


ABSTRACT
Liposuction is the second most commonly performed cosmetic surgery in the United States and the most common surgical procedure in patients between the ages of 35 and 64; practitioners of medicine and surgery will undoubtedly encounter these patients in their practice. This brief review discusses the role of liposuction and fat transfer in aesthetic and reconstructive surgery, as well as key considerations, indications, and safety concerns.
The most common area for fat removal is between the inframammary fold and gluteal fold—namely, the abdomen, flanks, trochanteric region, lumbar region, and gluteal region.
Liposuction is increasingly being used as an adjunct to enhance other aesthetic procedures such as breast augmentation, cervicoplasty, abdominoplasty, gluteal fat transfer, and body contouring after bariatric surgery.
Gluteal fat transfer, popularly called the “Brazilian butt lift,” is an application of liposuction in which large volumes of fat are transferred from an undesirable area, such as the abdomen or inner thighs, to the buttocks.
Noncosmetic indications include management of lipomas, lipedema, and lipodystrophy syndromes.
The most common complication is contour deformity.
Suction-assisted lipectomy, more commonly known as liposuction, is an outpatient procedure that removes adipose tissue from the subcutaneous space with the goal of achieving a more desirable body contour. It is the second most commonly performed cosmetic surgery in the United States and the most common surgical procedure in patients between the ages of 35 and 64.1 In 2018, surgeons performed 258,558 liposuction procedures, a 5% increase from 2017.2 The number of liposuction procedures increased 124% from 1997 to 2015.3
Liposuction is advantageous in that the removal of fat cells limits future deposition of fat in those areas.4 Ultimately, liposuction allows plastic surgeons to semipermanently redistribute volume in accordance with a patient’s ideal, and with lower complication, morbidity, and mortality rates than with other surgical procedures.
In addition to its utility for purely aesthetic purposes, liposuction is an important adjunct in reconstructive surgery, particularly of the breast and face, when harvested fat is autologously reinjected in these tissues. One particular procedure rising in popularity and gaining significant attention in the media is gluteal fat grafting.
This article provides a general overview of liposuction, including its history, current techniques, indications, and safety concerns.
HISTORY
The first attempt at fat removal was by Dujarrier in 1921, who operated on the knees and calves of a dancer. Injury to the femoral artery led to amputation of the leg.5 In 1964, Schrudde curetted subcutaneous fat from a patient’s leg, but observed skin necrosis in 4 of 15 separate patients, in addition to hematoma and seroma.6
The era of modern liposuction began in 1975 when Arpad and Fischer pioneered the use of blunt hollow cannulas and suction curettage for liposuction on the outer thighs, but the patients ultimately experienced deforming lymphorrhea.7 An important milestone was reached in 1977 when Illouz developed the “wet technique,” in which injection of hypotonic saline solution and hyaluronidase into adipose tissue before liposuction reduced hemorrhagic risk.8 This type of hydrodissection, similar to that used today, preserved neurovascular bundles and enlarged the deep adipose layer for easier aspiration.
In 1983, Fournier used syringes instead of mechanical suction for better control of negative pressure.9 By 1987, Klein had developed the tumescent technique—a type of local anesthesia infiltration that permitted the removal of larger volumes of fat while reducing bleeding.10 Toledo expanded the use of syringes to include various gauges and sizes for aspiration of adipose tissue in 1988.11
In the early 1990s, the development of ultrasonographically guided liposuction by Zocchi expanded the use of liposuction for previously unfavorable, fibrous areas such as the buttocks.12,13 The development of minimally invasive, laser-assisted liposuction by Apfelberg, also in 1992, prevented destruction of neurovascular structures by cannulas and promoted tissue tightening for an aesthetic result.14 Recently, the development of power-assisted liposuction has further expanded and improved this procedure, increasing the popularity and use of liposuction.15
COSMETIC INDICATIONS
Liposuction is used to achieve body contouring by removing excess fat deposits in undesirable areas of the body. Fat is suctioned from demarcated areas in the body amenable to contouring.
The most common area for fat removal is between the inframammary fold and gluteal fold—namely, the abdomen, flanks, trochanteric region, lumbar region, and gluteal region (Figure 1). Other areas of fat removal include the breasts (eg, breast reduction surgery), thighs, and calves.

Left: Preoperative appearance of a 52-year-old man who presented for liposuction of localized adiposity within the abdomen and bilateral flanks. Right: The same patient 6 months later after removal of 1.4 L of adipose tissue.
The site of incision is an important anatomic consideration, and the surgeon should select regions where the surgical scar, although modest, can be hidden by clothing, as well as locations conducive to broad fanning of the cannula during the procedure.
There are 5 zones in which superficial subcutaneous tissues adhere to underlying deep fascia of muscle: the lateral gluteal depression, gluteal crease, distal posterior thigh, midmedial thigh, and inferolateral iliotibial tract. Because these zones define the natural shape of the body, suctioning from these areas increases the risk of contour deformities.16 Ideally, patients have adequate skin elasticity and are within 20% to 30% of their ideal body weight to achieve desired aesthetic outcomes.17
Liposuction is also increasingly being used as an adjunct to enhance other aesthetic procedures such as breast augmentation, cervicoplasty, abdominoplasty, gluteal fat transfer, and body contouring for postsurgical bariatric patients (Figure 2 and Figure 3).18 Liposuction can also be used to promote gender-specific features.19 In women, the goals of liposuction are to promote shapely contours of the breasts, waist, hip, and buttocks. In men, liposuction aims to achieve upper body dominance, such as removing excess flank adipose tissue (“love handles”).

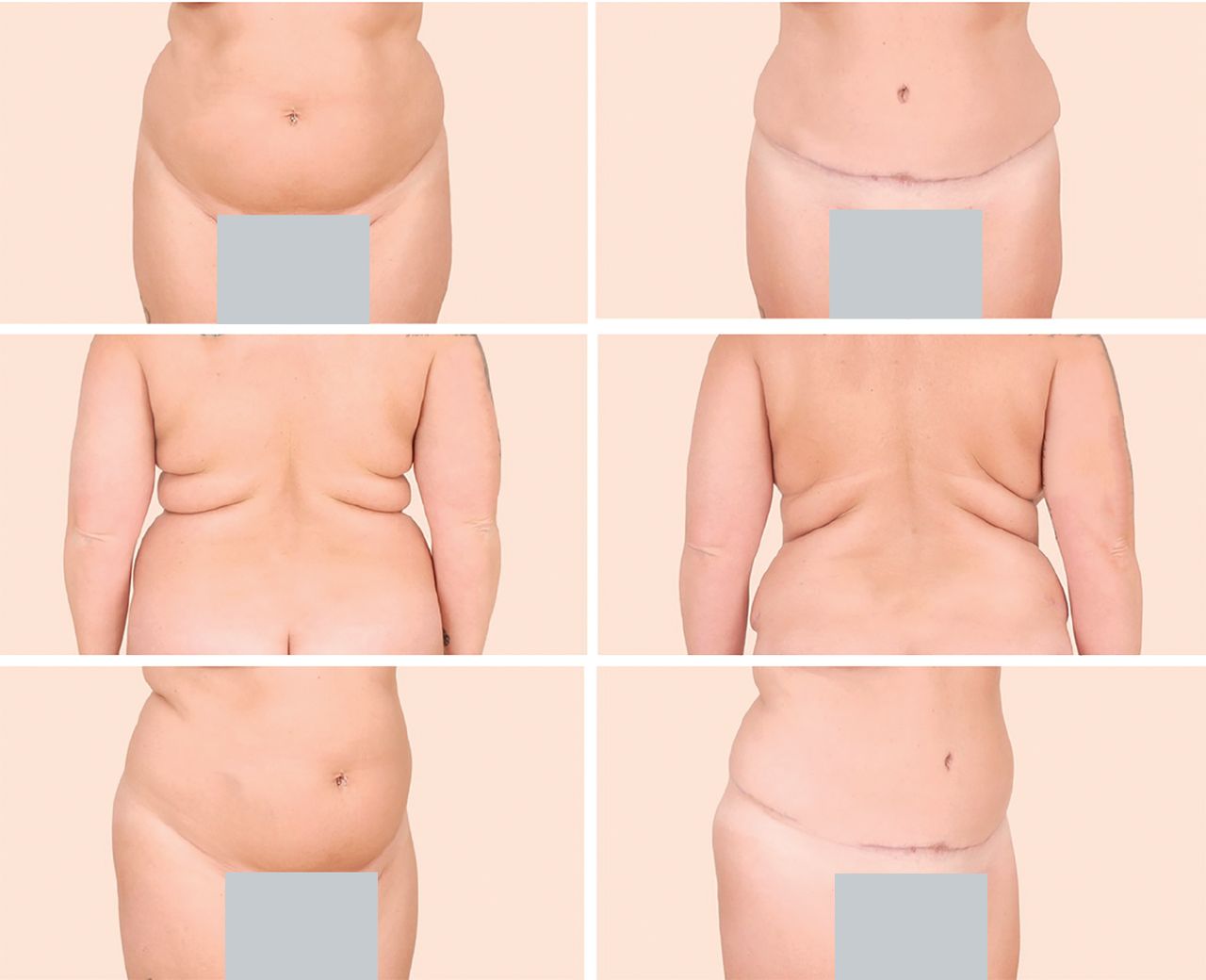
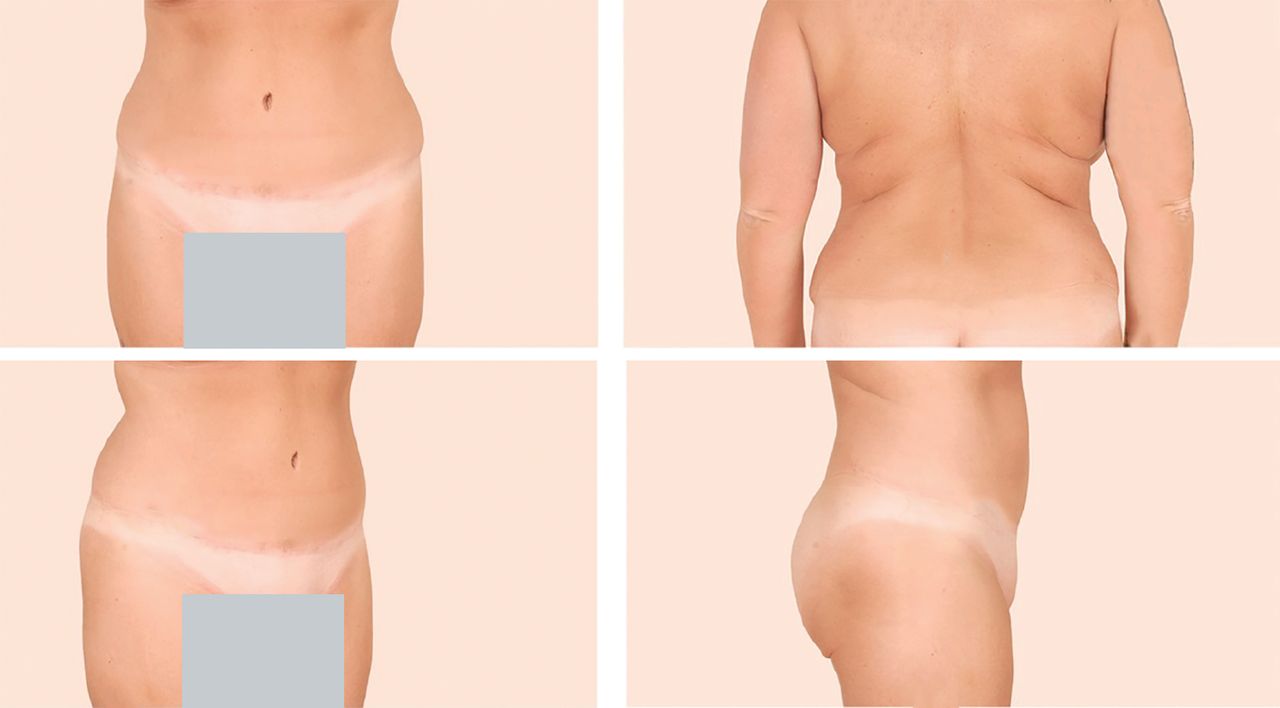
Left: A 38-year-old woman who presented with excess skin and adiposity of the anterior abdomen and excess adipose tissue in the bilateral upper back and hips. Right: The same patient 5 months later after full cosmetic abdominoplasty and liposuction of the bilateral upper back and hip areas (with a total of 2 L of tissue removed), illustrating that these procedures may be combined safely and yield satisfying results.

The same patient from Figure 2, now almost 19 months after surgery but having lost weight, demonstrating stable long-term results after abdominoplasty and liposuction. Note the stable improvement in bilateral flank and upper-back adiposity.
GLUTEAL FAT TRANSFER
Gluteal fat transfer, popularly called the “Brazilian butt lift,” is an application of liposuction in which large volumes of fat are transferred from an undesirable area, such as the abdomen or inner thighs, to the buttocks.20 Fat is first removed by liposuction (the volume of which varies widely and remains largely based upon the patient’s preoperative anatomy) and is then used to augment the contour of the buttocks commensurate with the patient’s desires and anatomic deficiencies.21,22
High-volume fat transfer, defined as a volume greater than 1,000 mL per buttock, has historically been associated with a higher risk of infection at the graft site and seroma formation at the harvested site. Newer evidence suggests high-volume buttock fat transfer may be safe and effective with proper technique.23 Thus, the contour is improved in both the donor region, such as the waist, and the recipient region.
The popularity of gluteal fat transfer is rapidly increasing due to shifting beauty standards in American culture and attention from celebrity figures. More than 26,000 gluteal fat transfer procedures were performed in 2018, a 16% increase from the previous year, and a 132% increase from 2013.3,24 However, reports of fatal pulmonary fat embolisms following injury to gluteal veins and an estimated mortality rate of 1 in 3,000 from this procedure warrant continued investigation about its safety and ideal technique.25
The Multi-Society Gluteal Fat Grafting Task Force26 was established to investigate and improve patient safety of this procedure, and current research including anatomic studies as well as educational symposia are ongoing. Risks and alternative methods such as gluteal implants must be discussed with the patient before this procedure. Moreover, as with any aesthetic or reconstructive procedure, the American Society of Plastic Surgeons recommends that patients seek consultation from a board-certified plastic surgeon.
NONCOSMETIC INDICATIONS
Liposuction is also being used for reconstructive purposes, including management of the following disorders:
Lipomas and angiolipomas, with minimal to no scarring
Lipedema, in which subcutaneous fat deposition in the lower limbs can interfere with daily activities such as walking; in these patients, liposuction can improve mobility27
Lymphedema, particularly if it is refractory to traditional conservative treatments
Lipodystrophy syndromes, which are congenital or acquired diseases of fat atrophy; liposuction with autologous fat transfer can replace loss of fat in areas such as the feet or buttocks to relieve physical discomfort28
Cervicodorsal lipodystrophy associated with Cushing syndrome and use of HIV medications29
Gynecomastia in men and macromastia in women, in conjunction with mammoplasty. Additionally, liposuction can be used to:
Reduce excess fat deposits at surgical sites in obese patients who are undergoing tracheostomy, colostomy, or urostomy procedures • Reduce the amount of subcutaneous fat in flaps created for reconstructive procedures, thereby improving aesthetic results
Collect harvested fat to “lipofill” in breast reconstruction, burns, and scars because adult adipose-derived stem cells are contained therein.30
Although no absolute contraindications exist for liposuction, relative contraindications should be considered during the patient evaluation.31 Anticoagulants and medications that interfere with lidocaine metabolism should be stopped before liposuction.32 Poor skin firmness and elasticity in elderly patients would lead to poor skin draping postoperatively and potentially increase patient dissatisfaction.
Further, reasonable expectations must be established, and patients with body dysmorphic disorder may require a psychiatric consultation before surgery. Patients with diabetes mellitus, cardiac disease, and liver disease may need medical clearance before surgery at the discretion of both the surgeon and the facility where the procedure is to take place. Lastly, as has been discussed elsewhere in the surgical literature, poorly controlled diabetes increases the risk of infection.
TECHNIQUES
The most common technique remains the traditional suction-assisted lipectomy (Table 1).33–36 Small-volume liposuction procedures in which a maximum of 1,000 mL of fat is removed can be performed with local anesthesia. Although there is no maximum volume of fat that can be removed in a single setting, the risk for seroma and fluid imbalance increases along with the volume of fat that is removed.
Liposuction techniques
Megaliposuction, a procedure in which an amount greater than 10% of body weight is removed, can be safely performed by an experienced surgeon. Large-volume liposuction procedures should be performed with general anesthesia.19 Harvested fat may be used for subsequent fat transfer.19
The advantages of liposuction are short surgery time (typically under 3 hours, depending on the extent of fat removal) and concomitant procedures. In addition, patients undergoing liposuction have a short recovery period, unobtrusive scars, permanent results, low complication rates, and low morbidity and mortality rates relative to other surgical procedures. Because adipocytes are removed, further storage of fat in those areas is limited, leading to high patient satisfaction with long-term results.37
More research is needed to determine the degree of fat reaccumulation in the treated area and redistribution to nontreated areas.38,39 As expected, weight gain can still occur, and the patient should be advised to maintain a well-balanced diet and exercise regimen.
RISK FACTORS
Patients with cardiovascular disease, pulmonary disease, diabetes, and vascular disease face a greater risk with this procedure. Tobacco use is a risk factor for surgical complications.40,41 Ongoing infections before the procedure, particularly near the area of the liposuction site (eg, cellulitis), would require treatment with antibiotics and resolution of infection before surgery. Previous venous thromboembolism, eg, pulmonary embolism, may also increase the risk of surgical complications.
COMPLICATIONS
Complications are relatively uncommon in liposuction and of low risk relative to other procedures.42 In one study, the overall complication rate was 2.4%.43 The complication rate was higher (3.5%) when liposuction was combined with other procedures, whereas liposuction as a solitary procedure had a complication rate of only 0.7%.41 Complications include ecchymosis, edema, surgical site infection, seroma, hematoma, and venous thromboembolism (Table 2).43
Complications of liposuction
The most common complication of liposuction is contour deformity. As many as 9% of patients may report soft-tissue depressions or elevations, skin panniculus, folds, or wrinkles.44 Contour deformities can be prevented by using smaller diameter cannulas, avoiding suctioning from superficial layers, employing a “crisscrossing” technique, and allowing slight undercorrection for postoperative fat lysis.45
Seroma and hematoma are also rare complications of liposuction.46 Seromas, which are collections of serous fluid resulting from breakdown of the fibrous tissue network, may develop from initial blind cannula injury to small perforating vessels or lymphatic vessels.31 Use of progressive tension sutures—primarily a technique to address dead space in surgeries such as abdominoplasty (“tummy-tuck”)—has been shown to reduce the rate of seroma from 9% to 2%.46
Wound infection is reported in fewer than 3% of inpatient liposuction cases and in approximately 1% in outpatient surgeries.47 Low infection rates can be attributed to surgeon expertise, proper prophylactic antibiotics, and sterile technique, among other factors. Although uncommon, early-stage wound infections (ie, cellulitis) may develop into more severe sepsis or necrotizing fasciitis—the latter of which is a surgical emergency.48
A 2018 study estimated that after liposuction with or without subsequent fat grafting, at least 17 patients have experienced clinically significant fat embolization, or fat embolization syndrome.49 However, more recent data suggests that worldwide, fatal and nonfatal fat embolism, particularly after gluteal fat grafting, may exceed 135 cases.50
Although fat embolism is rare, its mortality rate of 10% to 15% warrants careful postoperative monitoring for rapid detection and treatment, and it has been reported to occur within 12 to 72 hours after surgery. 50,51 As described, gluteal fat transfer is the only procedure with a higher risk of fatal fat embolism, and is still considered to have the highest mortality rate of any aesthetic procedure.52
The incidence of venous thromboembolic events (deep venous thrombosis and pulmonary embolism) after liposuction is low at 0.03%.53,54 Pulmonary embolism is the most common cause of death after this procedure, which carries an overall mortality rate of 0.01%.54 Same-day ambulation after liposuction surgery is encouraged to prevent thromboembolic events.
As with any surgical procedure, liposuction causes a transient elevation of acute inflammatory markers (interleukin 6, C-reactive protein), but there is no increased risk of progression to renal disease or chronic inflammation.55 Some studies suggest that, due to permanent removal of adipocytes, the long-term metabolic benefits of liposuction include improved insulin sensitivity and reduced inflammation. However, more studies are warranted.56
Systemic complications that arise weeks to months after surgery include edema, lymphedema, wound dehiscence, hypertrophic scar formation, ecchymosis, and skin laxity. Blind cannula injury can lead to abdominal wall injury, bowel perforation, or vessel injury. Although uncommon, skin devascularization and skin necrosis can occur if the surgeon suctions too closely to the skin undersurface and injures the dermal plexus.57
Breast augmentation with autologous fat transfer may lead to fat necrosis that mimics microcalcifications suspicious for breast cancer on mammographic imaging.58 However, the incidence of these imaging findings is similar to those in patients without fat transfer, and thus, breast augmentation does not hinder detection of breast cancer.
FUTURE DIRECTIONS
Liposuction can improve body contour and reduce body mass index, and advances are continually being developed. Due to the benefits of long-term weight redistribution, low surgical risk, and short operation time, patients seeking body contour changes will continue to pursue liposuction. The long-term effects on metabolic sequelae such as insulin sensitivity are still being actively researched.59,60
Noncosmetic indications are also expanding, particularly fat grafting for breast, facial, and pedal reconstruction.61 Although liposuction can address a wide variety of needs spanning from cosmetic to reconstructive purposes, the procedure is rarely covered by Medicare or third-party insurance plans, even for issues that cause functional impairment.62
Research is being performed in noninvasive body contouring such as cryolipolysis, which may decrease subcutaneous fat deposits while providing dermal tightening with no surgical scars.63,64 Cryolipolysis (CoolSculpting), deoxycholic acid subcutaneous injection (Kybella), and radiofrequency skin-tightening (Thermage) are nonsurgical volume-reduction and tissue-tightening procedures that address dissatisfaction with body contouring but remain beyond the scope of this manuscript. We mention them for the sake of completeness.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.