


A 20-year-old man with a 1-year history of untreated hypertension presented to the emergency department for evaluation and management of a hypertensive emergency. During the past 3 weeks, he had progressively worsening headaches, and on the day of presentation, his blood pressure was 184/154 mm Hg. Results of initial laboratory testing were as follows:
Sodium 132 mmol/L (reference range 136– 144)
Potassium 3.1 mmol/L (3.7–5.1)
Chloride 86 mmol/L (97–105)
Bicarbonate 34 mmol/L (22–30)
Blood urea nitrogen 14 mg/dL (9–24)
Creatinine 1.2 mg/dL (0.73–1.22)
Albumin 4.9 g/dL (3.4–4.9).
Urinalysis showed no hematuria or proteinuria. Plasma aldosterone was elevated at 49 ng/mL (reference range 3.0–35.4), as was plasma renin activity, at 115 ng/mL/hour. His 24-hour urine aldosterone secretion was quite elevated at 61.8 μg/24 hours (2.3–21). Thyroid-stimulating hormone, serum cortisol, and plasma catecholamine levels were normal. His urine normetanephrine level was mildly elevated at 399 μg/g creatinine (91–365), with a normal urine metanephrine level.
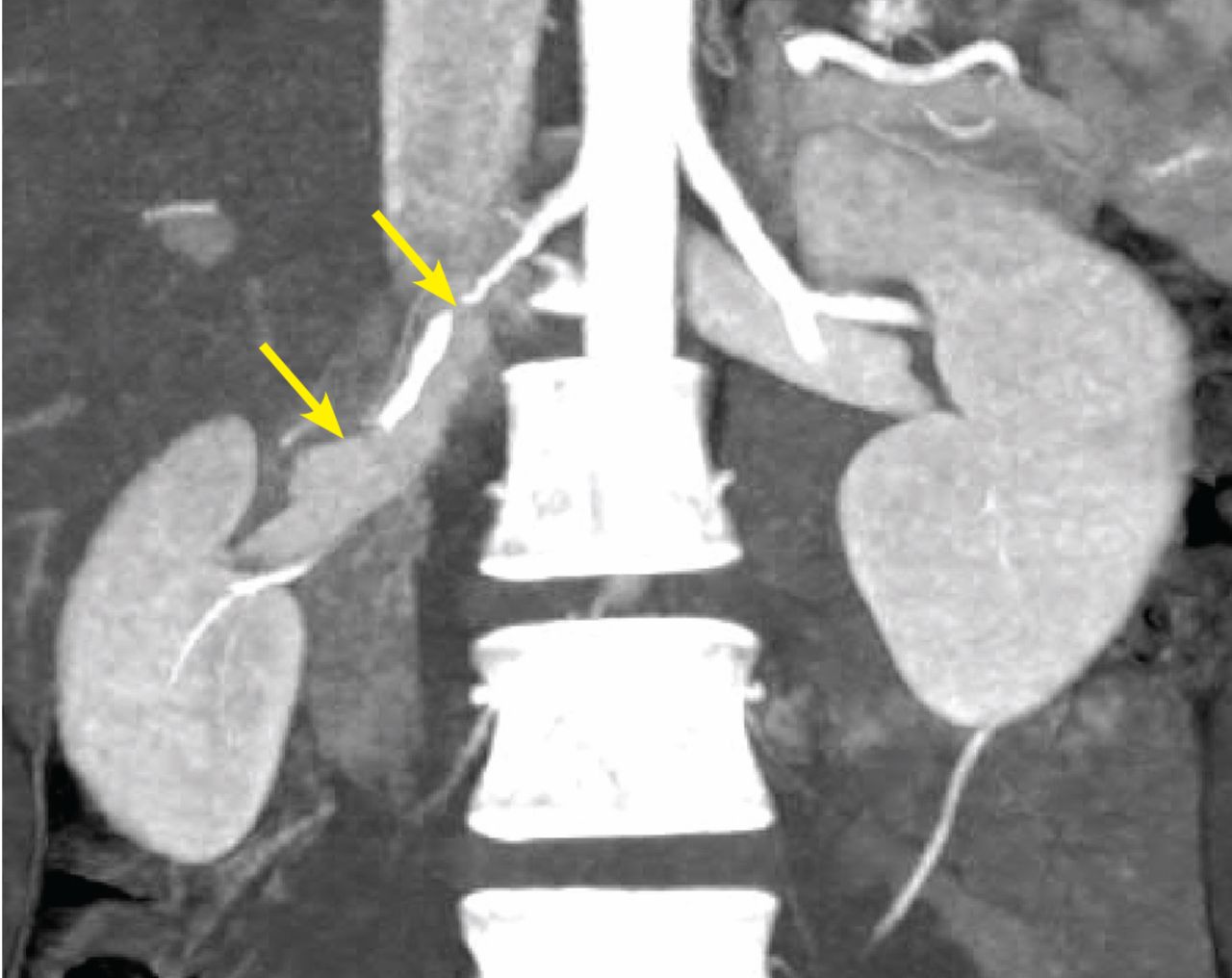
In light of the hypertension with elevated renin activity, hypokalemia, and metabolic alkalosis, the patient underwent computed tomographic angiography of the chest, abdomen, and pelvis with intravenous contrast. Aortic coarctation was ruled out, and the adrenal glands were unremarkable. The right kidney was small, measuring 9.6 cm (vs 11.1 cm for the left kidney), and the right renal artery had multiple midvessel stenoses (Figure 1). Subsequent renal artery duplex ultrasonography revealed a markedly elevated distal peak systolic velocity of 743 cm/second in the right renal artery (normal is < 150).

Coronal computed tomographic angiography demonstrated a small right kidney with multifocal fibromuscular dysplasia of the right renal artery (arrows).
The imaging characteristics were most consistent with multifocal fibromuscular dysplasia leading to secondary hyperreninemia with hyperaldosteronism. The patient underwent percutaneous transluminal angioplasty to 3 critical stenoses of the right renal artery, with less than 30% residual stenosis (Figure 2). Pressure wire measurements of the left renal artery did not demonstrate significant stenosis. Magnetic resonance angiography of the head and neck was normal, with no evidence of fibromuscular dysplasia in the cervical or intracranial circulation.
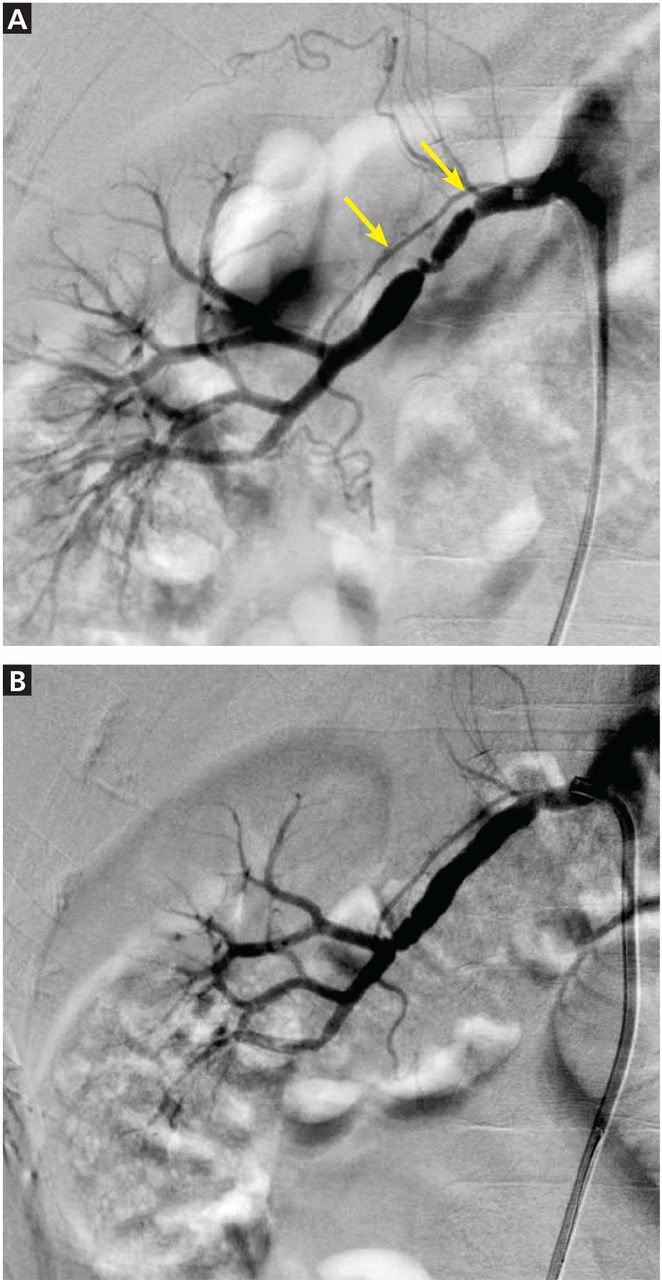
The right renal artery (arrows) before (A) and after (B) percutaneous transluminal angioplasty.
At follow-up 2 years later, his blood pressure was normal without medication; peak systolic velocity of the right renal artery was 203 cm/second.
RENAL ARTERY FIBROMUSCULAR DYSPLASIA
Fibromuscular dysplasia, a noninflammatory vasculopathy of medium-sized arteries, is diagnosed primarily in women (80%–90% of cases), although it can occur in men.1 The renal arteries are most frequently involved, followed by the extracranial internal carotid, vertebral, visceral, and iliac arteries.1 Aneurysm or dissection or both occur in 40% of patients.2 Renal artery fibromuscular dysplasia, when symptomatic, usually manifests with renovascular hypertension, dissection, infarction, and sometimes ischemic renal atrophy.
Diagnosis and treatment
Hypertensive disorders associated with elevated renin activity, hypokalemia, and metabolic alkalosis include renal artery disease and reninoma. Fibromuscular dysplasia is diagnosed radiographically and classified as multifocal (2 or more stenoses) or focal (single focal or tubular stenosis).1,3
Focal and multifocal fibromuscular dysplasia have different epidemiologies and histologies. The focal type is not well correlated with a specific histology, is more common in men, presents at a younger age, and is more often associated with both higher blood pressure and evidence of ischemic nephropathy.3,4 Multifocal fibromuscular dysplasia is classically described as resembling a “string of beads” and correlating with medial fibroplasia on histology. Our patient’s multiple, serial stenoses were clinically more similar to focal than to multifocal disease. Nevertheless, some investigators consider multiple focal, serial stenoses, as seen in this case, to be multifocal fibromuscular dysplasia.
Key to the diagnosis of fibromuscular dysplasia is to exclude vasculitis and other recognized vascular syndromes (eg, Ehlers-Danlos type IV, Loeys-Dietz syndrome) by history, laboratory evaluation, and imaging. Features of such diseases were not present in our patient.
Because disease is found in multiple arterial beds in as many as two-thirds of patients, it is recommended that all patients with fibromuscular dysplasia undergo baseline skull-to-pelvis cross-sectional imaging by computed tomographic angiography or magnetic resonance angiography.1,5
Although percutaneous transluminal angioplasty is not always curative, it is more likely to be successful when performed within 5 years of the onset of hypertension.6 Assessment for restenosis every 6 to 12 months by duplex ultrasonography is common, although velocity data specific to fibromuscular dysplasia are not well established.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.