


Article Figures & Data
Figures
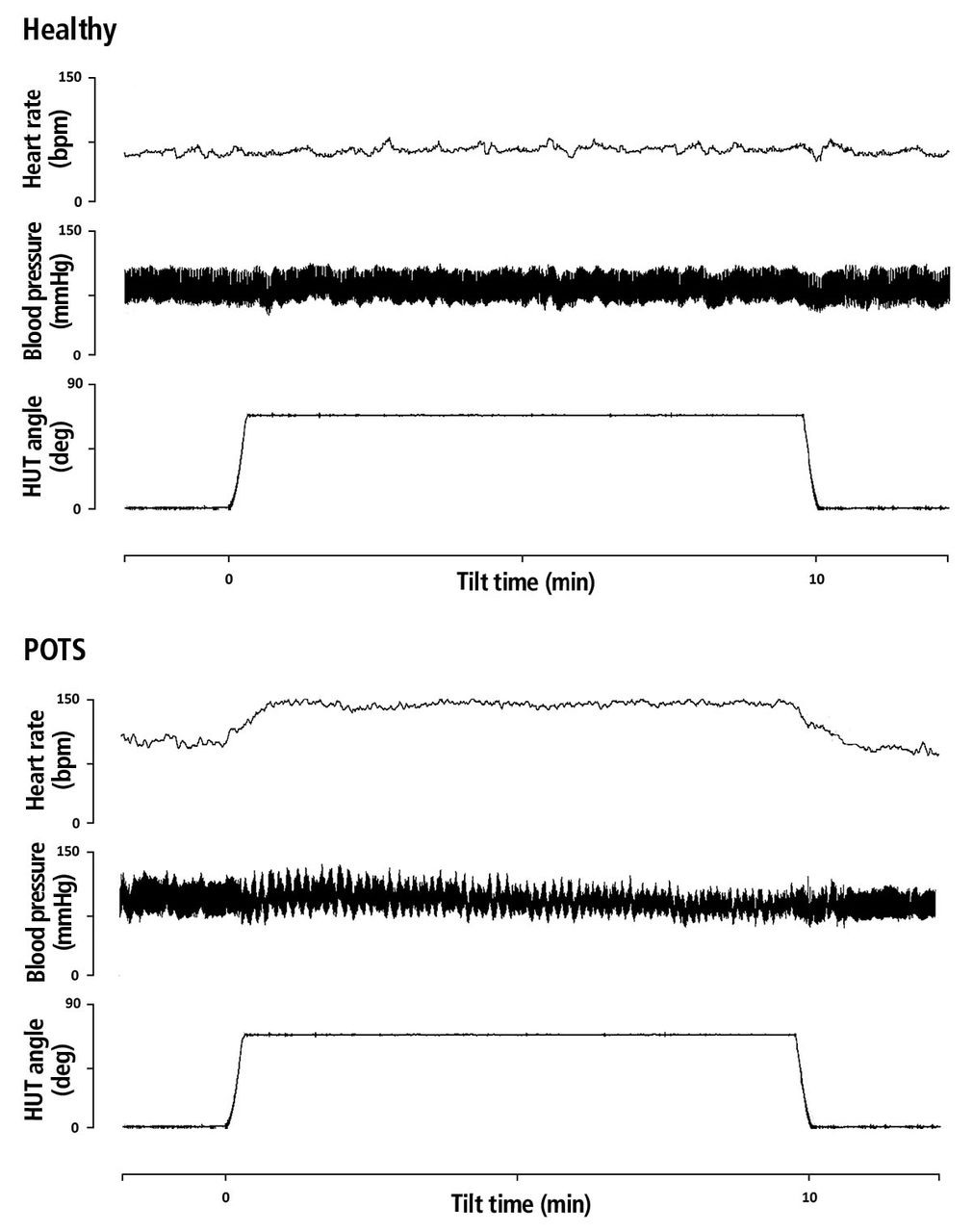
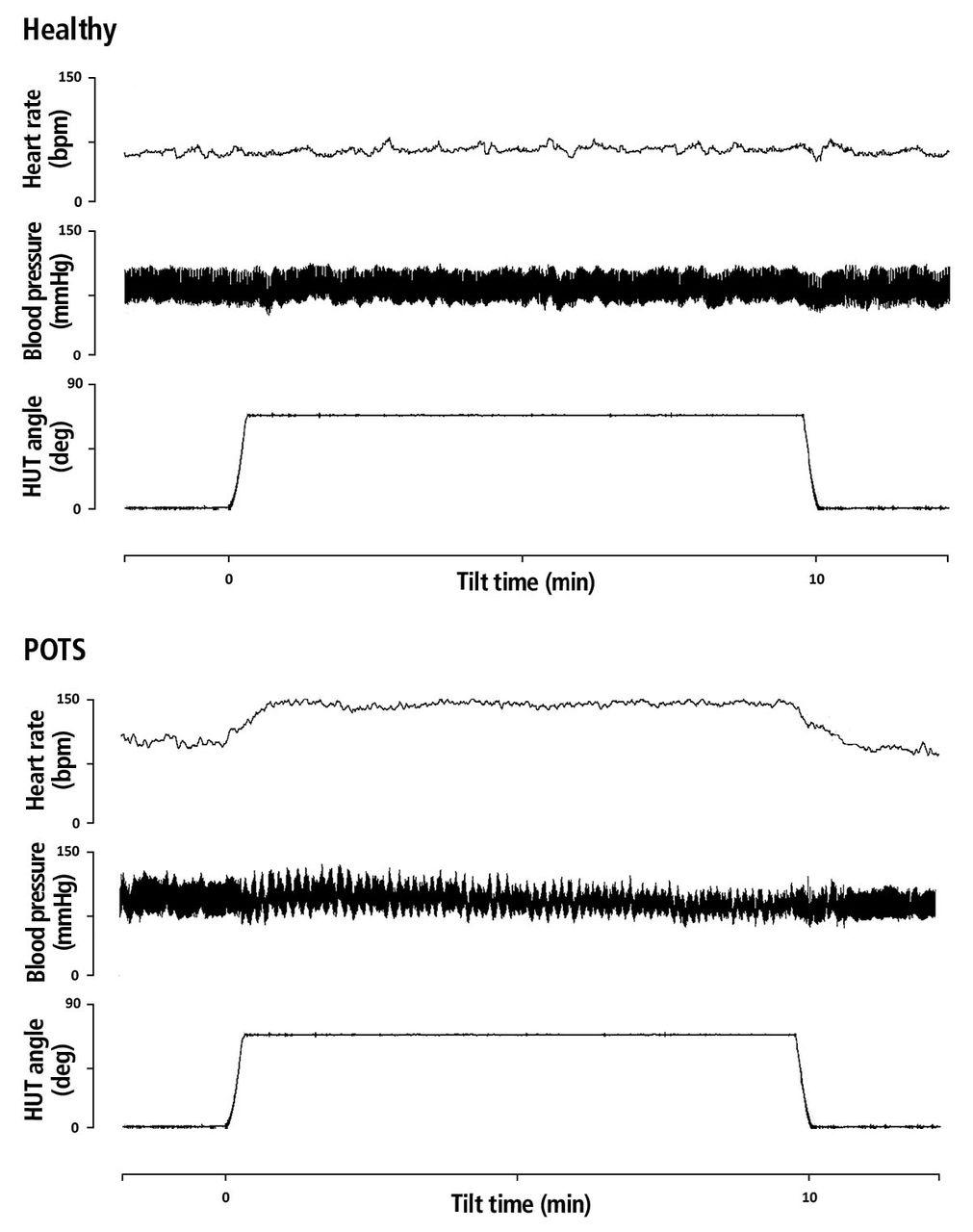
- Figure 1
Results of head-up tilt-table (HUT) testing in a healthy person (top) and in a patient with postural tachycardia syndrome (POTS) (bottom). Upon passive head-up tilting, the heart rate increases in POTS by at least 30 bpm but remains largely stable in healthy individuals. Ortho-static hypotension (a fall in blood pressure of ≥ 20/10 mm Hg) does not occur in either patient.
Tables
Cardiac symptoms Palpitations Lightheadedness Chest discomfort Dyspnea Noncardiac symptoms Mental clouding (“brain fog”) Headache Nausea Tremulousness Blurred or tunnel vision Sleep disturbances Fatigue Presyncope Gastrointestinal pain, heartburn, diarrhea, constipation Hyperthyroidism Infection Pheochromocytoma Inappropriate sinus tachycardia Acute dehydration Exercise Physical deconditioning Panic attacks Pain Alcohol Caffeine Medication-induced or exacerbated Information from references 39–41.
Therapy Dosage Pathologic mechanisms addressed Potential drawbacks Comments Exercise ≥ 30 min at least 3 times a week All Worsened symptoms at the outset, prolonged fatigue Gradually progress from non-upright to upright endurance and resistance exercises Dietary fluid 2–3 L per day All Hyponatremia Dietary salt 10–12 g per day All Difficult to augment sufficiently through diet alone Supplement with sodium chloride tablets, if necessary Salt tablets 1 g tablet 3 times daily Hypovolemia Poor taste, nausea, dyspepsia Recommended for use after meals Acute intravenous normal saline 1 L over 1–3 hours Hypovolemia Inconvenient, medical setting required Heart Rhythm Society Consensus Statement class IIa recommendation (benefit probably exceeds risk) Chronic intravenous normal saline 1 L every 2 days Hypovolemia Access complications and infection with central line Heart Rhythm Society Consensus Statement class III recommendation (recommends against) Antidepressants (serotonin-norepinephrine reuptake inhibitors, monoamine oxidase inhibitors, and tricyclic antidepressants at higher doses) Antipsychotic agents (phenothiazines) Anxiolytic agents Attention deficit medications Diuretics Venodilators and vasodilators Stimulants (including caffeine, nicotine) Therapy Dosage Pathologic mechanism addressed Potential drawbacks Comments Blood volume expanders Fludrocortisone 0.05–0.1 mg
twice dailyHypovolemia Hypokalemia, hypertension, fatigue, headache, fluid retention, edema Desmopressin 0.1–0.2 mg
3 times dailyHypovolemia Hyponatremia, headache, edema Only for occasional use; must monitor blood sodium Erythropoietin 2,000–3,000 IU subcutaneously
1–3 times per weekHypovolemia High cost, requires injection, risk of vascular complications Reserved for patients with symptoms refractory to more common treatments Heart rate-lowering agents Propranolol 10–20 mg
3–4 times dailyAll Hypotension, fatigue, drowsiness, wheezing Not well tolerated at higher dosages Ivabradine 5–7.5 mg
twice dailyAll Palpitations, headache, dizziness, constipation Central nervous system sympatholytics Clonidine 0.05–0.2 mg
twice dailyHyperadrenergic Mental clouding, fatigue, drowsiness, constipation Can be associated with rebound hypertension and tachycardia Methyldopa 125 mg
once or twice dailyHyperadrenergic Hypotension, fatigue, headache, drowsiness, constipation Rare lupus-like syndrome reported Other drugs Midodrine 5–15 mg
every 4 hours, 3 times daily onlyNeuropathic Hypertension, goose bumps, urinary retention Not recommended for use within 4-5 hours of sleep Pyridostigmine 30–60 mg
3 times dailyAll Abdominal cramping, diarrhea, increased sweating May increase gastrointestinal motility Droxidopa 100–600 mg
3 times dailyAll Nausea, palpitations, urinary symptoms May worsen tachycardia Modafinil 100–200 mg
twice daily“Brain fog” Headache, dizziness, anxiety, insomnia May improve cognitive symptoms




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.