


A 45-year-old man presented to the emergency department with severe dyspnea and cough that had gradually worsened over the past 3 months. His medical history was notable for stage IIA esophageal squamous cell carcinoma that had been treated with esophagectomy 15 years ago; and 13 years ago, he had developed mediastinal lymph node metastasis and had received chemoradiotherapy. He had been a heavy smoker and drinker but had quit 15 years ago.
Emergency contrast-enhanced thoracic computed tomography (CT) revealed a tumor mass in the lower trachea, sclerotic enhancement of the T1 vertebral body (Figure 1) and from the C2 to T2 vertebral bodies, and thrombosis in the left brachiocephalic vein (Figure 2). The patient rapidly developed type 2 respiratory failure (defined as a Pao2 < 8.0 kPa and a Paco2 > 6.0 kPa) and underwent bedside fiberoptic bronchoscopy, which revealed an obstructive tumor in the lower trachea that had invaded the carina and both the left and right main bronchi. Bronchoscopy-guided radiofrequency ablation was performed to relieve airway obstruction. Moderately differentiated squamous cell carcinoma was confirmed by endobronchial biopsy study.
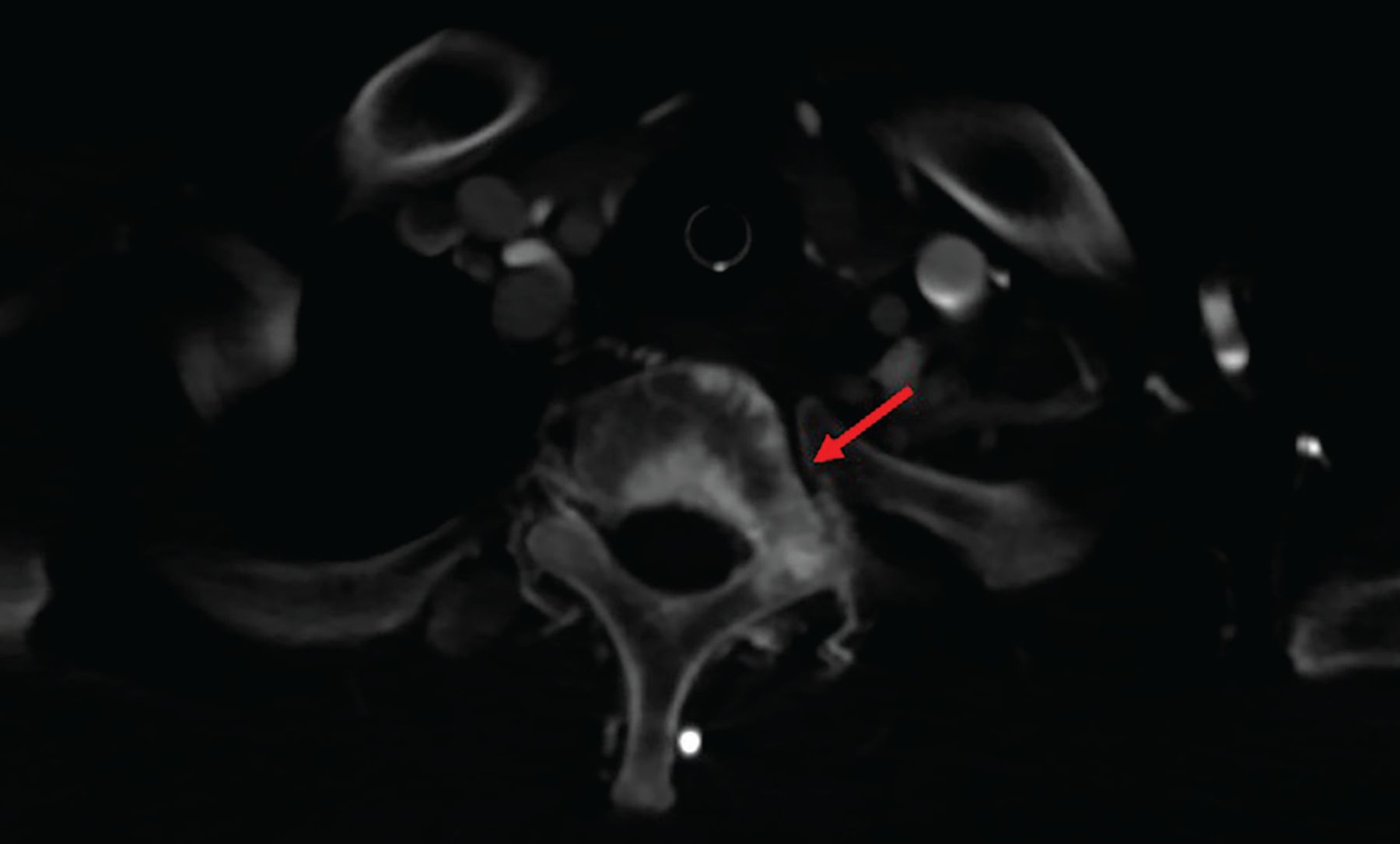
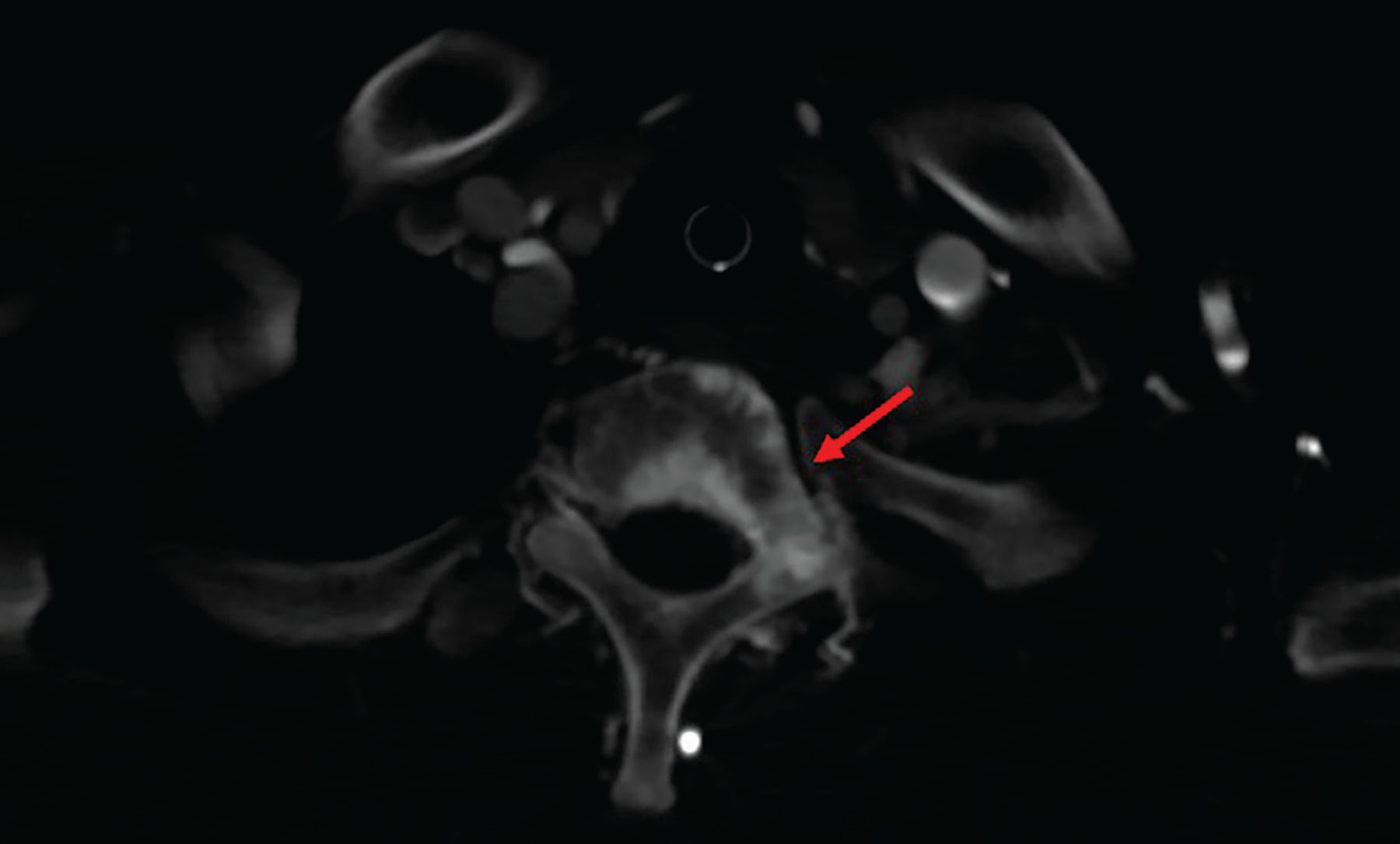
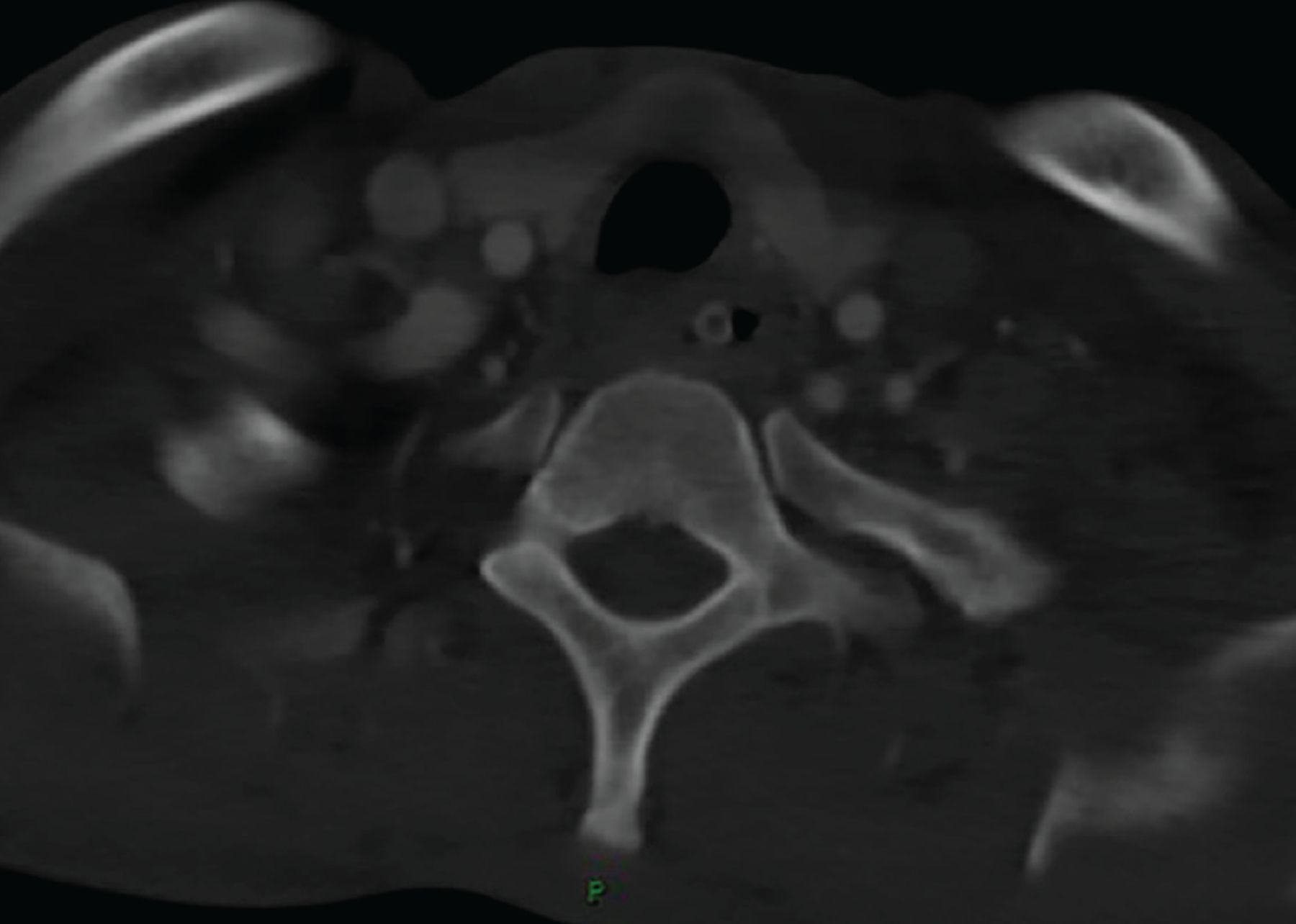
Contrast-enhanced thoracic computed tomography showed sclerotic enhancement of the T1 vertebral body (red arrow).
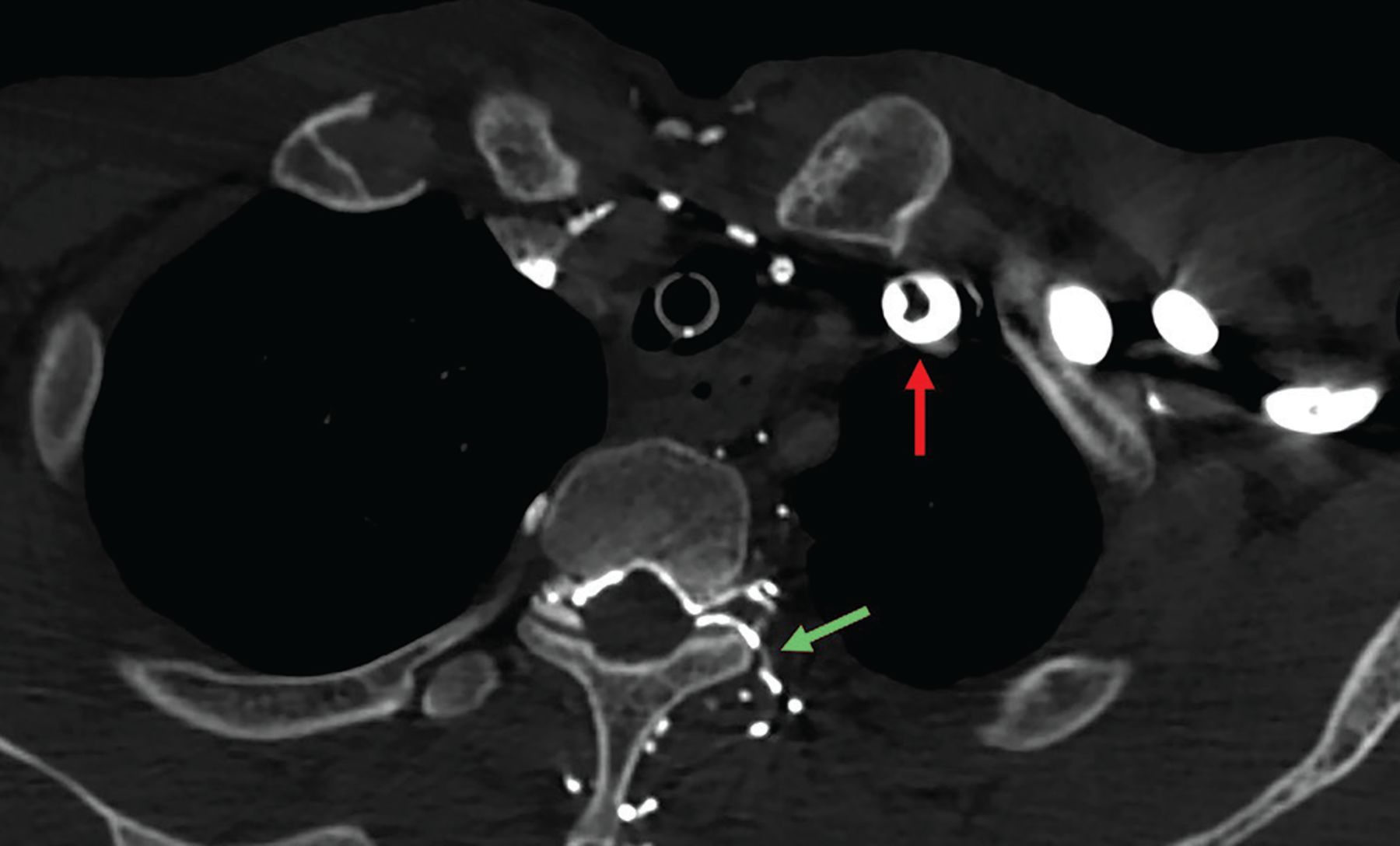
Contrast-enhanced computed tomography noted thrombosis in the left brachiocephalic vein (red arrow) and contrast filling of the paravertebral veins, usually occult on contrast enhancement (green arrow).
The patient’s dyspnea improved after bronchoscopic therapy. Repeat CT 5 days later showed no evidence of the vertebral body enhancement (Figure 3). Esophagoscopy showed an anastomotic stenosis 24 cm from the incisors and smooth mucosa in the esophagus. Anastomotic stenosis was consistent with the tumor location in the lower trachea and carina. Esophageal stenosis and smooth esophageal mucosa demonstrated external tumor compression of the esophagus, which did not support the diagnosis of esophageal carcinoma.
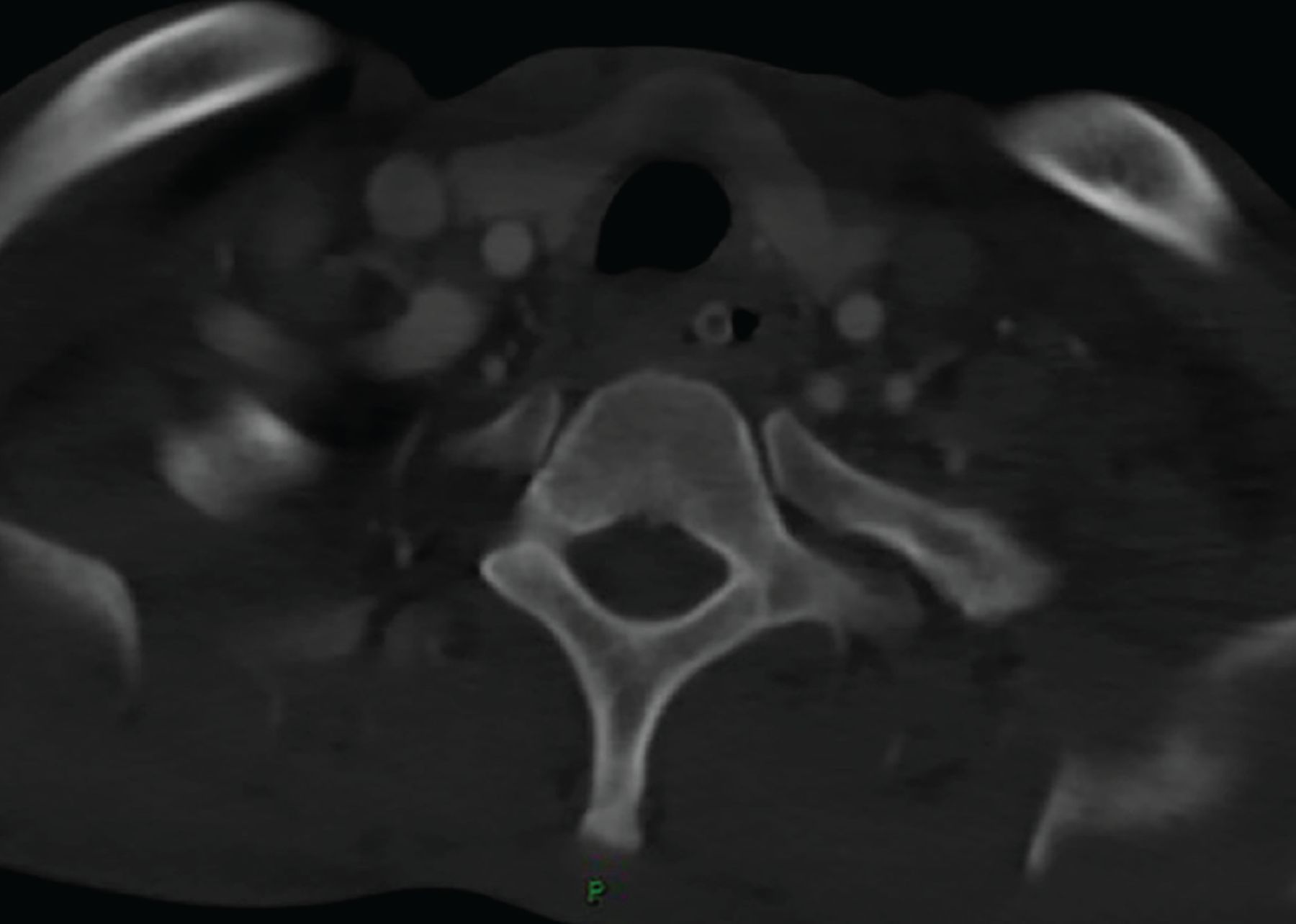
Repeat computed tomography showed the disappearance of the sclerotic vertebral body enhancement.
Based on the patient’s smoking and irradiation history and the long interval between the last anticancer treatment and the appearance of the second tumor, the obstructive tumor was diagnosed as a second primary bronchogenic carcinoma.
The patient underwent disease staging with positron emission tomography CT, which showed increased 18F-fluorodeoxyglucose uptake at the back wall of the trachea alone, indicating that the tumor was localized.
TREATMENT
The patient received 4 cycles of capecitabine and anlotinib, followed by 4 cycles of anlotinib. This achieved a partial response. At last follow-up, the patient was alive and without disease progression.
PSEUDOPATHOLOGIC VERTEBRAL BODY ENHANCEMENT
The differential diagnosis of sclerotic lesions on contrast-enhanced CT includes tumor metastasis, mastocytosis, sarcoidosis, osteomyelitis, lymphoma, Paget disease, and pseudopathologic vertebral body enhancement. For patients with a history of cancer, the leading cause is metastatic malignancy.
A limited number of case reports showed that pseudo pathologic vertebral body enhancement may exist in the presence of obstruction of the superior vena cava or brachiocephalic vein. This is uncommon and easily misdiagnosed as sclerotic osseous metastasis in clinical practice.1,2
The mechanism of pseudopathologic sclerotic enhancement of vertebral bodies is not well characterized. However, an elevated venous pressure that induced contrast agent reflux into the intravertebral venous plexus was proposed as a main reason.3
In our patient, narrowing of the left brachiocephalic vein proximal to the superior vena cava resulted in elevated venous pressure and blood flow into the vertebral venous plexus, causing reflux of contrast agent.1,4 Sclerotic enhancement of the vertebral bodies and vertebral venous collaterals, which are usually occult on CT, were seen. Eight consecutive vertebral bodies were involved, which is uncommon with metastasis. However, when the contrast agent was injected into the contralateral arm during the second CT, the vertebra enhancement disappeared (Figure 3).
Pseudopathologic vertebral body enhancement due to brachiocephalic vein narrowing is rare. However, sclerotic bone metastasis based on contrast-enhanced CT should prompt a careful evaluation when narrowing or obstruction of the brachiocephalic vein and paravertebral collateral veins is present on imaging. Spine magnetic resonance imaging or positron emission tomography CT should be performed to confirm the diagnosis.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2021 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.