


ABSTRACT
Community-acquired pneumonia significantly contributes to patient morbidity and healthcare costs. As our understanding of this common infection grows, collaborative efforts among researchers and clinical societies provide new literature and updated guidelines informing its management. This review discusses diagnostic methods, empiric treatment, and infection prevention strategies for patients with suspected community-acquired pneumonia.
Systematically stratifying patients with suspected community-acquired pneumonia based on mortality risk can aid in designating the safest level of care for each patient.
Empiric treatment should be informed by the local antibiogram (ie, local patterns of antibiotic resistance) with multidrug-resistant organism coverage added based on individual patient and institutional risk factors.
Prompt de-escalation to targeted antimicrobial therapy, guided by diagnostic testing, can reduce antibiotic resistance and antibiotic-related adverse drug reactions.
Appropriate clinical and radiographic follow-up after antibiotic course completion to assess for treatment failure is a subject of ongoing debate.
While physicians have treated pneumonia for centuries, each stage of the clinical decision-making process still poses challenges, from determining the most appropriate setting of care for a patient with suspected pneumonia to planning follow-up after antibiotic completion. Over the years, physicians have witnessed the advent of new medical and respiratory therapies as well as the development of antibiotic resistance in the management of this common infection.
Inpatients with pneumonia fall into 2 categories: those with community-acquired pneumonia (CAP) who are admitted, and those who develop either hospital-acquired or ventilator-associated pneumonia while already hospitalized. Each patient population faces unique organism exposures, and thus, recommended diagnostic tests, empiric treatment regimens, and goals for infection prevention vary.
This article reviews guidelines by the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS)1 and interprets recent studies to address questions that arise specifically in the inpatient management of CAP.
COMMON AND COSTLY
CAP is a significant health concern, with one study reporting 915,500 episodes in adults at least 65 years of age in the United States every year, and medical costs associated with CAP exceeding $10 billion in 2011.2,3
The National Center for Health Statistics reported 1.7 million visits to emergency departments in the United States in 2017 in which pneumonia was the primary discharge diagnosis, and listed pneumonia as the cause of death for 49,157 people in 2017.4
RISK-STRATIFICATION OF COMMUNITY-ACQUIRED PNEUMONIA
The IDSA/ATS 2019 guidelines1 emphasize the importance of first determining what level of patient care is needed: Is outpatient treatment appropriate, or does the patient need to be admitted to the hospital, or even to the intensive care unit? Appropriate triage can prevent stresses on the patient and the healthcare system associated with under- or overestimating illness severity. Patients at high risk of death whose acuity is not fully appreciated face inadequate support, while those admitted despite low risk of death may be unnecessarily subjected to the risks of the hospital setting, such as infections from healthcare-associated multidrug-resistant organisms.
Risk calculators are routinely used to help physicians triage their patients in everyday practice, although they have not been specifically validated to predict the need for admission.
CURB-65 is a simple calculator based on 5 risk factors first identified in 1987 (Table 1).1 Patients receive 1 point each for confusion, high blood urea nitrogen, high respiratory rate, low blood pressure, and age 65 or older; the higher the total score, the higher the 30-day mortality risk. According to the IDSA/ATS, patients with scores of 0 or 1 can be managed as outpatients, those with scores of 2 should be admitted to the hospital, and those with scores of 3, 4, or 5 need care in the intensive care unit.
The CURB-65 calculator
An abbreviated version of this calculator, CRB-65, allows risk-stratification of outpatients without laboratory work.1
The Pneumonia Severity Index incorporates 20 risk factors to place patients into 5 classes correlated with mortality risk (Table 2).5 The authors suggest outpatient management for those in classes I or II and inpatient management for those in risk classes IV and V. Patients in class III may be safely treated in an outpatient setting with adequate support or in an inpatient observation unit.
Pneumonia Severity Index calculator and associated risk classes
While CURB-65 may be better in busy clinical settings, as it is a shorter risk stratification scale for CAP, the Pneumonia Severity Index is preferred by the IDSA/ATS 2019 guidelines as it has been more extensively studied and validated.1
The IDSA/ATS guidelines list a separate set of major and minor criteria to define “severe pneumonia” to determine which patients with suspected CAP merit intensive care.1 At least 1 of the major criteria or at least 3 of the minor criteria are required for the diagnosis of severe pneumonia (Table 3).
Severe pneumonia: Infectious Diseases Society of America and American Thoracic Society criteria
The Pneumonia Patient Outcomes Research Team study, a multicenter, prospective controlled study of both ambulatory and hospitalized patients with CAP, also devised a list of risk factors associated with death within 30 days.6 These risk factors include altered mental status, uremia, leukopenia, and hypoxemia. Chronic liver failure was a risk factor highlighted in this study but was not included in the IDSA/ATS criteria.
Yet none of these scoring systems can fully capture all medical or psychosocial comorbidities that may prevent successful recovery in the outpatient setting. A retrospective chart review of more than 1,800 patients found that 45% of patients who had “low-risk” CAP by the Pneumonia Severity Index were nevertheless admitted.7 Patients with cognitive impairment, coronary artery disease, diabetes mellitus, pulmonary disease, multilobular radiographic opacities, home oxygen therapy, corticosteroid use, or use of antibiotics prior to presentation had increased odds of hospitalization.
Clinical judgment should be applied to the results of any of these calculators to appropriately triage patients with pneumonia.
DIAGNOSIS OF COMMUNITY-ACQUIRED PNEUMONIA
Imaging
After triaging a patient with suspected CAP to the safest level of care, several radiographic and laboratory methods can be used to verify the diagnosis and identify the organism most likely responsible for the ongoing infection. Chest radiographs with demonstrable infiltrates are required to diagnose CAP and to distinguish it from upper respiratory tract infection.1
Different organisms can be associated with characteristic infiltrate patterns, which often manifest within 12 hours of symptom onset:
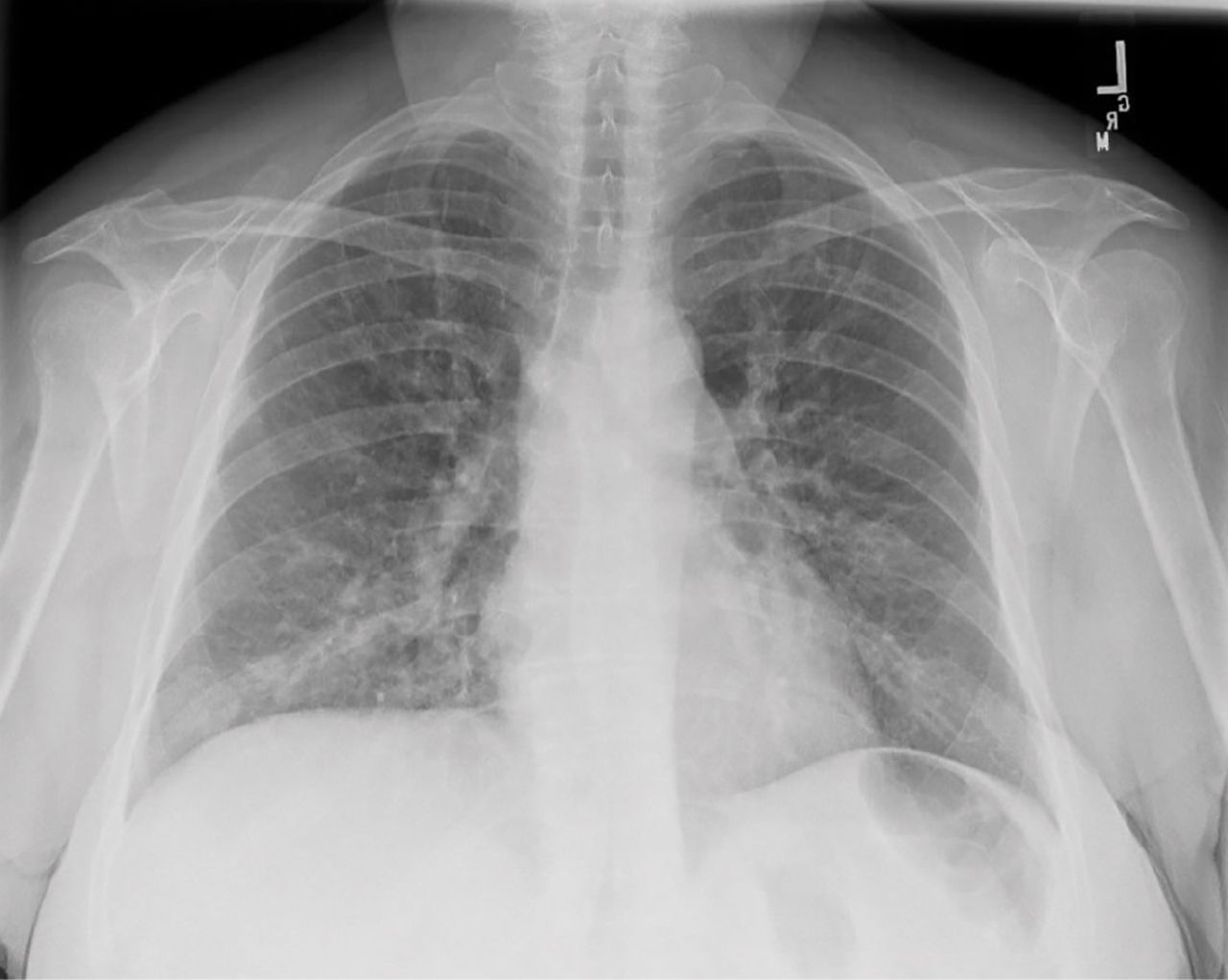
Focal nonsegmental or lobar pneumonia (Figure 1). Typical bacterial pneumonias caused by organisms such as Streptococcus pneumoniae tend to manifest with an airspace opacity in 1 segment or lobe, though antibiotic use can alter their pathophysiology to create a patchy, multilobular opacity pattern.

Focal lobar pneumonia.
Multifocal bronchopneumonia or lobar pneumonia. Bronchopneumonias, similarly characterized by a patchy pattern, are most commonly caused by Staphylococcus aureus, Haemophilus influenzae, and fungi.8
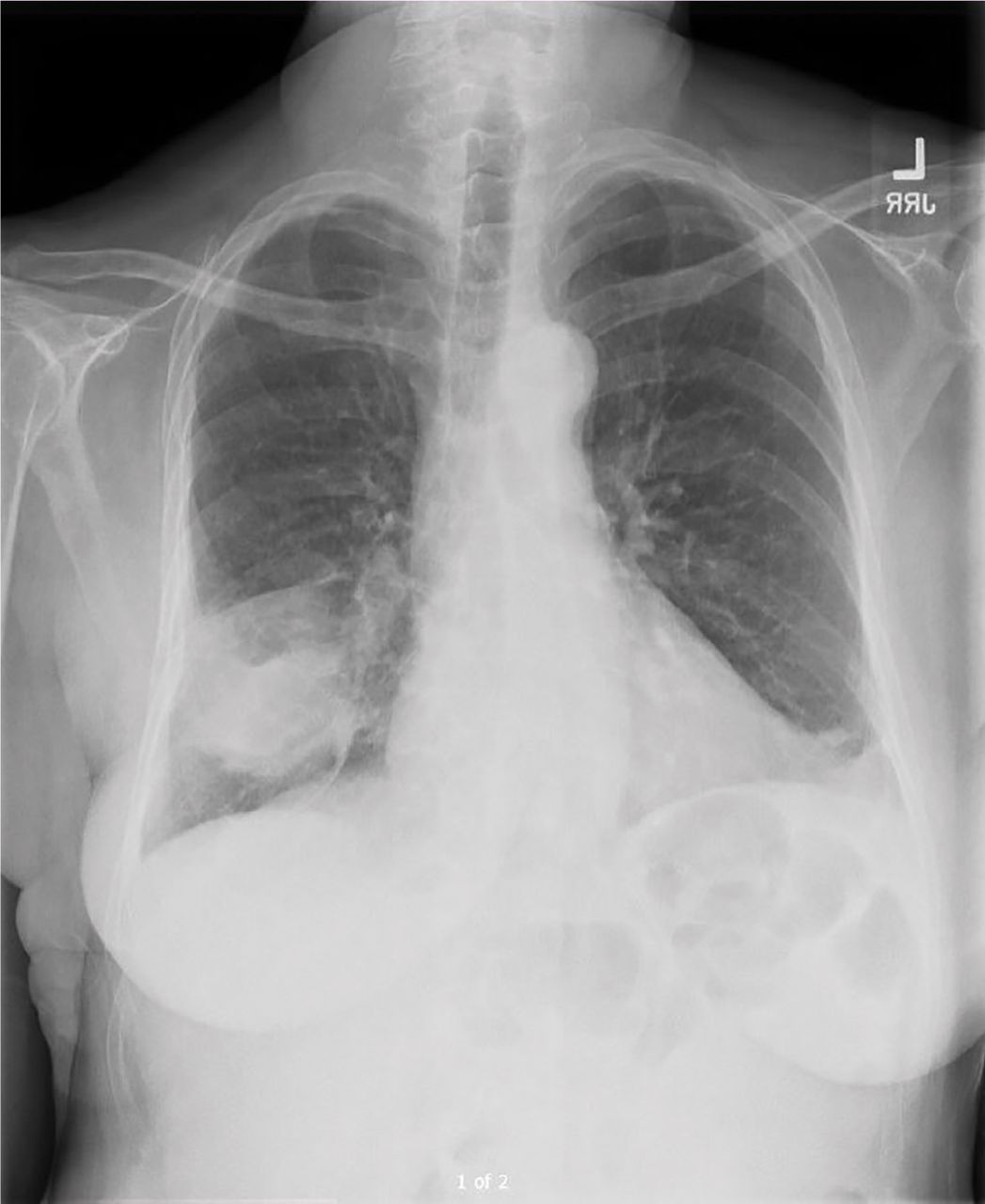
Focal or diffuse “interstitial” pneumonia (Figure 2). Atypical bacterial organisms including Legionella pneumophila, Mycoplasma pneumoniae, and Chlamydophila pneumoniae frequently involve the lung bases in a diffuse, bilateral, reticulonodular pattern, but can start as isolated lobar opacities on chest radiography.9 Viral organisms are associated with diffuse, bilateral lung involvement as well.
Diffuse interstitial pneumonia.
Early radiographic identification of pulmonary complications, such as pleural effusions or cavitating lesions, can provide more clues to the causative organism and allow for timely intervention.9
How accurate is chest radiography?
The utility of chest radiographs in diagnosing CAP is ultimately subject to interobserver variability, with some studies citing 65% ac curacy in diagnosing viral pneumonia, 67% in diagnosing bacterial pneumonia, and no statistical reliability for differentiating bacterial from nonbacterial pneumonias.10 A Swedish retrospective chart review of 103 outpatients with suspected CAP noted that just 88% of patients with high clinical concern for CAP demonstrated radiographic evidence of infection.11
Microbiology
A thorough social history should be gathered for every patient with suspected CAP to screen for potential occupational, travel, or endemic exposures. This will guide microbiologic testing and empiric antibiotic treatment.1 For example, patients presenting during flu season or with known exposures to poultry in areas of prior influenza outbreaks should be screened for influenza A and B with a nasopharyngeal swab.
Isolating a specific organism in outpatients with CAP may not be necessary but is recommended to guide de-escalation of empiric antibiotic regimens.1 Pretreatment Gram stain and culture in patients able to adequately expectorate a good-quality specimen or endotracheal aspirate in intubated patients should be collected. Patients fulfilling criteria for severe pneumonia as defined by the IDSA/ATS guidelines merit blood and sputum cultures as well as urinary antigen tests for L pneumophila and S pneumoniae (Table 4).1
Indications for blood culture testing in suspected community-acquired pneumonia
Overall, active surveillance of more than 2,200 patients with CAP requiring hospitalization noted that 38% of blood and sputum cultures, nasopharyngeal and oropharyngeal swabs, and urinary antigens yielded a causative organism.12 Viral organisms accounted for 25% of these cases and bacterial organisms accounted for 14%; 5% of patients with viral pneumonias were coinfected with either another respiratory virus or a bacterial organism.
Procalcitonin testing
Procalcitonin testing can help differentiate viral from bacterial pathogens in patients admitted for CAP, preventing the use of unnecessary antibiotics and allowing prompt de-escalation of empiric therapy more effectively than clinical judgment alone.13 While any infectious pneumonia can precipitate elevations of this serum biomarker, typical bacteria tend to result in higher procalcitonin levels than atypical bacteria or viruses.14 Cytokines, associated with bacterial infections, enhance procalcitonin release, while interferons, associated with viral infections, inhibit procalcitonin release. This biomarker is not perfect, however, and will not be elevated in up to 23% of typical bacterial infections.14
For this reason, procalcitonin should not replace clinical judgment in guiding the decision to initiate antimicrobial therapy for patients with suspected CAP but can be used in conjunction with clinical judgment to de-escalate therapy. In patients whose clinical histories suggest alternative causes of respiratory distress or improvement with concomitantly administered therapies such as diuresis, a negative procalcitonin can help guide cessation of antibiotics. On the other hand, in patients with polymerase chain reaction-proven influenza, an elevated procalcitonin can suggest continuation of antibiotics to treat bacterial superinfection.
MANAGEMENT OF COMMUNITY-ACQUIRED PNEUMONIA
Antibiotic therapy
The selection of antibiotics before a causative pathogen is identified should be informed by the patient’s risk factors and degree of illness (Table 5, Table 6).1
Common organisms in community-acquired pneumonia
Initial antibiotic therapy for community-acquired pneumonia
Patients on a medical floor should be started on either a respiratory fluoroquinolone or a combination of a beta-lactam plus a macrolide; intensive care patients should receive a beta-lactam plus either a macrolide or a respiratory fluoroquinolone. Doxycycline can be used as an alternative to the macrolide or respiratory fluoroquinolone to cover atypical organisms such as Chlamydia pneumoniae, Legionella pneumophila, and Mycoplasma pneumoniae in patients with prolonged QTc. In penicillin-allergic patients, aztreonam should be used in combination with an aminoglycoside and a respiratory fluoroquinolone.
Patients who may have been exposed to influenza or who have a history of injection drug use or structural lung disease or who have a lung abscess, cavitary infiltrates, or endobronchial obstruction also merit coverage against community-acquired methicillin-resistant S aureus (MRSA) with vancomycin or linezolid. Those with confirmed or suspected influenza A presenting within 48 hours of symptom onset or with severe illness should be treated with oseltamivir.1
If an organism is identified by culture, polymerase chain reaction, or serology, the empiric antibiotic regimen should be tailored to this organism. MRSA nares screening can be reliably used to guide empiric and targeted antimicrobial regimens; patients started on vancomycin or linezolid based on the above-stated risk factors can be safely de-escalated on the basis of a negative nasal swab.15 The pneumococcal urinary antigen has a similarly reliable negative predictive value and can also be used to de-escalate empiric antimicrobial therapy.16
Should microbiologic evaluation fail to identify a causative organism, the patient’s individual risk factors as listed above must be considered in de-escalating therapy to a final regimen with coverage for MRSA, Pseudomonas aeruginosa, or atypical pathogens as indicated. Pseudomonal pneumonia has been associated with higher risk of mortality and relapse than pneumonia caused by other pathogens.
Corticosteroids as adjunctive therapy
The use of adjunctive corticosteroids for CAP management has been widely contested. The IDSA/ATS guidelines recommend against corticosteroid use for adjunctive treatment of CAP except in patients with refractory septic shock.1
Later management
Patients who are hemodynamically stable, can ingest medications safely, and have a normal gastrointestinal tract can be discharged on oral therapy without waiting to observe the clinical response. Antibiotics should be given for at least 5 days, though longer durations may be needed in immunocompromised patients or in those with pulmonary or extra-pulmonary complications.1
An infectious disease consultation may be beneficial if long-term intravenous antibiotic therapy is anticipated or if the patient progressively deteriorates on guideline-based antimicrobial therapy.
Pulmonary consultation may be needed for bronchoscopy to obtain deep respiratory samples, especially if the patient is clinically worsening and the causative pathogen remains unidentified. We acknowledge that the yield of bronchoscopy and bronchoalveolar lavage samples is reduced with longer durations of antibiotic therapy, yet believe that in the context of clinical worsening in spite of antibiotics, bronchoalveolar lavage may help successfully identify multidrug-resistant or atypical pathogens which may not be covered by the ongoing antibiotic regimen. Pulmonology consultation is also indicated for patients with complications of pneumonia such as empyema that require procedural intervention.
TAKE-HOME POINTS
CAP continues to contribute to patient morbidity and mortality as well as healthcare costs.
Professional societies have released collaborative guidelines to streamline practice patterns and provide evidence-based protocols for the diagnosis, treatment, and prevention of this common infection.
Further research is needed to delineate appropriate strategies to de-escalate antibiotics in the absence of a causative organism, define the dose and duration of adjunctive steroid use, and clarify patient follow-up after discharge from the hospital.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}