


A 22-year-old woman was brought to the emergency department after her parents had noted she had been behaving more and more strangely for the past 2 to 3 weeks, being irritable and secluding herself in her room. They had called emergency medical services after noticing that 4 amitriptyline tablets were missing from her father’s prescription bottle and after hearing her make nonsensical statements. The patient had recently lost a close friend to drug overdose, and her parents had attributed her behavior changes to this stressor.
The patient had also been complaining of gradual-onset and progressive headache and neck and back pain for 3 weeks. She described it as a constant, aching sensation of moderate intensity that over the past week had begun to wake her from sleep. She denied any sensory or motor disturbances, changes in vision, fever, trauma, or sick contacts. She had been taking acetaminophen, naproxen, and tizanidine.
INITIAL EXAMINATION
Her blood pressure was 111/55 mm Hg, pulse rate 55 beats per minute, temperature 97.4°F (36.3°C), respiratory rate 16 breaths per minute, and oxygen saturation 100% by pulse oximetry on room air. She was alert but uncooperative and answered questions inappropriately.
Her ears, eyes, nose, and throat were unremarkable. Breath sounds were clear throughout both lungs. Her heart rate and rhythm were normal with no murmurs, rubs, or gallops. Her abdomen was soft and non-tender. Her cranial nerve examination was normal. She had normal strength (5 on a scale of 5) and intact sensation in all extremities. Her neck had full range of motion, but she said it hurt, worst during flexion.
Results of a comprehensive metabolic panel including liver function tests, complete blood cell count with differential, ethanol level, acetaminophen level, urine beta-human chorionic gonadotropin, urinalysis, and urine toxicology were normal, but her urine was positive for tetrahydrocannabinol.
Magnetic resonance imaging (MRI) of the head with and without contrast was obtained and revealed a 1.2-cm nonhemorrhagic ring-enhancing lesion within the insular pole of the left frontal lobe with adjacent subcortical vasogenic edema, without restricted diffusion (Figure 1).

Tumor or abscess? T1-weighted magnetic resonance imaging with contrast, obtained soon after presentation, showed a 1.2-cm ring-enhancing lesion (arrow). Diffusion-weighted imaging did not show restricted diffusion.
RING-ENHANCING BRAIN LESIONS
1. Which of the following brain tumors typically presents with ring-enhancing lesions on MRI and therefore would be the most likely in our patient, if she has a brain tumor?
Low-grade glioma
Meningioma
Germ cell tumors
Glioblastoma
Ring-enhancing lesions have a broad differential diagnosis that includes malignancy, demyelinating lesions, infection, and subacute infarction. Certain characteristics can help distinguish the likely etiology of central nervous system lesions. For example, pyogenic brain abscesses typically present with restricted diffusion while malignant lesions typically do not.1
Among the choices given, this patient’s MRI characteristics would be most consistent with glioblastoma. Glioblastoma typically presents with ring enhancement due to central necrosis, without restricted diffusion.2 However, glioblastoma also usually has thick, irregular borders, which our patient’s MRI did not show.
CASE CONTINUED: WORKUP FOR FEVER AND INFECTIOUS DISEASES
The neurosurgery department was consulted for a possible brain tumor. However, on her fourth day in the hospital, the patient became febrile for the first time during the hospitalization, and her temperature was 102.6°F (39.2°C).
We elicited further history from her parents. She had no fever or febrile symptoms before admission. She had grown up in the Ohio River valley and lived with her father, who was divorced from her mother. She had no pets at home and no recent infections or dental manipulations. She drank socially on weekends and consumed marijuana “gummies” on rare occasions. She had no history of recent travel and had never traveled outside of the United States. Her father had recently been released after a year in prison.
Despite the indeterminate MRI findings, her fever put cerebral abscess higher on the differential diagnosis, prompting her physicians to begin empiric antibiotic therapy and perform a lumbar puncture.
CHOOSING AN ANTIBIOTIC REGIMEN
2. Which of the following is the most appropriate empiric regimen for suspected cerebral abscess?
Vancomycin and piperacillin-tazobactam
Cefepime and metronidazole
Ceftriaxone and metronidazole
Vancomycin and metronidazole
Brain abscess is often the result of seeding from oral, otic, or sinus sources, making streptococcal species the most common isolates.3 Empiric coverage is based on the typical flora from these locations, including streptococcal species, gram-negative organisms, and anaerobic pathogens.
Antibiotics that cover methicillin-resistant Staphylococcus aureus, such as vancomycin, could be considered in a postoperative setting or if hematogenous seeding from bacteremia is suspected.
Pseudomonas infection is uncommon except after surgery or in head trauma.4 Thus, it is not necessary to empirically cover them, for example, with piperacillin-tazobactam or cefepime.
The best regimen of those presented above is ceftriaxone and metronidazole, which provides adequate coverage of streptococcal species and anaerobes. However, we chose to add vancomycin in this patient’s case in addition to ceftriaxone and metronidazole due to the unclear etiology of the possible abscess and the severity of the patient’s illness.
CASE CONTINUED: CEREBROSPINAL FLUID STUDIES
Testing for human immunodeficiency virus infection was negative.
On hospital day 5, lumbar puncture with cerebrospinal fluid analysis yielded the following values:
Opening pressure 480 mm H2O (reference range 50–200)
White blood cell (WBC) count 343 × 106/L (reference range 0–5), with 71% lymphocytes and 27% neutrophils
Glucose level 26 mg/dL (reference range 40–70 mg/dL)
Protein 286 mg/dL (reference range 15–45 mg/dL).
INTERPRETING THE CEREBROSPINAL FLUID FINDINGS
3. Which of the following cerebrospinal fluid findings would most strongly indicate bacterial meningitis?
WBC count 800 × 106/L with neutrophilic predominance, glucose 21 mg/dL, protein 110 mg/dL
WBC count 200 × 106/L with lymphocytic predominance, glucose 48 mg/dL, protein 90 mg/dL
WBC count 900 × 106/L with lymphocytic predominance, glucose 34 mg/dL, protein 180 mg/dL
WBC count 800 × 106/L with lymphocytic predominance, glucose 19 mg/dL, protein 160 mg/dL
Analyzing the cerebrospinal fluid is a key part of evaluating suspected meningitis. Bacterial meningitis typically manifests with very elevated WBC counts with neutrophilic predominance, low glucose, elevated protein, and elevated opening pressure. Therefore, the first answer choice above is correct. In contrast, viral infections typically manifest with moderately elevated WBC counts with lymphocytic predominance, elevated protein, normal glucose, and normal or modestly elevated opening pressure.
Our patient’s results were not typical of either of these presentations. While bacterial meningitis should still be considered, the cerebrospinal fluid findings and subacute presentation were more consistent with atypical infection, perhaps with a fungus or Mycobacterium species.
CASE CONTINUED: HER CONDITION WORSENS
A number of tests were ordered and yielded negative results. These included blood cultures, cerebrospinal fluid cultures, cerebrospinal fluid cytology, leukemia panel, lymphoma panel, potassium hydroxide smear, Gram stain, Toxoplasma polymerase chain reaction testing, meningitis polymerase chain reaction panel (including Escherichia coli K1, Haemophilus influenzae, Listeria monocytogenes, Neisseria meningitidis, Streptococcus agalactiae, Streptococcus pneumoniae, cytomegalovirus, enterovirus, herpes simplex virus 1, herpes simplex virus 2, human herpesvirus 6, human parechovirus, varicella zoster virus, and Cryoptococcus neoformans/gattii), antineutrophil cytoplasmic antibody panel, Lyme antibody, 1,3 beta-glucan (a test for fungal cell wall elements), and a screening test for syphilis.
Although the patient had no pulmonary symptoms or signs, results of chest radiography to uncover supporting evidence of infection or malignancy were interpreted as normal (Figure 2).

Chest radiography showed no airspace abnormalities or hilar abnormalities.
On hospital day 6, the patient began reporting a worsening headache associated with blurred vision. She continued to exhibit irritability, intermittently refusing testing and nursing interventions. Her confusion and somnolence worsened. No additional fever was recorded. Cardiopulmonary examinations and peripheral neurologic examinations were normal. The development of disconjugate gaze and esotropia indicated left abducens nerve palsy. Optic disc margins were crisp. Repeat lumbar puncture again demonstrated elevated opening pressure, lymphocytosis, and elevated protein.
Acetazolamide was given to treat the increased intracranial pressure. Her serum sodium began trending downwards at this time and would remain at approximately 130 mg/dL.
Repeat MRI on hospital day 8 revealed several new foci of restricted diffusion compatible with acute infarcts. She underwent transesophageal echocardiography and computed tomography of the chest, abdomen, and pelvis, which showed no signs of pulmonary, cardiac, lymphatic, or skeletal disease. Skin examinations were negative for rashes, nodules, or lesions. Testing for histoplasmosis (by serum antibody testing and antigen enzyme immunoassay), blastomycosis, Coccidioides, and antiphospholipid antibody panel were negative. Cerebrospinal fluid tests for Mycobacterium tuberculosis by polymerase chain reaction, acid-fast stain, and acid-fast culture were negative. However, a blood test for M tuberculosis (T-SPOT) returned positive on hospital day 10.
Before this blood test result was available, her condition worsened on hospital day 10 with lethargy and near-total loss of vision in her left eye. Repeat computed tomographic angiography of the head and neck with transcranial Doppler revealed narrowing in both middle cerebral arteries with mild spasm in the left anterior cerebral artery. At this point, the patient was started on dexamethasone and was transferred to a tertiary care facility.
Approximately 2 days after transfer, her clinical condition deteriorated further. She was started on levetiracetam for suspected seizures and was intubated for her inability to protect her airway. She was treated broadly with amphotericin, rifampin, isoniazid, pyrazinamide, and ethambutol in addition to ceftriaxone and metronidazole. An external ventricular drain was placed to decrease her intracranial pressure.
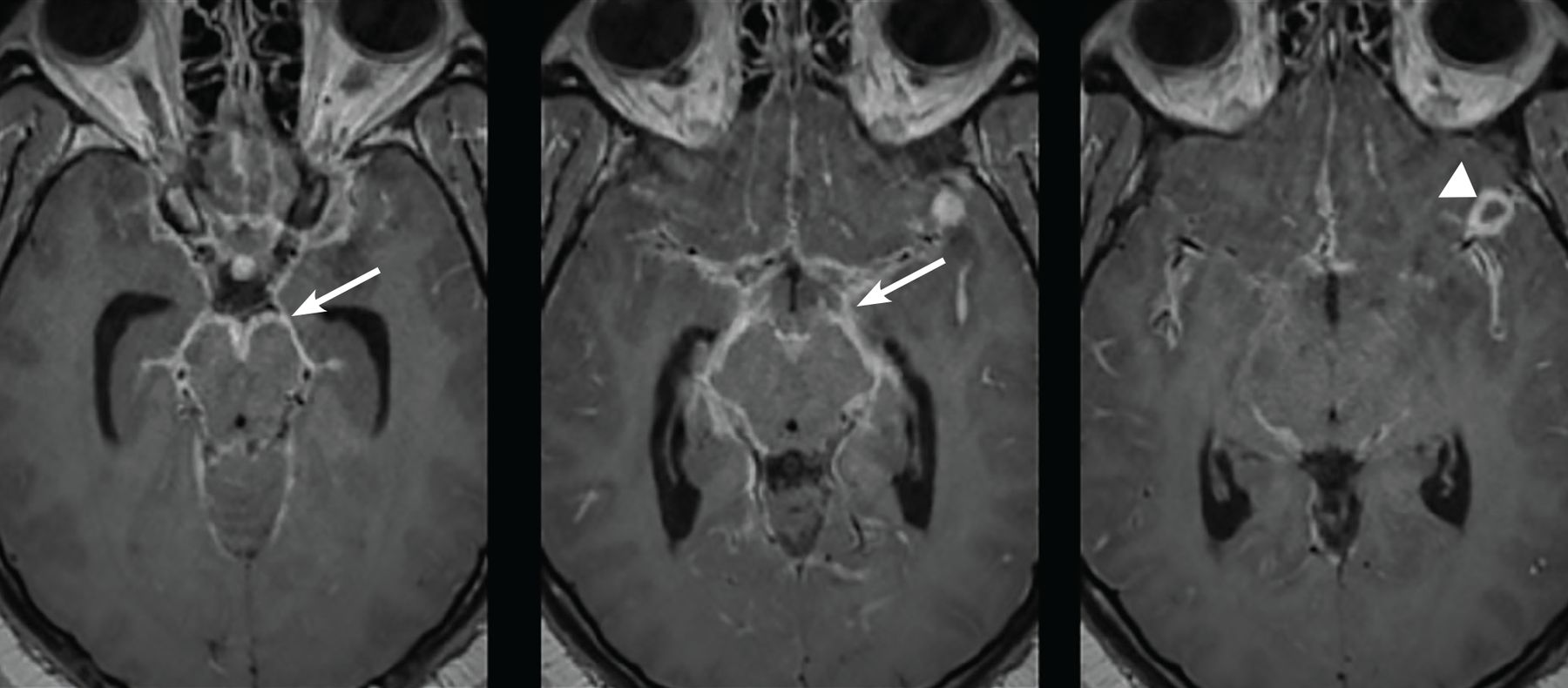
A third MRI showed worsening basilar leptomeningeal enhancement with a persistent peripherally enhancing lesion (Figure 3). Another lumbar puncture was done. Cerebrospinal fluid antigen and antibody testing for histoplasmosis were negative. Repeat acid-fast stain and a nucleic acid amplification test for M tuberculosis (Xpert MTB/RIF assay) were negative. Metagenomic next-generation sequencing detected M tuberculosis complex, but below threshold levels for a confirmed positive result. DNA probe of cerebrospinal fluid culture ultimately confirmed the diagnosis of tuberculous meningitis approximately 2 weeks after the sample was obtained.
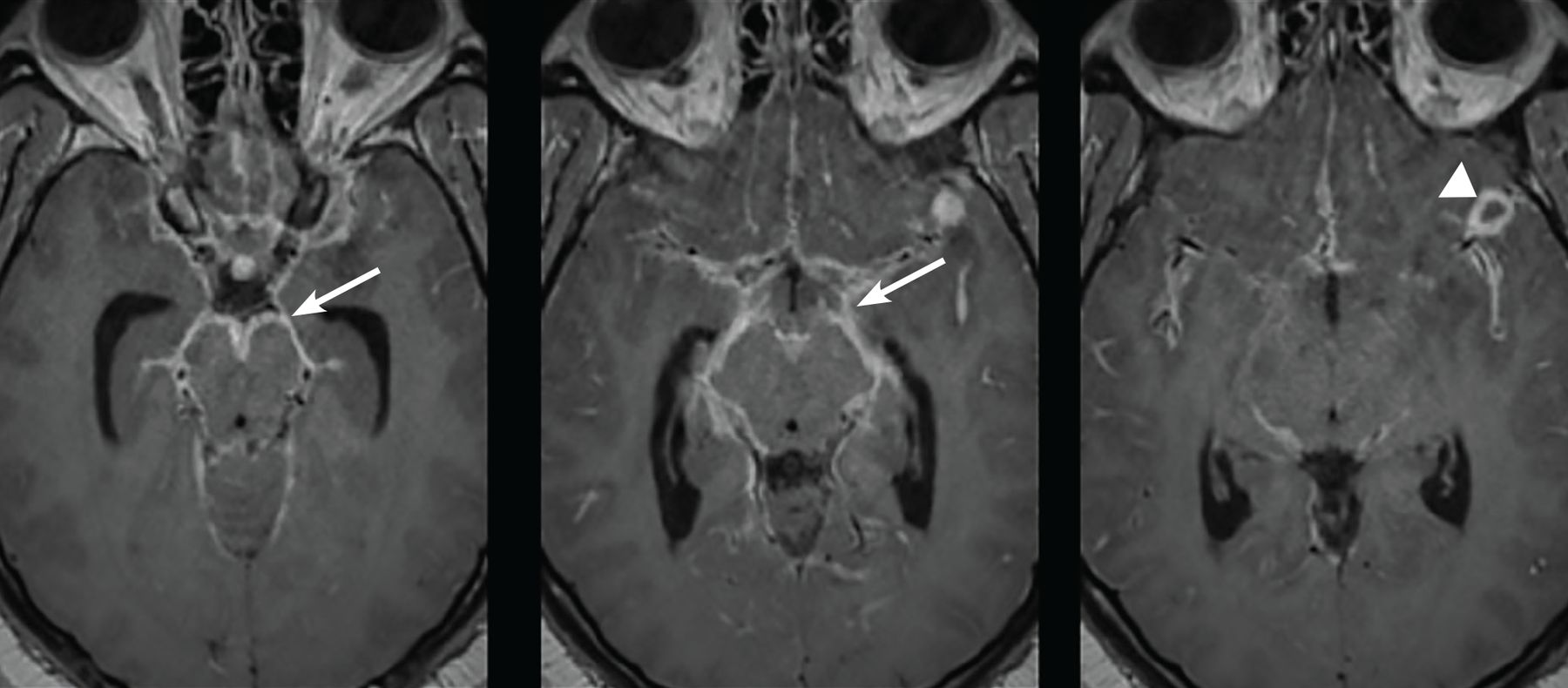
Two weeks later, with the patient’s condition continuing to worsen, magnetic resonance imaging showed bulky leptomeningeal enhancement (arrows), most prominent at the basal surface of the cerebrum, with a peripherally enhancing 1.2-cm lesion at the left sylvian fissure (arrowhead).
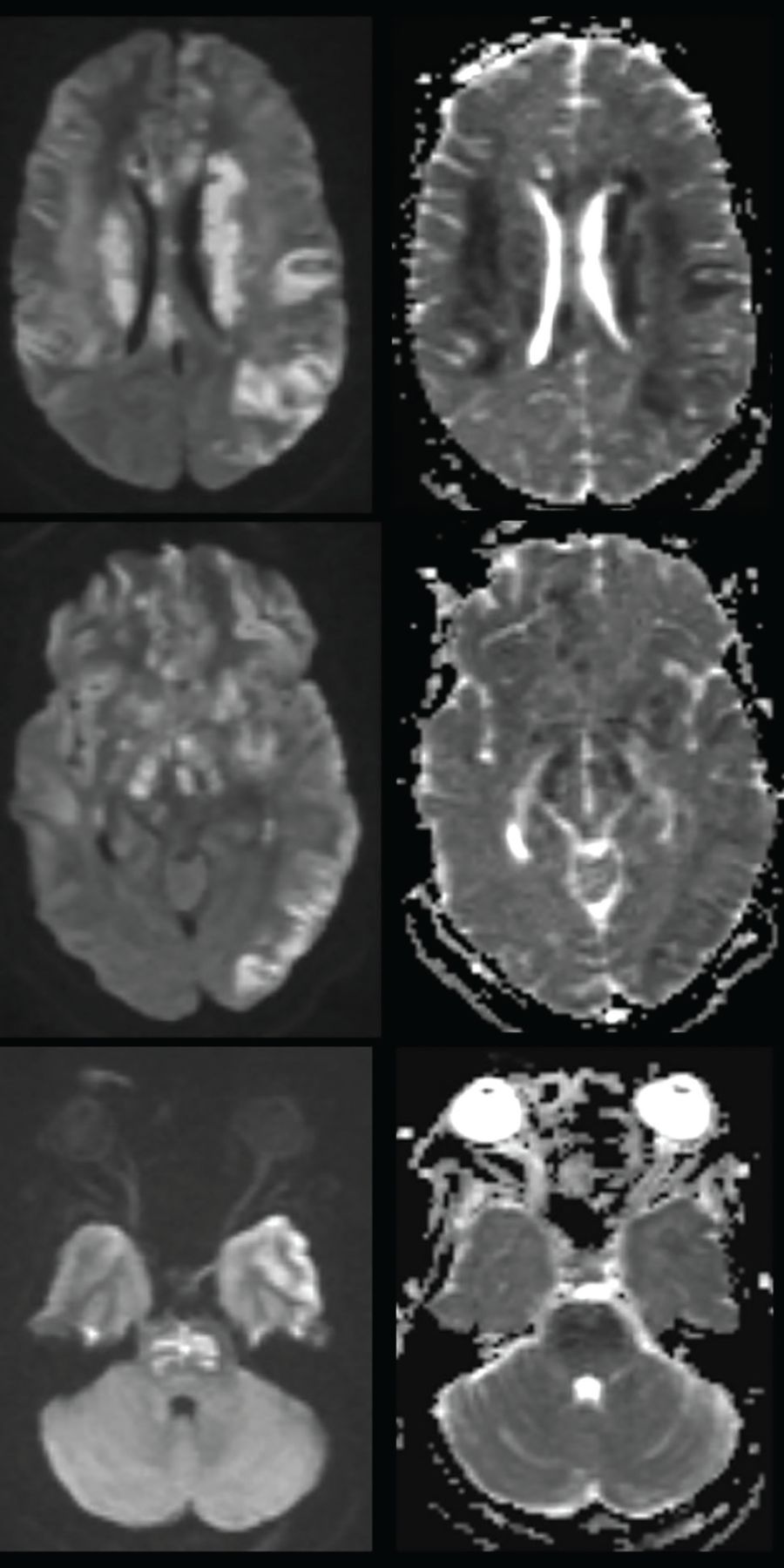
The patient’s intracranial pressure was controlled with barbiturate coma, hypothermia, and paralytics. Despite these interventions, her clinical status did not improve due to extensive cerebral infarcts (Figure 4). She was subsequently transferred to hospice care and died approximately 5 weeks after her initial presentation.
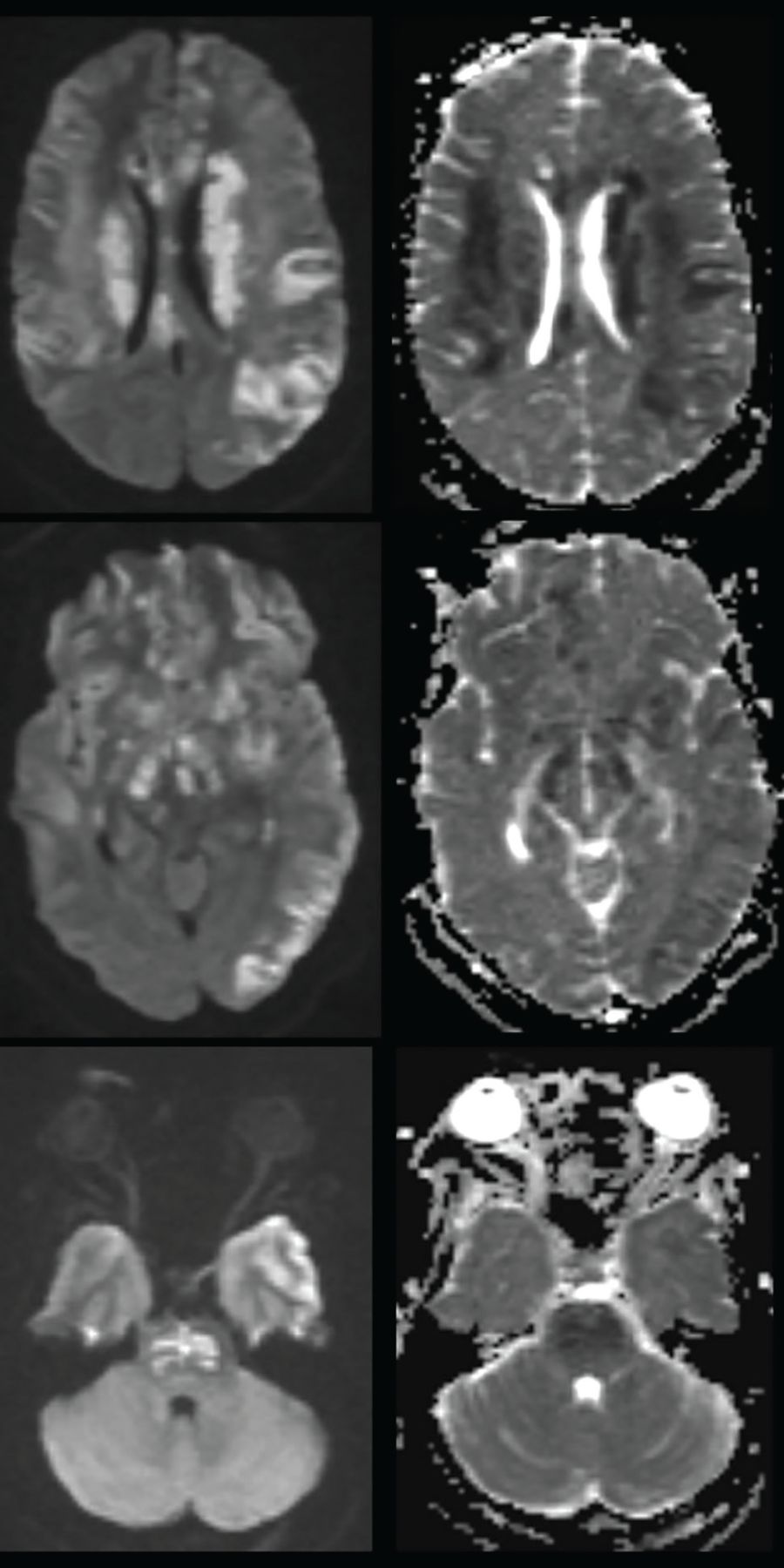
One month after presentation, shortly before the patient died, magnetic resonance imaging showed multifocal areas of patchy parenchymal restricted diffusion that were not associated with localized pathologic enhancement. These features raised suspicion for acute infarction along the genu and body of the corpus callosum, left corona radiata and corpus striatum, juxtacortical left frontal operculum, left temporal stem and anterior temporal white matter, right anterior temporal white matter, anterior commissure and forniceal columns, right posterior limb internal capsule, right hippocampal body, left cingulate gyrus, and left parietal convexity.
TUBERCULOUS MENINGITIS AND VASCULOPATHY
Tuberculosis is often called “the Great Imitator” due to its ability to mimic the clinical presentation of many diseases. In the United States, the prevalence of tuberculosis is low, and extrapulmonary tuberculosis occurs primarily in adults with reactivation disease.
Cases of tuberculous meningitis are increasingly rare in the United States, with only 74 cases reported in 2018.5 However, when it does occur, it is devastating. Short-term mortality rates range from 20% to 69% with standard antituberculosis therapy, and the disease is fatal without treatment.6 It is estimated that more than half of those affected by tuberculous meningitis die or have permanent disability despite antituberculosis treatment.6 The morbidity and mortality underscore the importance of early recognition.
Clinically, tuberculous meningitis can be very difficult to diagnose. A history of an immunocompromised state such as human immunodeficiency virus infection or travel to endemic areas is often present. Among patients with tuberculosis, those with human immunodeficiency virus infection have a fivefold higher likelihood of central nervous system dissemination compared with those without.7 However, as our patient’s case demonstrates, risk factors are not always present. The patient’s father’s incarceration presents a clue, but it is unclear if that was truly the source of her infection. Presentation with neurologic manifestations without prior history of tuberculosis is relatively uncommon, representing as few as 10% of cases in one series.8
Clues to tuberculous meningitis
Some clinical features can point to tuberculous meningitis. Many patients present with a subacute febrile illness that includes malaise and headache. Over a period of weeks to months, the disease progresses and causes meningismus, worsening headache, confusion, and abnormal behavior or personality changes, sometimes accompanied by cranial nerve abnormalities.9
Our patient’s parents believed that her behavioral or personality changes were related to suffering the loss of a close friend. This history, her uncooperative behavior, and our suspicion of substance abuse were red herrings. Further, she had no fever, leukocytosis, or other overt infectious symptoms. Her neck and back pain were attributed to other possible causes, contributing to a delay in diagnosis.
Prodromal, meningitic, and paralytic phases
Untreated, tuberculous meningitis will continue to progress and cause stupor, coma, seizures, and often death. Based on this progression of symptoms, tuberculous meningitis is often said to have 3 phases: prodromal, meningitic, and paralytic. These 3 phases parallel the 3 stages of severity of the illness based on mental status and neurologic signs: fully conscious with no focal defects; conscious but with inattention, confusion, lethargy, and focal signs; and stuporous or comatose, with multiple cranial nerve palsies or complete hemiparesis or paralysis.9 Even when treated appropriately, tuberculous meningitis often paradoxically deteriorates before it improves, resembling a reaction like the immune reconstitution syndrome.10
Associated vasculitis and stroke
Vasculitis leading to stroke can also occur, usually during the paralytic phase, and accompanies 15% to 57% of cases of tuberculous meningitis.11 In such cases, leptomeningeal inflammation and exudate surround the arteries as they traverse the area. The artery most commonly affected by stenosis due to this inflammation is the middle cerebral artery, causing downstream infarcts at perforators and terminal cortical branches. The area most commonly involved is the basal ganglia, particularly the area supplied by the lateral lenticulostriate arteries.12 Branches from the anterior cerebral artery are also commonly involved. This distribution of vasospasm is consistent with the distribution seen in our patient, involving bilateral middle cerebral artery stenosis and left anterior cerebral artery stenosis. Vasculopathy can be a large contributor to the severity of illness, with cerebral infarction an independent predictor of death in tuberculous meningitis.13
Our patient’s diffuse infarctions sealed her fate. Her infarctions involved the left precentral and post-central gyri, left superior and inferior parietal lobules, and dorsal aspect of the left superior middle frontal gyri, suggesting extensive disease in the left middle cerebral artery. In addition, she had infarcts at the lentiform nucleus, left caudate head, genu body and splenium of the corpus callosum, posterior limb of each internal capsule and underlying cerebral peduncles, the basis pontis, the right precentral and postcentral gyri, right opercular cortex, right insular cortex, left precuneus, and the subcortical white matter of both temporal poles.
SUSPECTING AND DIAGNOSING TUBERCULOUS MENINGITIS
Subacute meningitis with middle cerebral artery distribution vasospasm and basilar leptomeningeal enhancement should raise suspicion for possible tuberculous meningitis.14 However, these often only present in later stages of the disease. Furthermore, they are not specific to tuberculous meningitis. Viral and fungal infections can have a similar clinical presentation, emphasizing the importance of early and accurate diagnostic testing.
Testing for histoplasmosis was especially pertinent for this patient, who lived in the Ohio River valley. Evaluation for histoplasmosis optimally includes urinary antigen testing, which is more sensitive than serum antigen or antibody testing.15 Cerebrospinal fluid testing can also be considered, with less robust data suggesting sensitivity around 85% to 98%.15,16
Traditional diagnostic tests for tuberculosis such as acid-fast bacillus smear and culture have low sensitivity for tuberculous meningitis. Thwaites et al17 reported sensitivities of 52% for smear and 64% for culture. Culture is also less clinically useful, as M tuberculosis can take weeks to grow on culture. Our patient had 2 sets of negative acid-fast bacillus smears and cultures, both obtained in the third phase of tuberculous meningitis. One was obtained before starting antibiotics directed at M tuberculosis, which should have made for optimal test results.
The poor sensitivity and the delay in diagnostic results can be mitigated with ancillary molecular diagnostic testing. Nucleic acid amplification can provide rapid results, if it is available. The most utilized is polymerase chain reaction, offering a sensitivity around 82%.18 While it is not approved by the US Food and Drug Administration for testing cerebrospinal fluid samples, it can improve diagnostic yield compared with traditional methods and provides results much more rapidly than culture.
CASE CONCLUSION, LESSONS LEARNED
This patient’s case involved a unique scenario of negative cerebrospinal fluid polymerase chain reaction testing but still high clinical suspicion for tuberculous meningitis, as well as positive blood testing. Factors such as a low-volume cerebrospinal fluid sample, testing early in the course of disease, and low pathogen burden can increase the likelihood of false-negative results. However, none of these were apparently involved in this patient’s case.
When further testing is indicated due to high clinical suspicion and negative results on polymerase chain reaction testing, other molecular diagnostic testing options include metagenomic next-generation DNA sequencing, DNA-probe testing, and the Xpert MTB/RIF assay or Xpert Ultra MTB/RIF assay. In such scenarios, next-generation DNA sequencing can offer an improved diagnostic sensitivity compared with polymerase chain reaction testing, acid-fast bacillus smear, and culture.19 In our patient’s case, it was the first test to detect M tuberculosis in the cerebrospinal fluid, which was later confirmed with DNA-probe testing of the culture weeks later. Clinically, the next-generation DNA sequencing was able to help provide earlier guidance about the need and direction of further testing.
Ultimately, patients without classic risk factors or pulmonary disease pose a significant challenge for clinicians to diagnose tuberculous meningitis. A clinical presentation involving subacute meningitis with cerebrospinal fluid studies indicating increased intracranial pressure and lymphocytic pleocytosis with low glucose should raise suspicion for tuberculous meningitis, but these signs are nonspecific.20 Depending on disease severity and progression, MRI findings indicating vasculopathy or meningeal enhancement with predilection of the basal cisterns may also be present.
Traditional acid-fast bacilli smear and culture have poor sensitivity that can be improved with molecular diagnostic testing. As demonstrated in this patient’s case, the tuberculosis blood test and other serologic tests can help augment cerebrospinal fluid studies, as the latter can be less sensitive. In addition, when high clinical suspicion for tuberculous meningitis is present, metagenomic next-generation DNA sequencing and DNA-probe testing should be considered, as they improve overall sensitivity of cerebrospinal fluid results.
Finally, our patient’s case emphasizes the importance of early antimicrobial therapy against M tuberculosis, in view of the disease’s high rates of morbidity and mortality.
TEACHING POINTS
Tuberculous meningitis should be considered in the differential diagnosis of subacute meningitis and is associated with a poor prognosis.
Vasculopathy leading to cerebral infarction is common with tuberculous meningitis.
Diagnostic confirmation can be difficult in tuberculous meningitis due to delay in culture results. Thus, molecular diagnostics should be considered to help confirm the diagnosis early.
Empiric therapy should be started early when tuberculous meningitis is suspected, in view of its high mortality rate when left untreated.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- INITIAL EXAMINATION
- RING-ENHANCING BRAIN LESIONS
- CASE CONTINUED: WORKUP FOR FEVER AND INFECTIOUS DISEASES
- CHOOSING AN ANTIBIOTIC REGIMEN
- CASE CONTINUED: CEREBROSPINAL FLUID STUDIES
- INTERPRETING THE CEREBROSPINAL FLUID FINDINGS
- CASE CONTINUED: HER CONDITION WORSENS
- TUBERCULOUS MENINGITIS AND VASCULOPATHY
- SUSPECTING AND DIAGNOSING TUBERCULOUS MENINGITIS
- CASE CONCLUSION, LESSONS LEARNED
- TEACHING POINTS
- DISCLOSURES
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.