


Article Figures & Data
Figures
- Figure 1
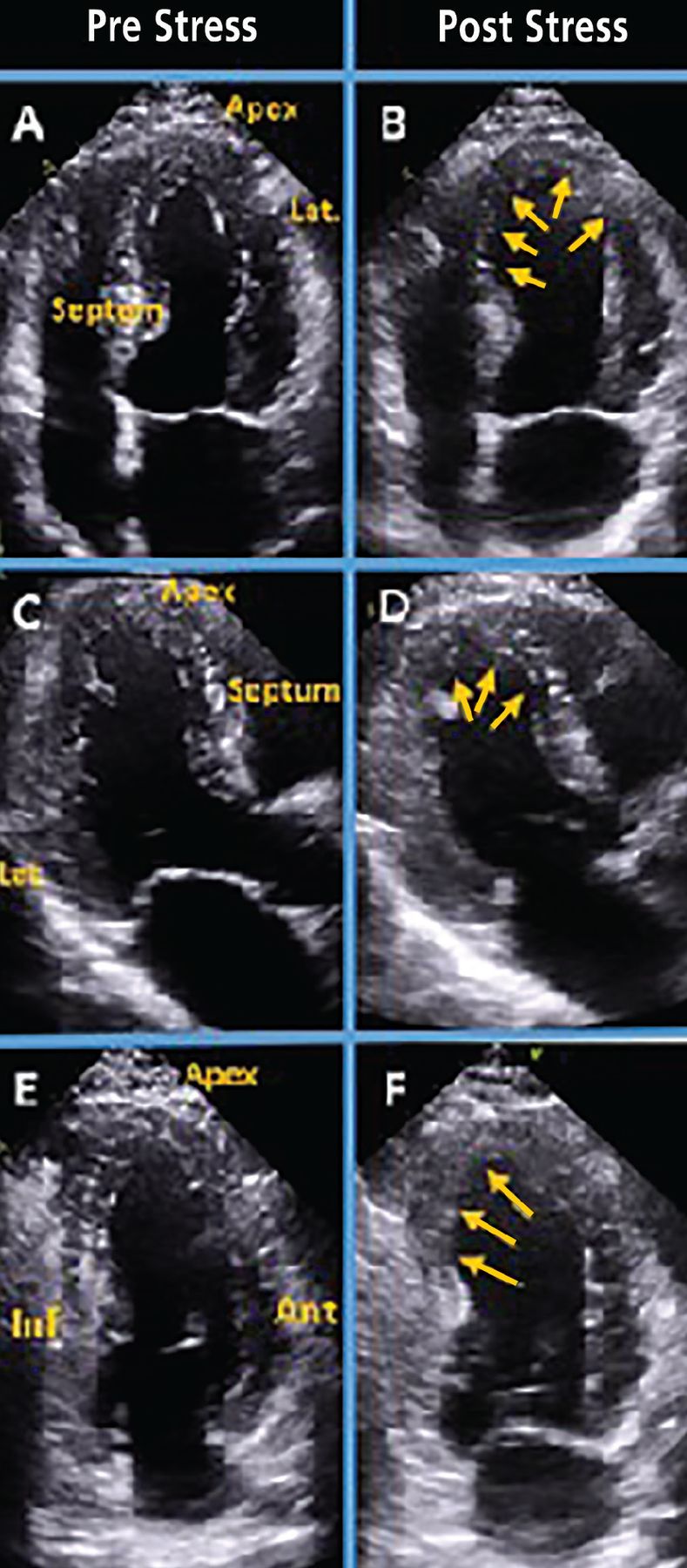
Stress echocardiogram from a 54-year-old woman with chest pain shows ischemia in the left anterior descending artery and right coronary artery territories. Panels A and B show the 4-chamber view before and after the stress test. On the poststress image (B), the arrows point to hypokinesis at the apex and distal septum; enlargement of left ventricular cavity suggests significant ischemia. In the long-axis view (C, D), arrows point to hypo-kinesis at the apex and distal septum. In the 2-chamber view (E, F), arrows point to hypokinesis on the mid and apical inferior wall.
- Figure 2
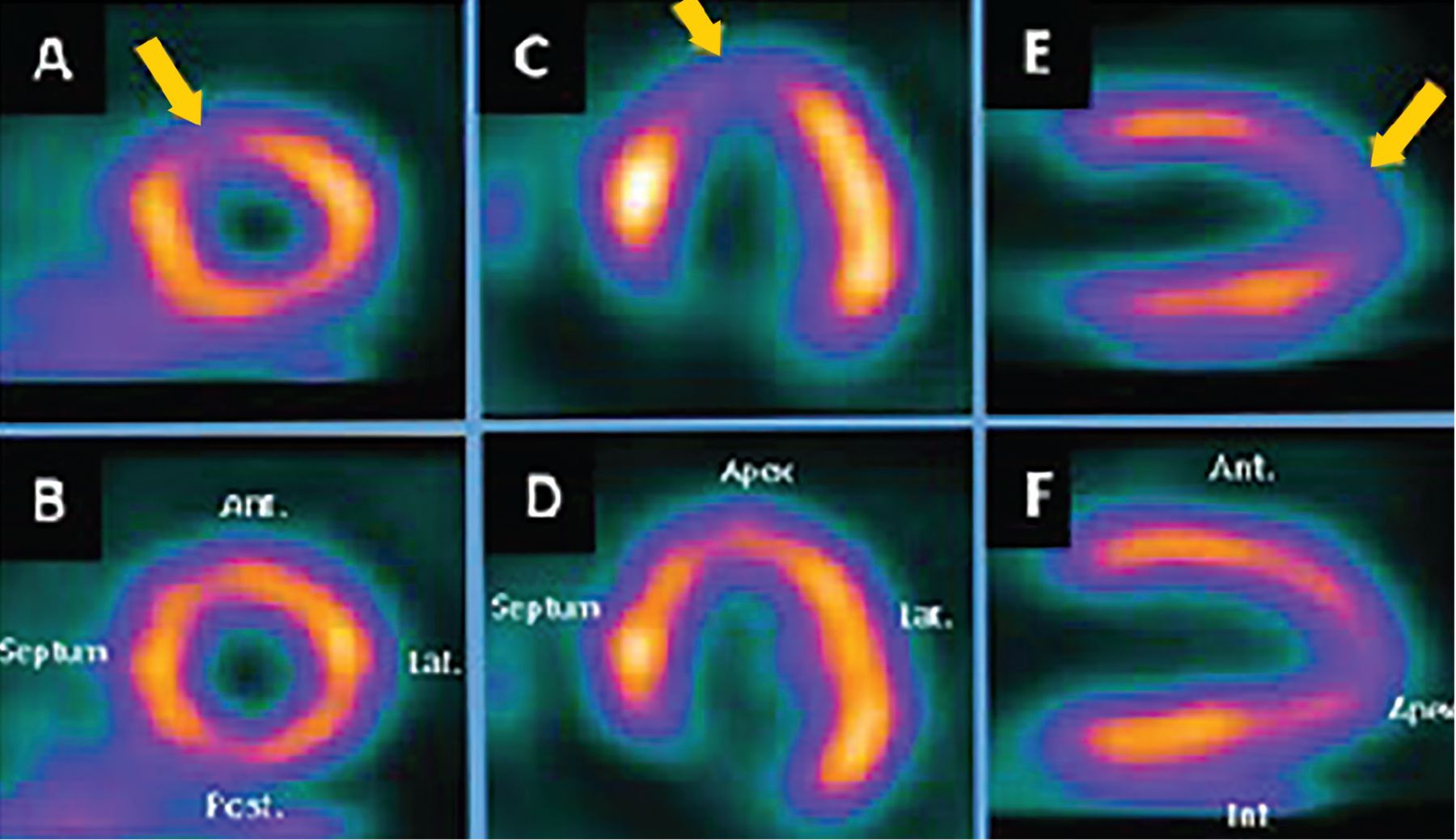
Single-photon emission CT myocardial perfusion imaging in a 62-year-old man with diabetes and a 2-month history of dyspnea shows moderate left anterior descending coronary artery ischemia. Panels A, C, and E are poststress images that show perfusion defects in the apex, apical septum, and apical anterior wall (arrows). Panels B, D, and F show relatively normal perfusion at rest at the corresponding levels.
- Figure 3
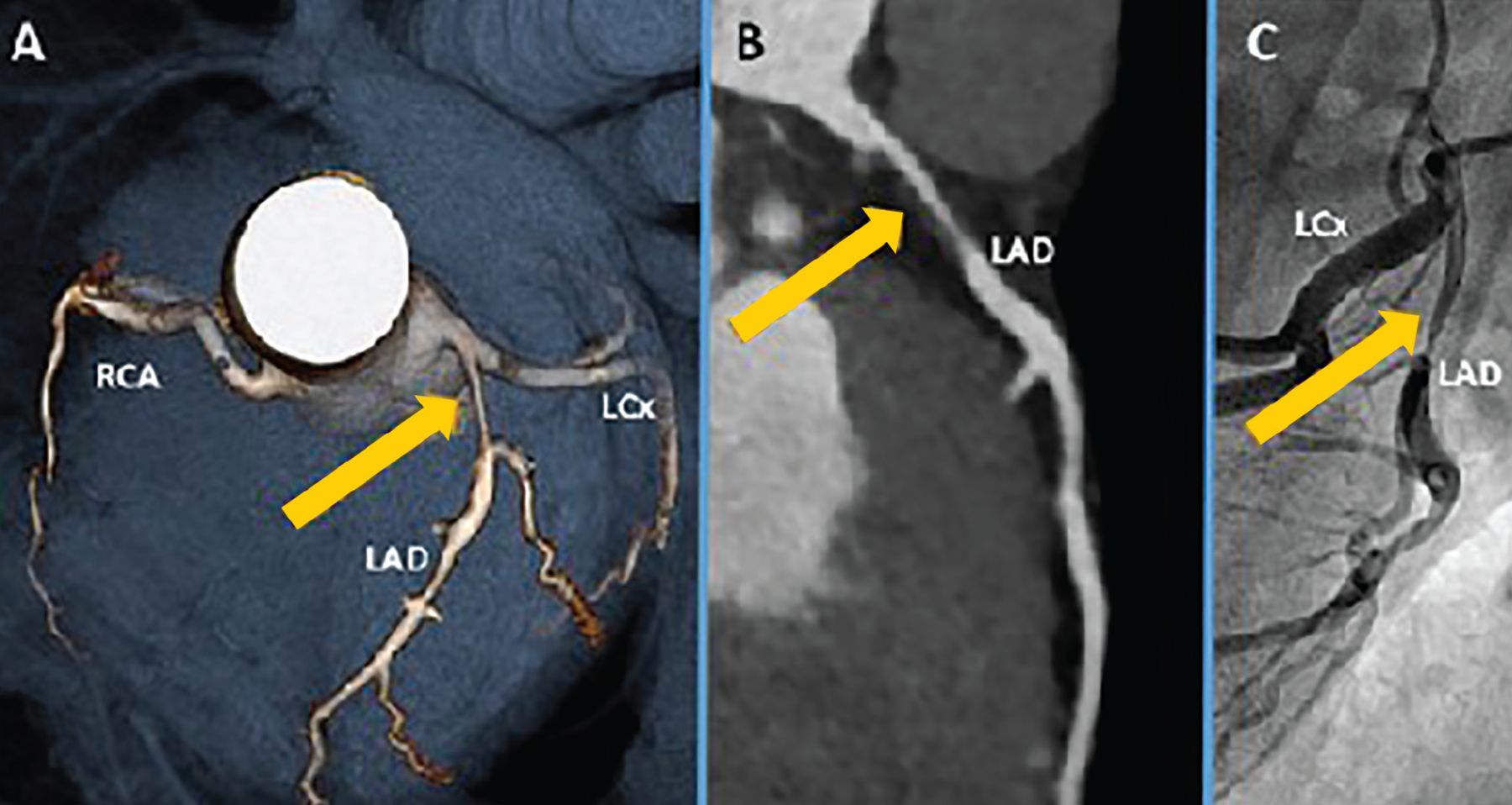
Coronary computed tomography angiography in a 40-year-old man who smoked and had a family history of premature coronary artery disease. Panel A is a 3-D rendering showing proximal left anterior descending (LAD) coronary artery stenosis (arrow). Panel B is a multiplanar reconstruction showing proximal LAD coronary artery stenosis with predominantly soft (lipid-laden) noncalcified plaque (arrow). Panel C shows the corresponding LAD lesion (arrow) on coronary catheterization.
LCx = left circumflex artery; RCA = right coronary artery
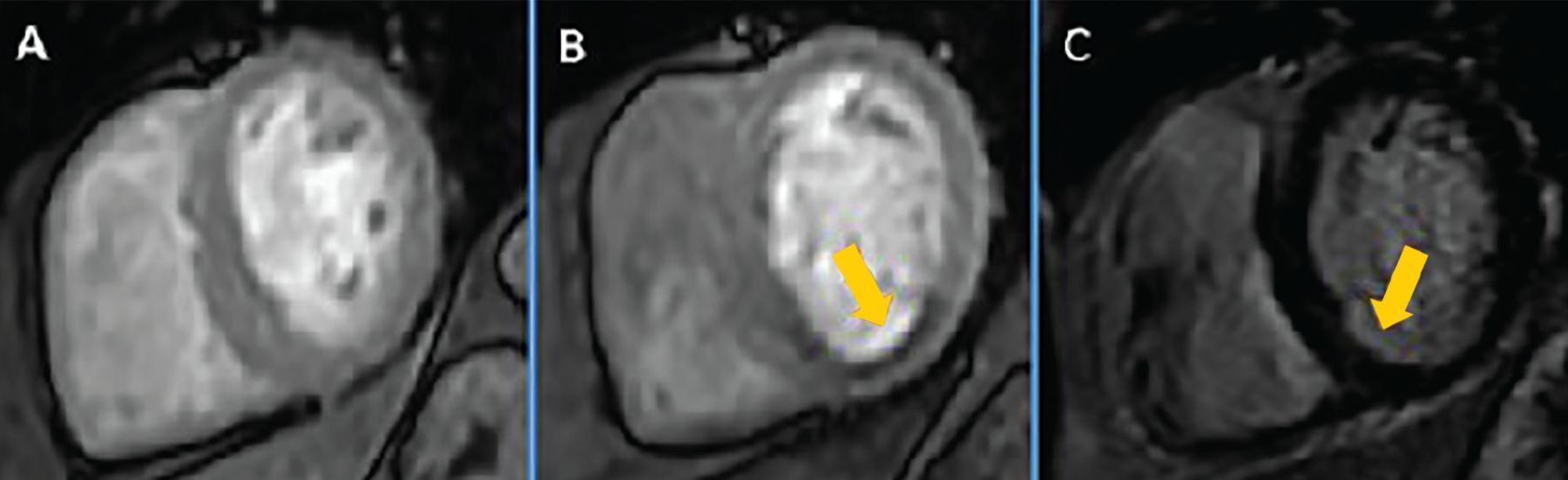
- Figure 4
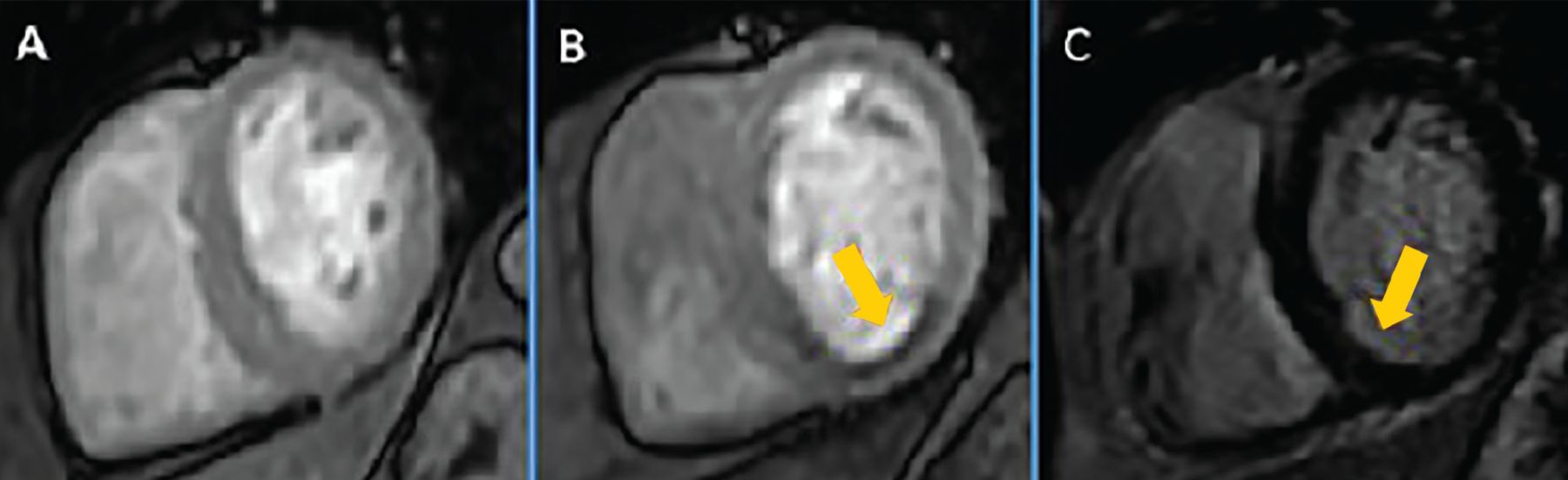
Stress cardiac magnetic resonance imaging in a 67-year-old woman with diabetes and chest pain shows normal perfusion at rest (A). Panel B shows a poststress image with a perfusion defect in the inferior and inferoseptal segments (arrow), suggestive of ischemia in the right coronary artery territory. Panel C is a delayed gadolinium-enhanced image showing mild subendocardial enhancement (arrow) in the corresponding region, consistent with a small area of scar.



Tables
Functional Electrocardiography exercise stress test
Stress echocardiography
Nuclear medicine myocardial perfusion imaging techniques
Single-photon emission computed tomography
Positron emission tomography
Cardiac magnetic resonance imaging with stress perfusionAnatomic Coronary computed tomography angiography
Invasive coronary catheterization- TABLE 2
Common indications for stress testing and coronary computed tomography angiography
Assessment for coronary artery disease
Angina or anginal equivalent symptoms and negative cardiac enzymes
Atypical symptoms in patients with diabetes or with high probability of diabetes
New diagnosis of cardiomyopathy (to define whether the cause is ischemic or nonischemic)
New or increasing heart failure symptoms despite adherence to medical therapy
Re-evaluation of known heart failure (systolic or diastolic) in patients with a change in clinical status without a clear precipitating change in medication or diet
Arrhythmias such as ventricular tachycardia or atrial fibrillation (to exclude ischemia as the cause) or new left bundle-branch block
To exclude severe ischemia prior to noncardiac surgery in those with increased coronary artery disease risks, angina symptoms, or poor exercise capacity (< 4 metabolic equivalents)
To define presence or absence of ischemia in those with moderate coronary stenosis (stress test or fractional flow reserve-computed tomography)
Evaluation of anomalous coronary arteriesStress testing for indications other than coronary artery disease assessment
Valve assessment
Mitral valve stenosis or regurgitation severity (exercise stress echocardiography)
Low-flow low gradient aortic stenosis (dobutamine stress echocardiography)
Exercise-induced pulmonary hypertension or diastolic dysfunction (exercise stress echocardiography)
Hypertrophic cardiomyopathy to demonstrate provocable left ventricular outflow tract obstruction (exercise stress echocardiography)
Exercise-induced arrhythmia or chronotropic incompetence (exercise stress echocardiography)
To define cardiopulmonary disease and aerobic exercise capacity (metabolic stress test)Data from references 3 and 7–10.
Indicator Comments Functional capacity Strongest prognostic indicator, reported as metabolic equivalents.7,14 ST-segment depression or elevation > 1-mm ST deviation is suggestive of ischemia.13 Exercise-induced hypotension Defined as systolic blood pressure that is lower during exercise than while standing at rest before exercise, reflecting failure of cardiac output to increase during exercise.
Associated with severe coronary artery disease or left ventricular systolic dysfunction.15Chronotropic incompetence Failure of heart rate to increase as expected during exercise, defined as achieving < 80% of predicted heart rate (or < 62% for patients taking beta-blockers).16
Associated with increased all-cause and cardiovascular mortality.17Impaired heart rate recovery Heart rate fails to decrease normally after cessation of exercise.
Predicts all-cause mortality and cardiovascular events, including sudden death.18Ventricular arrhythmia Sustained ventricular tachychardia or ventricular fibrillation.
Associated with significant coronary artery disease or left ventricular dysfunction.19
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.