


Article Figures & Data
Figures
- Figure 2
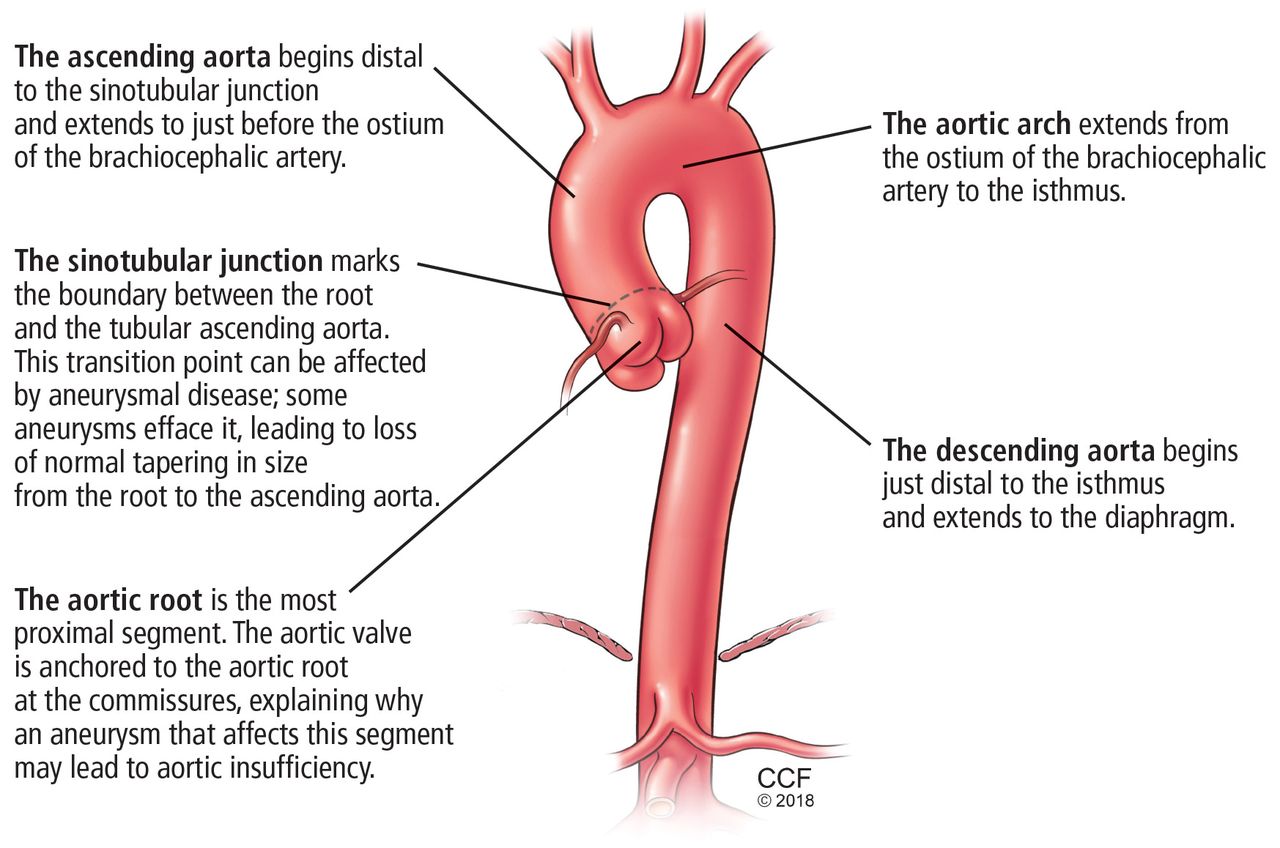
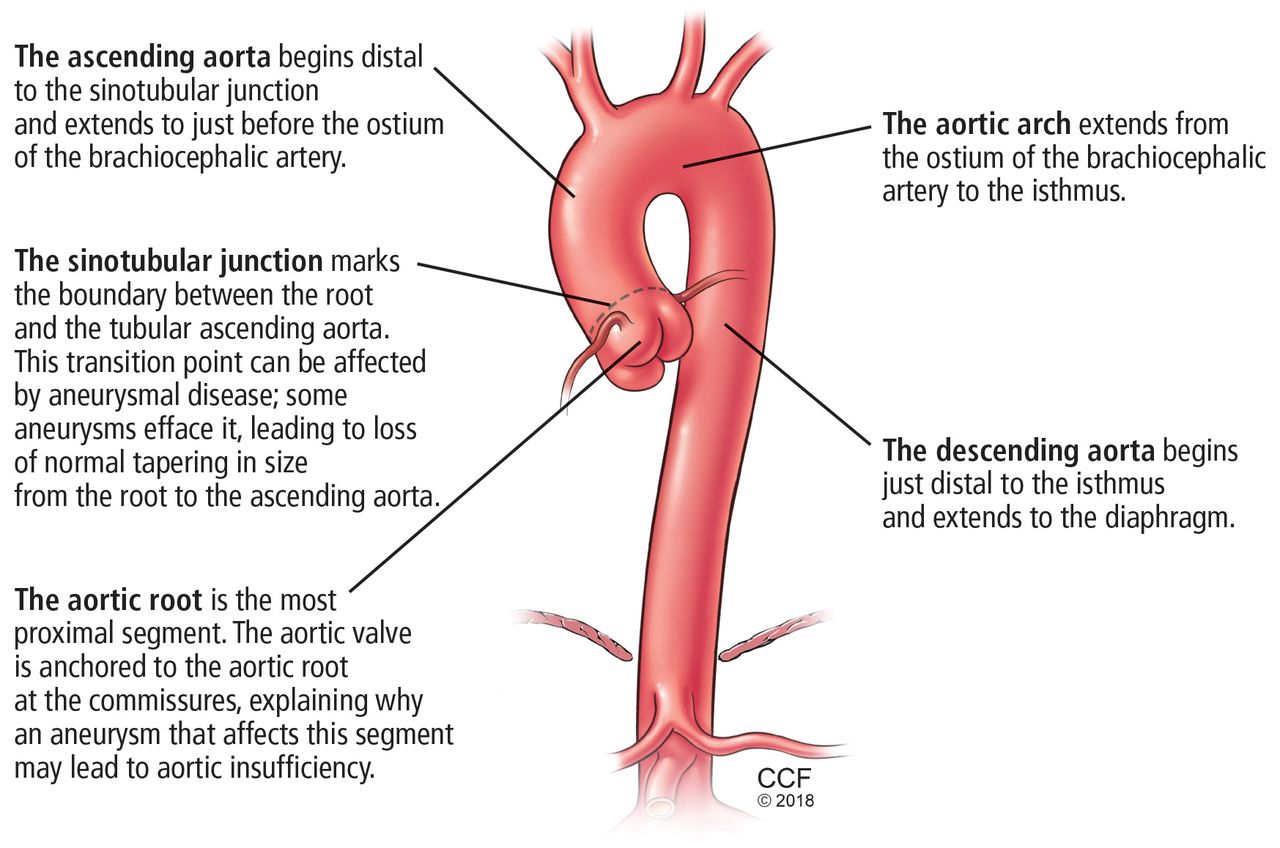
Echocardiographic image of an aneurysmal aortic root (white arrow) that tapers to normal dimensions at the sinotubular junction (yellow arrow) and ascending aorta. See videos (this image and a bicuspid aortic valve).
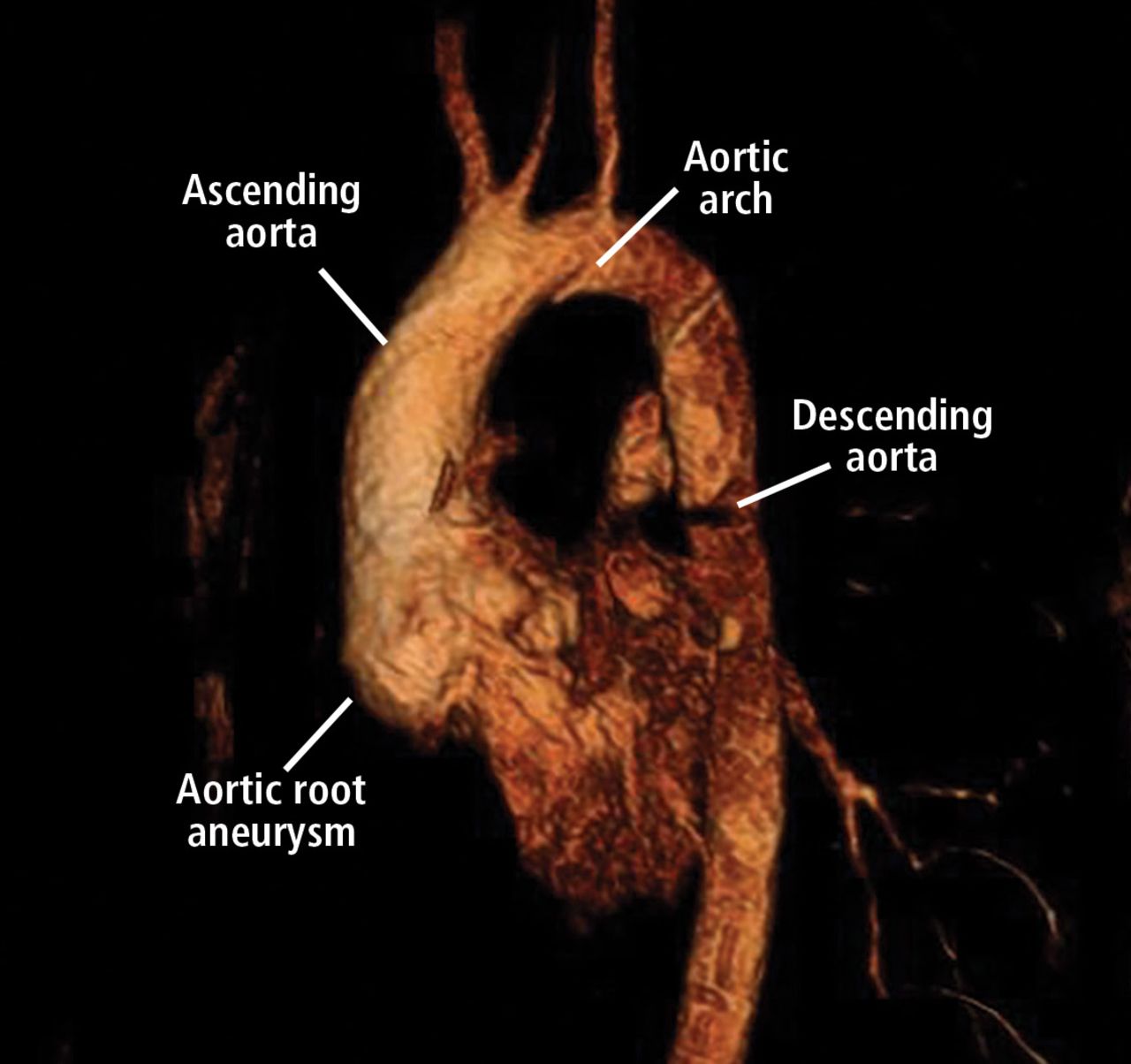
- Figure 3
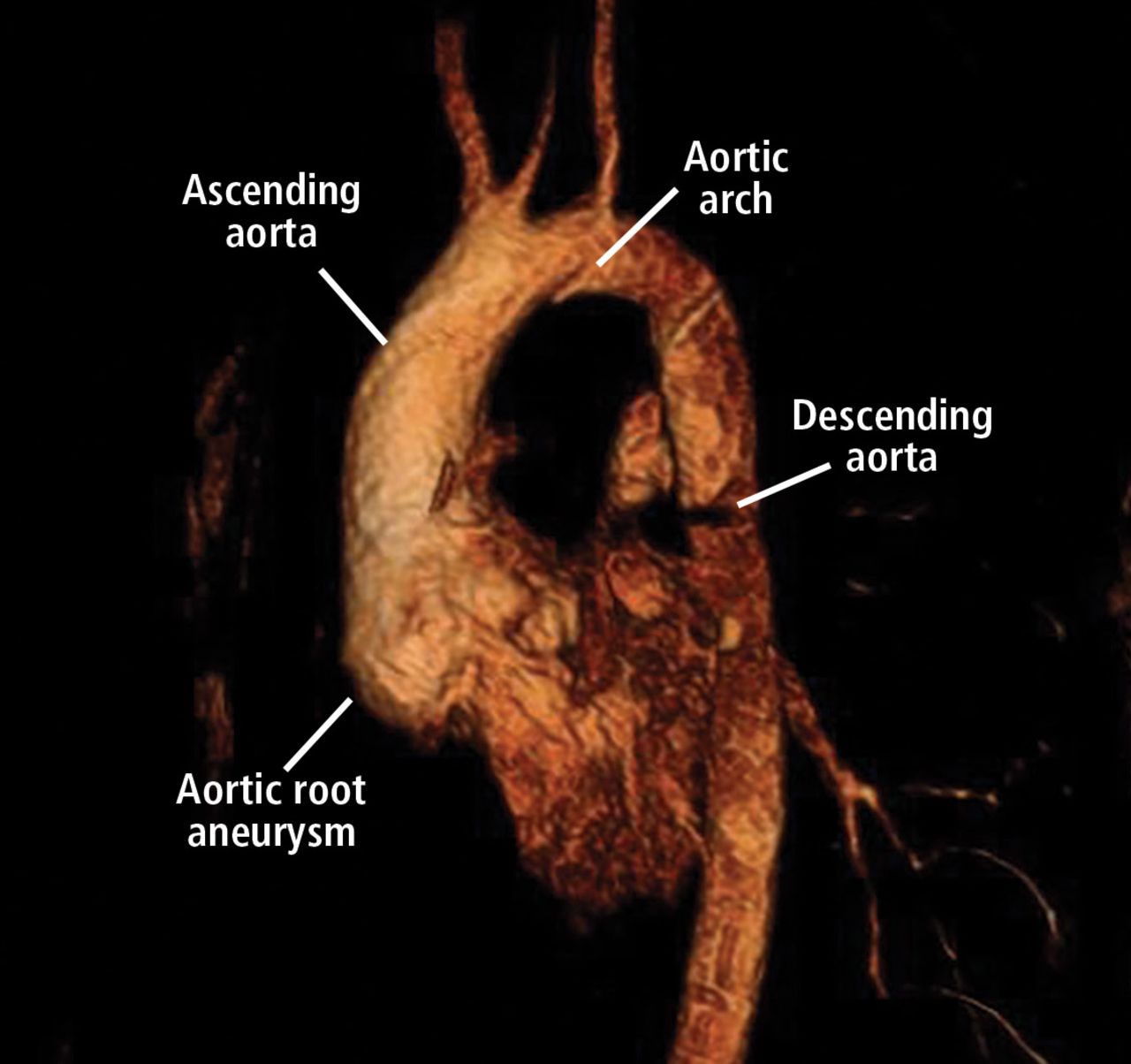
An aortic root aneurysm in a patient with Mar-fan syndrome using magnetic resonance angiography. See videos (this image, follow-up after surgical repair, and a computed tomographic study).
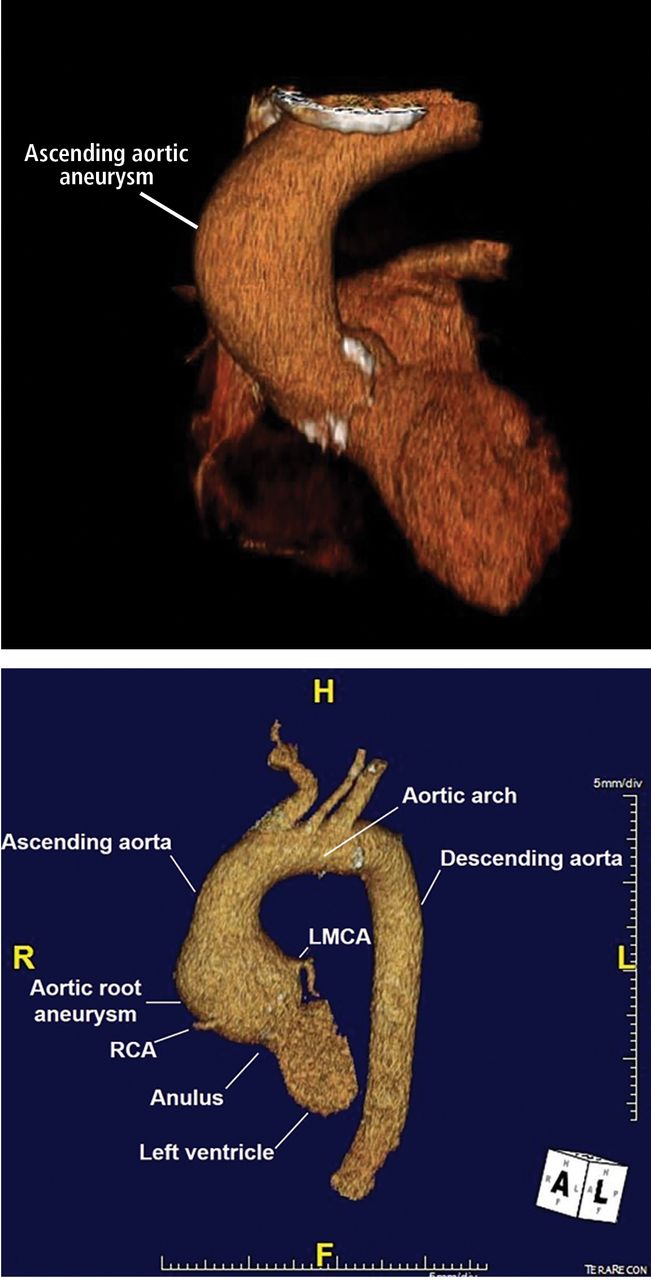
- Figure 4
Top, 3D reconstruction of an ascending aortic aneurysm in a patient with a bicuspid aortic valve. See video. Bottom, 3D reconstruction of a young patient with an aortic root aneurysm. Note the tapering from the aneurysmal aortic root to the normalsized ascending aorta. LMCA = left main coronary artery; RCA = right coronary artery.
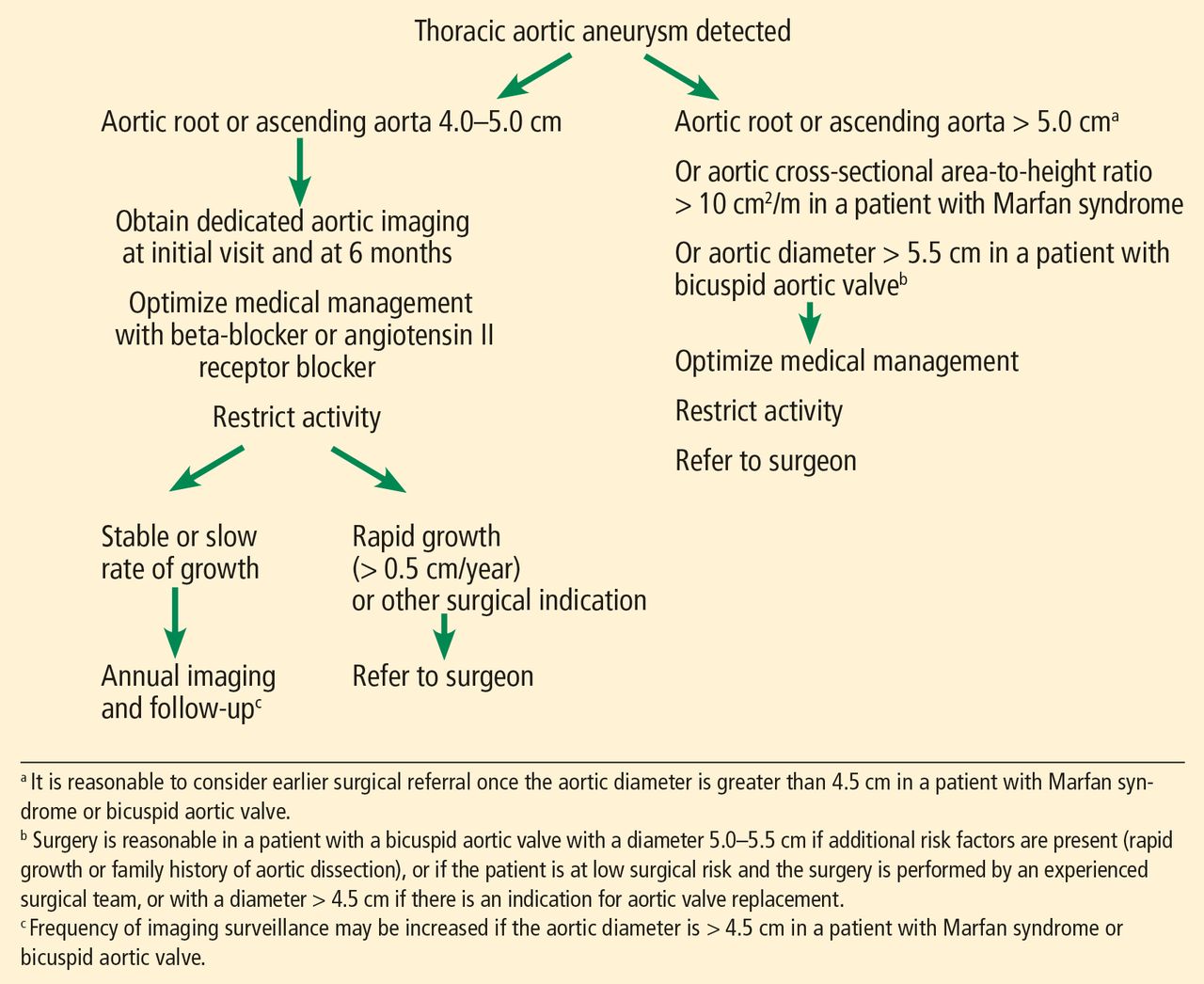
- Figure 5
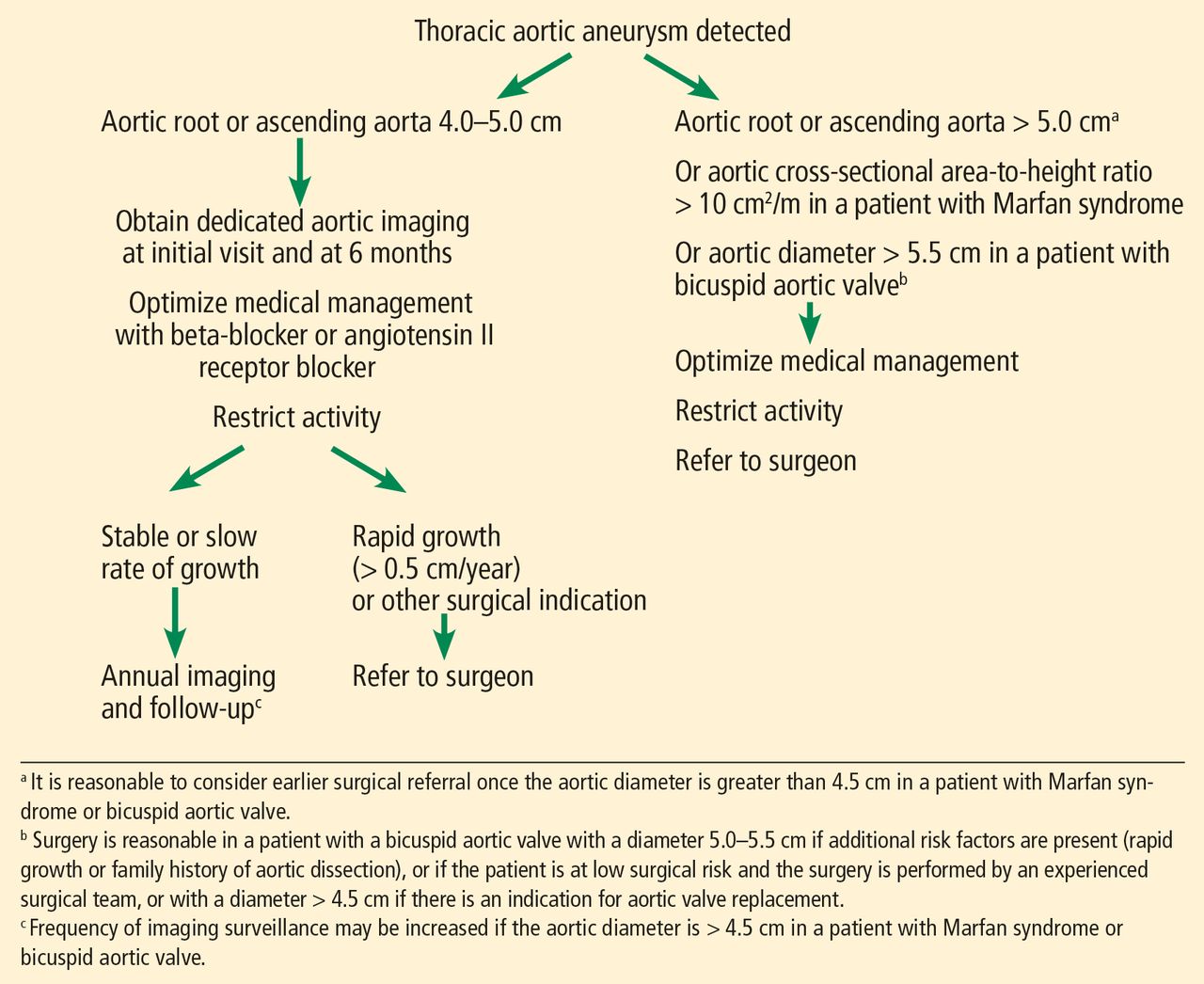
Initial screening and follow-up of thoracic aortic aneurysm.


Tables
Age (years) BSA (m2) Ascending aorta (mm) Descending aorta (mm) Women (n = 1,147) Men (n = 1,805) Women (n = 736) Men (n = 1,195) < 45 < 1.70 33.8 33.0 23.0 NA 1.70–1.89 34.4 36.3 24.6 26.6 1.90–2.09 35.0 36.3 22.7 26.7 > 2.1 NA 38.3 NA 28.3 45–54 < 1.70 35.2 38.6 24.3 24.2 1.70–1.89 37.2 38.1 25.4 27.5 1.90–2.09 38.9 39.7 27.2 29.2 > 2.1 40.6 40.6 28.3 29.6 55–64 < 1.70 36.9 36.3 25.9 26.1 1.70–1.89 37.0 39.7 27.1 28.6 1.90–2.09 39.0 41.2 27.8 29.9 > 2.1 42.0 43.1 31.7 31.6 ≥ 65 < 1.70 37.5 38.5 27.0 NA 1.70–1.89 39.2 41.0 27.4 32.4 1.90–2.09 42.7 42.2 29.0 31.0 > 2.1 NA 42.4 29.8 32.5 ↵a Upper limits of normal are 2 standard deviations above the mean. Not calculated if there were fewer than 6 patients in a group. BSA = body surface area; NA = not available
Information from Wolak A, Gransar H, Thomson LE, et al. Aortic size assessment by noncontrast cardiac computed tomography: normal limits by age, gender, and body surface area. J Am Coll Cardiol Cardiovasc Imaging 2008; 1(2):200–209. doi:10.1016/j.jcmg.2007.11.005
Idiopathic Bicuspid aortic valve Genetic syndromes
Marfan syndrome
Loeys-Dietz syndrome
Ehlers-Danlos syndrome
Familial thoracic aortic aneurysm and dissection
Autosomal dominant polycystic kidney disease
Turner syndromeInflammatory vasculitis
Takayasu arteritis
Giant cell arteritis
Behçet arteritis
Ankylosing spondylitisOther
Atherosclerosis
Syphilis
Previous dissection
Infectious aortitis
TraumaRisk factors
Hypertension
Smoking
Advanced ageInherited condition Implicated gene Clinical features Marfan syndrome FBN1 Aneurysm of aortic root, dilation of pulmonary artery, and aortic dissection Ehlers-Danlos syndrome COL5A1, COL5A2, COL3A1 Arterial mid-sized rupture, especially involving thoracic vasculature Loeys-Dietz syndrome TGFBR1, TGFBR2, SMAD3, TGFB2, TGFB3 Premature and aggressive aneurysm and dissection; aneurysm may involve aortic segments other than the root Familial thoracic aortic aneurysm and dissection ACTA2, MYH11, PRKG1, MYLK, TGFBR2 Thoracic aortic aneurysm and dissection; associated vascular disease (eg, patent ductus arteriosus) Bicuspid aortic valve Unknown (may be associated with ACTA2, MYH11, syndromic connective tissue diseases) Aortic dilation typically involving the aortic root and ascending aorta Autosomal dominant polycystic kidney disease PKD1, PKD2 Dilation of the aorta and thoracic aortic dissection Turner syndrome 45,X Thoracic aortic aneurysms and dissections, bicuspid aortic valve, aortic coarctation Reprinted from Cury M, Zeidan F, Lobato AC. Aortic disease in the young: genetic aneurysm syndromes, connective tissue disorders, and familial aortic aneurysms and dissections. Int J Vasc Med 2013(2013); 2013:267215. doi:10.1155/2013/267215
Imaging study Advantages Disadvantages Cardiac-gated multidetector computed tomographic angiography Highly specific and sensitive Can diagnose vascular anomalies, tortuosity Large doses of ionizing radiation and contrast Magnetic resonance angiography Highly specific and sensitive Can be accurate without using contrast Ability to assess valve disease Prolonged scanning time Difficult for those with claustrophobia Transthoracic echocardiography Noninvasive, readily available Can assess valve disease Limited visualization of ascending aorta Accuracy reduced with “oblique” measurements Transesophageal echocardiography Highly specific and sensitive Ability to assess valve disease Requires skilled personnel Invasive, requires procedural sedation Angiography Highly sensitive and specific Invasive Requires contrast Based on Smith AD, Schoenhagen P. CT imaging for acute aortic syndrome. Cleve Clin J Med 2008; 75(1):7–17. pmid:18236724




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- ABSTRACT
- LIKELY UNDERDETECTED
- RISK FACTORS FOR THORACIC AORTIC ANEURYSM
- DIAMETER INCREASES WITH AGE, BODY SURFACE AREA
- HOW IS TAA DIAGNOSED?
- HOW IS TAA CLASSIFIED?
- HOW IS ANEURYSM MANAGED ON AN OUTPATIENT BASIS?
- WHEN SHOULD A PATIENT BE REFERRED?
- WHEN SHOULD TAA BE REPAIRED?
- HOW SHOULD PATIENTS BE SCREENED? WHAT FOLLOW-UP IS NECESSARY?
- BACK TO OUR PATIENT WITH A BICUSPID AORTIC VALVE
- BACK TO OUR PATIENT WITH MARFAN SYNDROME
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics