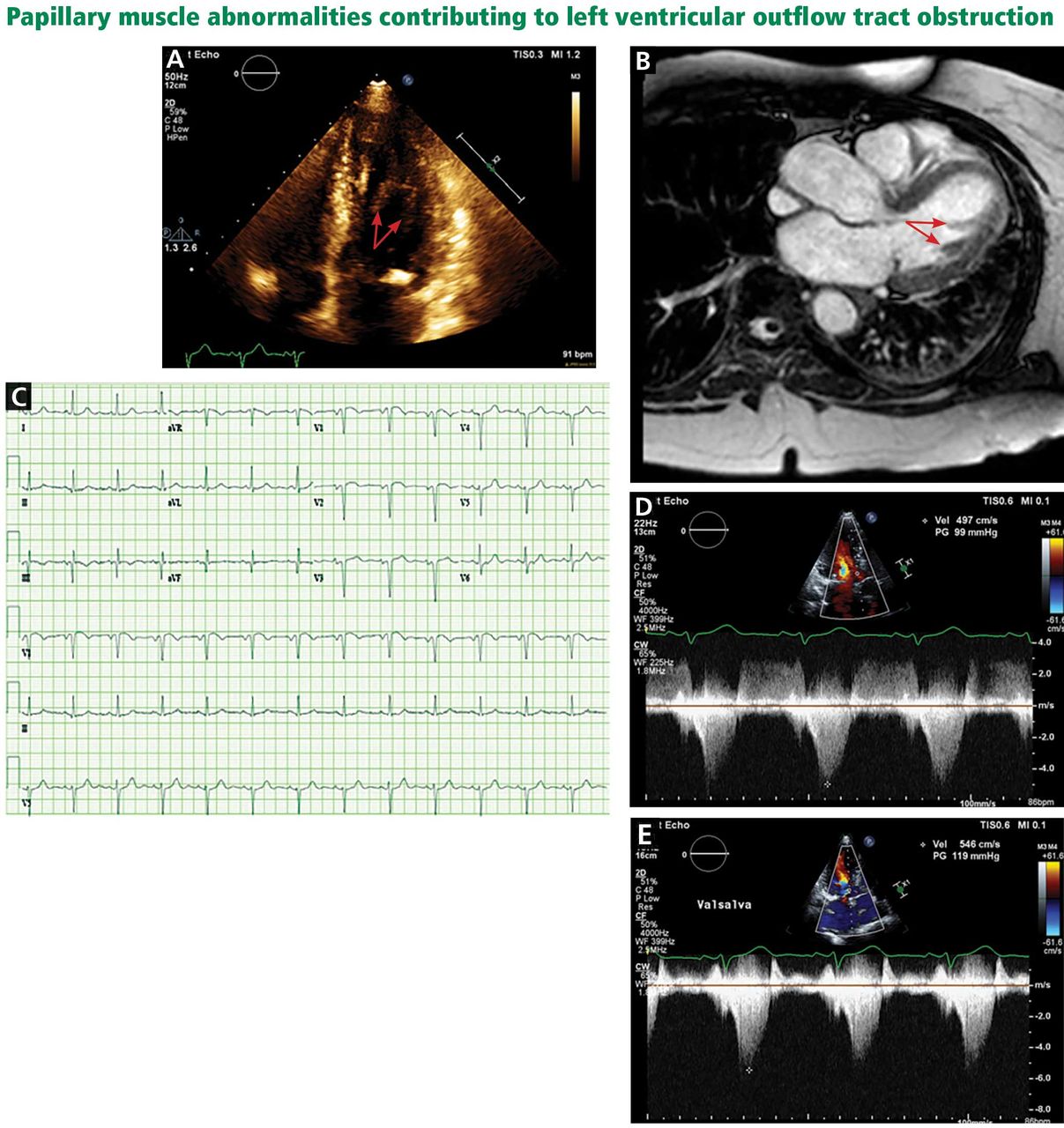
A, echocardiography, apical 4-chamber view, demonstrates a bifid papillary muscle resulting in left ventricular outflow tract obstruction (arrows). B, cardiac magnetic resonance imaging (left ventricular outflow tract view) demonstrates a bifid papillary muscle (arrows). C, an electrocardiogram of a patient with obstruction related to abnormal papillary muscle morphology demonstrates a lack of significant left ventricular hypertrophy. D, continuous-wave Doppler through the left ventricular outflow tract demonstrates a peak gradient of 99 mm Hg, consistent with obstruction, which increases with the Valsalva maneuver to 119 mm Hg (E).
- Figure 5
Left ventricular outflow tract (LVOT) obstruction without significant left ventricular hypertrophy. The prominent bifid papillary muscles lead to systolic anterior motion of the mitral valve, causing LVOT obstruction and simultaneous mitral regurgitation.
- Figure 6
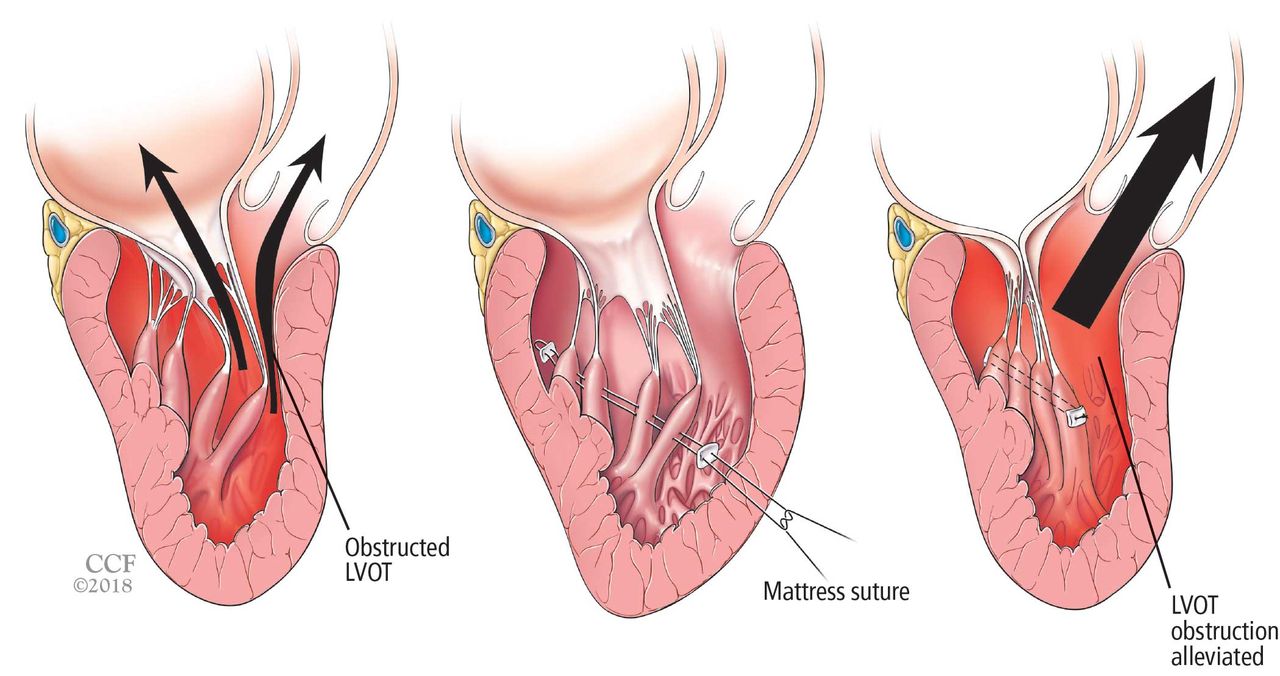
Reorientation surgery reduces mobility of bifid hypermobile papillary muscles, reducing left ventricular outflow tract (LVOT) obstruction.


Tables
Hypertensive cardiomyopathy Aortic valvulopathy
Aortic stenosis
Supra-aortic or subaortic membranesInfiltrative cardiomyopathy
Amyloidosis
Fabry disease
Lysosomal diseases (eg, Danon disease)
Glycogen storage disorders (eg, Pompe disease)Hemochromatosis ‘Athlete’s heart’ Noncompaction cardiomyopathy Sarcomeric proteins Gene Gene prevalence in HCM probands Myosin-binding protein C MYPBC3 15% Beta myosin heavy chain MYH7 15% Cardiac troponin T TNNT2 7% Alpha-tropomyosin TPM1 7% Regulatory myosin light chain MYL2 < 5% Essential myosin light chain MYL3 < 5% Cardiac troponin I TNNI3 < 5% Nonsarcomeric proteins Gene Inheritance Associated phenotype Transthyretin TTR Dominant; 1%–10% Amyloidosis Lysosome-associated membrane glycoprotein 2 LAMP2 X-linked; rare Danon disease Alpha-galactosidase A GLA X-linked; 1%–2% of males Fabry disease Lysosomal alpha-glucosidase GAA Recessive; rare Pompe disease Frataxin FXN Recessive; rare Friedrich ataxia Based on information in reference 3.
- TABLE 3
Risk-stratification models for primary prevention of sudden cardiac death in hypertrophic cardiomyopathy
North American model European model An implantable cardioverter-defibrillator (ICD) is reasonable (class IIa recommendation, level of evidence C—limited evidence) if any of the following are present: Family history of sudden death
Unexplained syncope
Maximum left ventricular wall thickness ≥ 30 mm
Or if the patient has any other risk factor or modifier for sudden cardiac death and either of the following:Nonsustained ventricular tachycardia
Abnormal blood pressure response during exercise (decrease or failure to increase systolic blood pressure ≥ 20 mm Hg during exercise stress test)
The following factors are used to electronically calculate the 5-year risk of sudden cardiac death: Family history of sudden death
Unexplained syncope
Maximum left ventricular wall thickness
Nonsustained ventricular tachycardia
Age
Left atrial diameter
Left ventricular outflow gradient
5-year risk < 4%: an ICD is generally not indicated
5-year risk ≥ 4% to < 6%: an ICD may be considered
5-year risk ≥ 6%: an ICD should be consideredBased on information in references 9 and 30.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}