


A 53-year-old woman came to us because of shortness of breath. The problem had started about 3 years earlier, had slowly gotten worse, and was now limiting her activities of daily living. It was associated with wheezing, and her primary care physician had diagnosed it as asthma. Since that time, she had been hospitalized at least twice with “asthma exacerbations,” which were treated with systemic corticosteroids and intravenous antibiotics.
See related editorial, page 150
She had then been referred to a pulmonary physician for spirometry, which showed severe obstruction that did not reverse with bronchodilators. Her condition was diagnosed as chronic obstructive pulmonary disease (COPD) and was treated with montelukast and the combination of inhaled budesonine and formoterol at home.
These drugs did not relieve the symptoms, and she continued to have shortness of breath and wheezing, mainly on exertion. Her BODE index, which is used to predict mortality in COPD, was 5. BODE is an acronym that stands for body mass index, airflow obstruction [forced expiratory volume in 1 second (FEV1)], dyspnea, and exercise [6-minute walk distance]. The minimum score is 0 and the maximum score is 10. Lower scores are better than higher: a score of 5 indicates more than a 50% chance of death in 4 years.
The patient never smoked or used illicit drugs. She worked as a teacher most of her life and reported no environmental exposure to fumes or dust. She had never undergone endotracheal intubation. She was referred to our clinic for evaluation for a lung transplant.
PHYSICAL EXAMINATION AND WORKUP
The patient weighed 52 kg and her height was 155 cm. Her blood pressure was 132/84 mm Hg, heart rate 82 beats per minute, and respiratory rate 18 breaths per minute. General inspiratory and expiratory stridor sounds were detected in both lung fields and in the anterior neck area. The rest of the systemic examination was unremarkable.
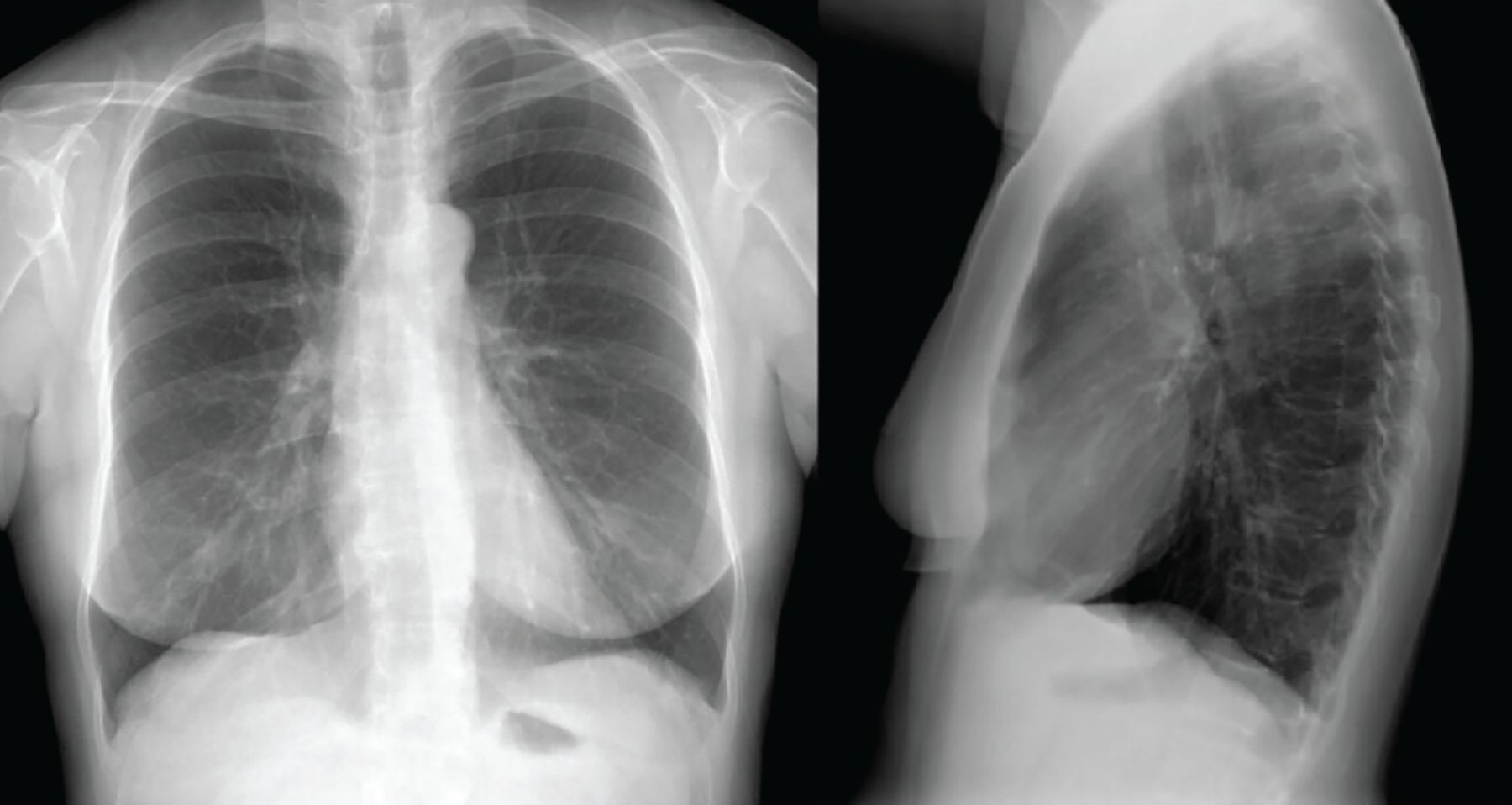
Chest radiography (Figure 1) and computed tomography of the chest were normal.

Chest radiography, posteroanterior and lateral views, showed normal findings.
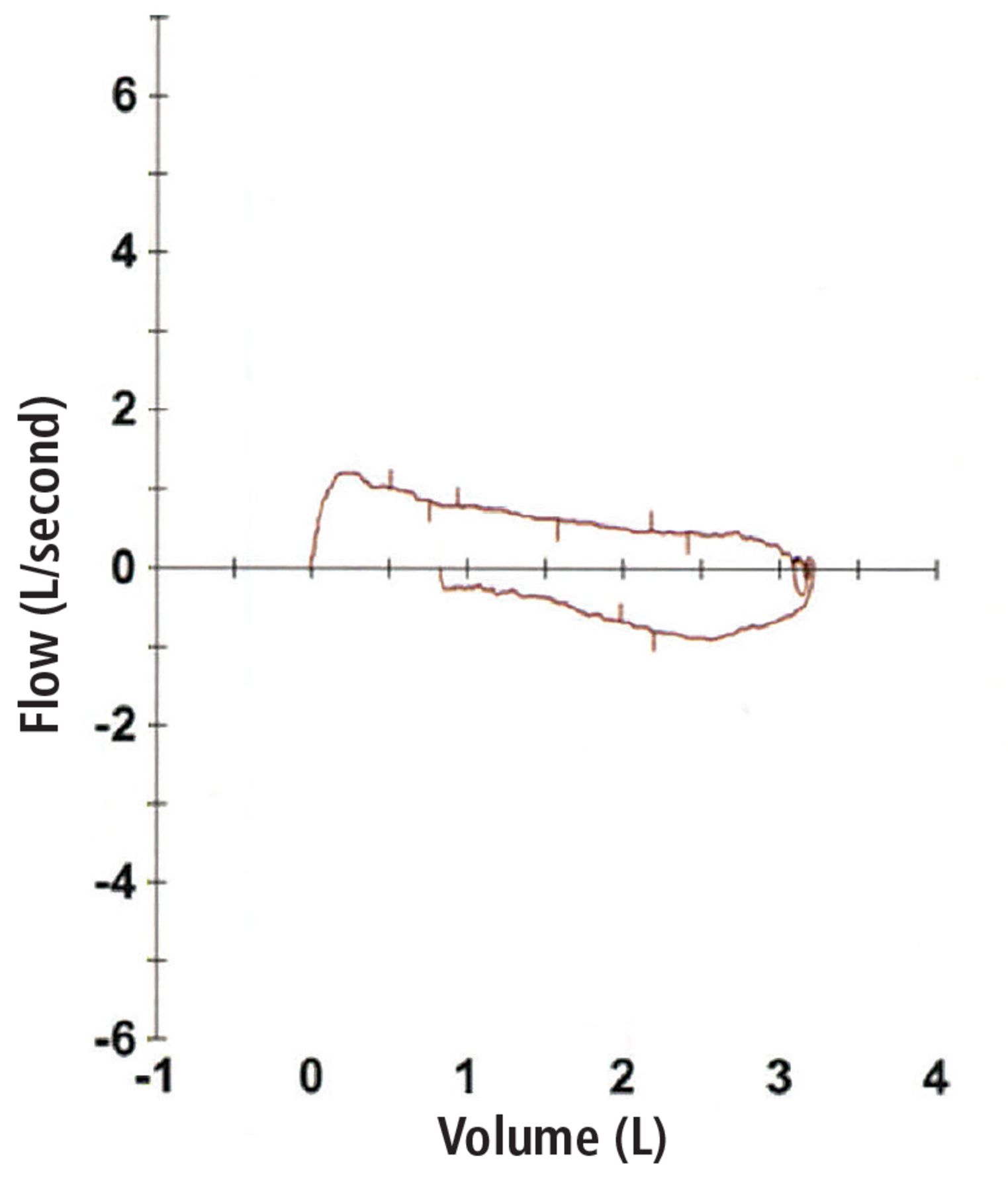
Spirometry showed severe obstructive pulmonary disease, and her forced vital capacity and FEV1 did not change when she was given a bronchodilator. Lung volume showed no evidence of air trapping or hyperinflation (Table 1). A flow-volume loop showed obstruction during inspiration and exhalation, suggesting a fixed extrathoracic airway obstruction (Figure 2).
Results of spirometry
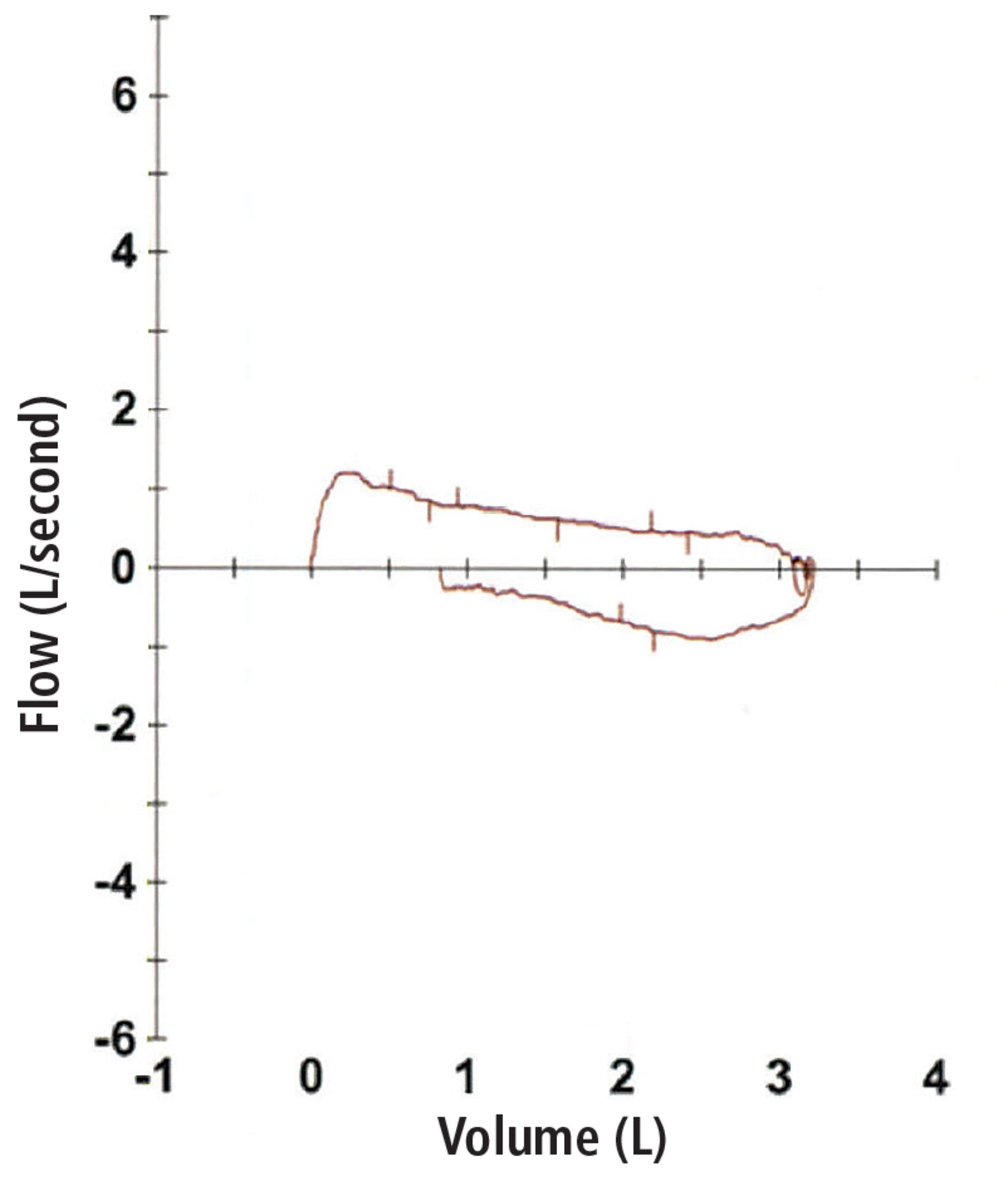
Flow-volume loop showed a decrease in inspiratory and expiratory flow suggestive of fixed extrathoracic airway obstruction.
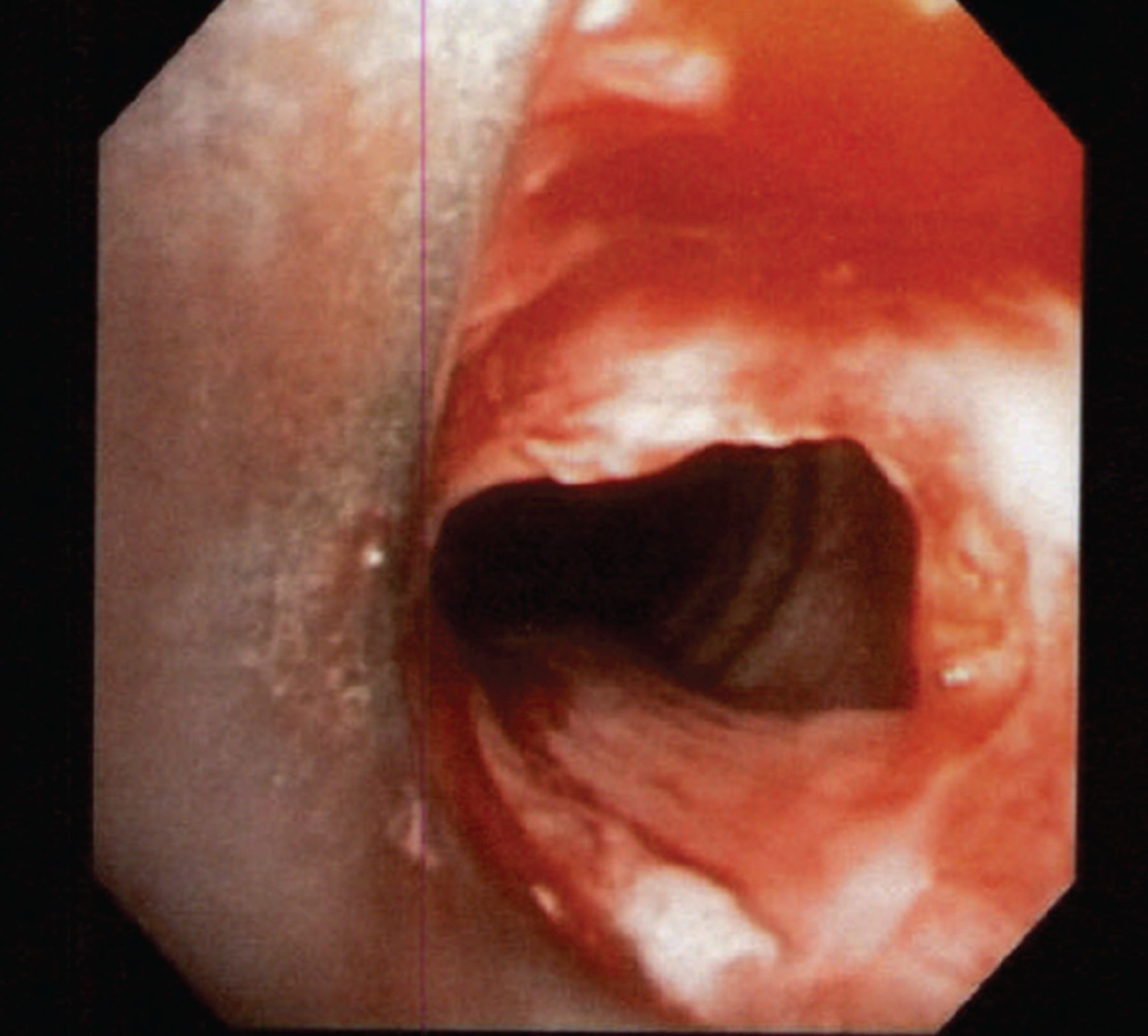
Flexible fiberoptic bronchoscopy was performed to evaluate the upper airway. The larynx was normal in shape, without laryngomalacia, and the vocal cords had synchronized movement with no abnormalities detected. However, an incomplete ring of tissue (web) was found about 1 cm below the vocal cords (Figure 3).
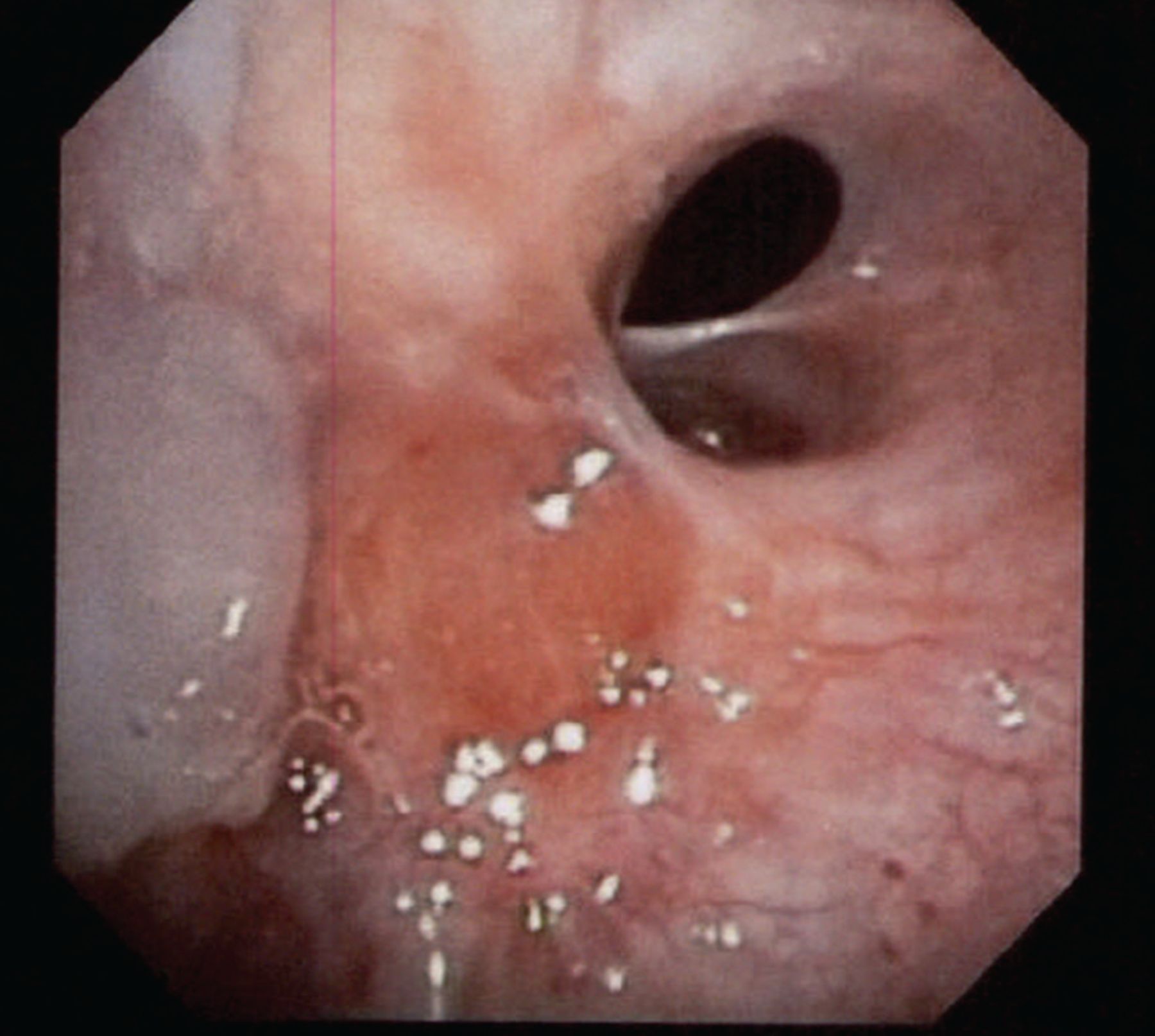
Tracheal web was seen below the vocal cords on flexible bronchoscopy.
The patient underwent resection of the tracheal web with endobronchial argon plasma coagulation. Afterward, bronchoscopy showed appropriate dilation of the tracheal stenosis (Figure 4), and her symptoms significantly improved. She was followed in the pulmonary clinic for 1 year, during which her symptoms completely resolved, and repeat pulmonary function testing showed normal findings.

Resection of tracheal web performed with successful endobronchial argon plasma coagulation dilation.
DISCUSSION
Tracheal web is a tissue layer covering the tracheal lumen. The web is usually incomplete and is not associated with a tracheal cartilage abnormality or deformity.
Congenital tracheal web is a rare anomaly. In children, the incidence has been estimated at 1 in 10,000 births.1 In adults, a few cases have been found incidentally during planned endotracheal intubation.1–5 In addition, tracheal stenosis can be a late complication of endotracheal intubation or tracheostomy in adults, and so can tracheal web, although it is rare.6,7
Tracheal web is usually misdiagnosed as asthma or COPD.2,6,8 In our patient, the correct diagnosis was missed by multiple physicians over many years, leading to inappropriate referral for lung transplant.
Bronchoscopy combined with computed tomography reconstruction is a reliable and sensitive method of evaluating tracheal web in suspected cases.6,9 It is also important to examine the flow-volume loop obtained during spirometry. Sometimes a rare diagnosis like tracheal web can be easily identified, and appropriate management can be rendered.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2021 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}
{kind=link}
{kind=link}