


A 43-year-old woman presented to the dermatology department with multiple small skin-colored papules on her cheeks (Figure 1) and acrochordons (“skin tags”) on the axillae (Figure 2). She reported that they had appeared over the past few years. Her personal medical history was unremarkable, but she had a first-degree relative with renal carcinoma.

Multiple whitish to skin-colored papules on both cheeks.

Acrochordons on the axillae.
Biopsy of a papule revealed dermal follicular structures surrounded by a perifollicular fibrous sheath and a densely fibrous stroma, consistent with a fibrofolliculoma (Figure 3), ie, a benign hair follicle tumor pathognomonic for Birt-Hogg-Dubé (BHD) syndrome. Subsequent genetic testing found a mutation in the FLCN gene, confirming the diagnosis.
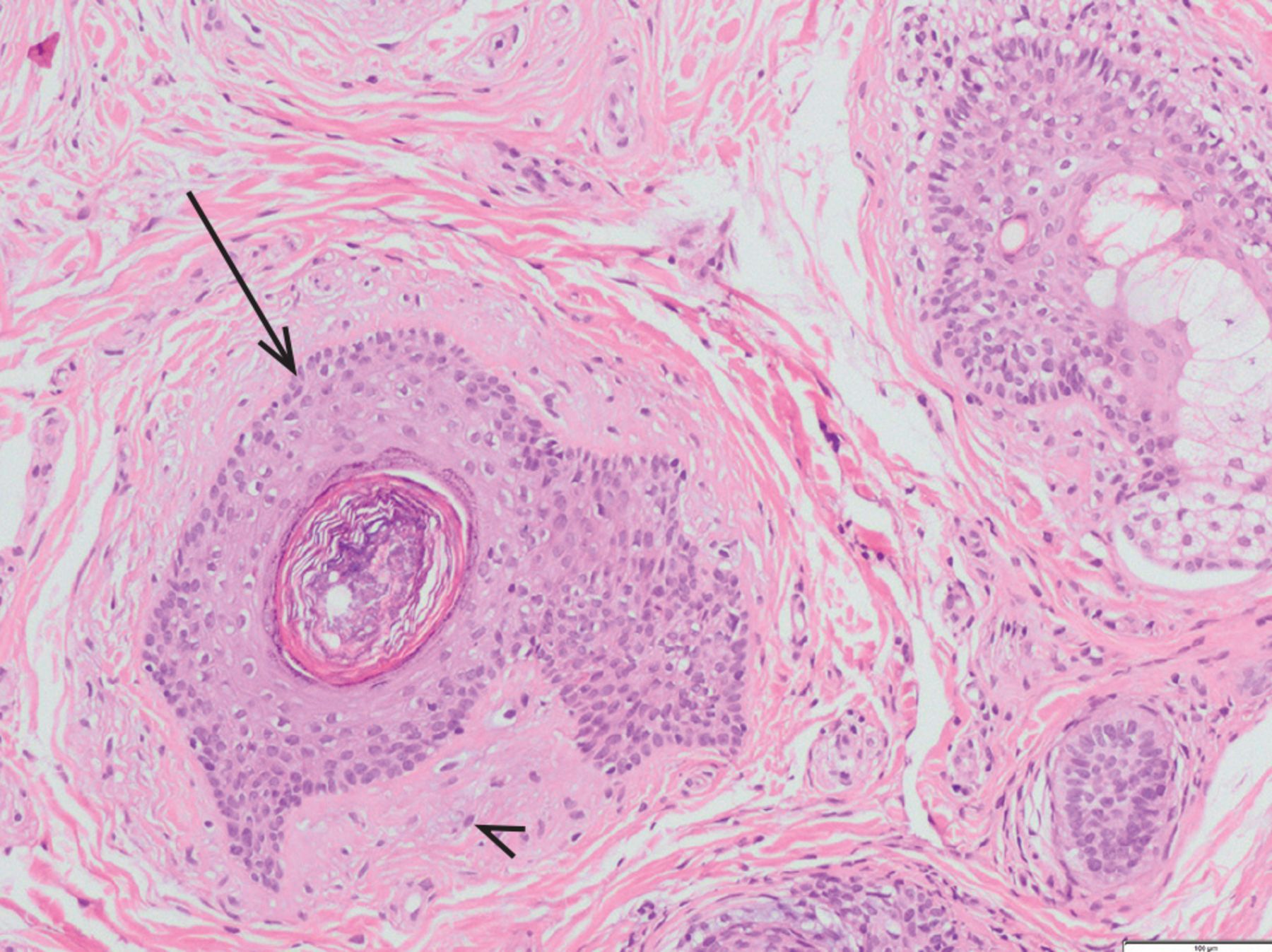
Skin biopsy showing dermal follicular structures (arrow) surrounded by a perifollicular fibrous sheath and a densely fibrous stroma (arrowhead), consistent with fibrofolliculoma (hematoxylin and eosin, × 400).
Computed tomography showed no evidence of lung cysts or kidney tumor. Regular cancer surveillance was instituted.
BHD SYNDROME: SKIN, LUNGS, KIDNEYS
BHD syndrome is an autosomal dominant genetic disorder that predisposes patients not only to characteristic skin lesions but also to the development of lung cysts, spontaneous pneumothorax, and kidney neoplasms. It is caused by inactivating mutations in the gene that codes for folliculin, a protein that likely acts as a tumor suppressor. Most studies suggest that folliculin plays a role in the mammalian target of rapamycin (mTOR) pathway.1,2
Prevalence of BHD syndrome is uncertain. It is likely underdiagnosed, especially as more than 150 pathogenic variants with variable penetrance have been described.3,4 Some studies suggest that BHD syndrome may be the cause of 5% to 10% of cases of apparent primary spontaneous pneumothorax.3
Skin manifestations often arise first
First clinical manifestations tend to appear in the second or third decade. Many patients with BHD syndrome (75% to 90% of White patients, but only 30% to 50% of Asian patients) present with multiple fibrofolliculomas.2,4 They are rarely seen in the general population.
BHD syndrome should be suspected in patients with more than 5 fibrofolliculomas. Histologically, they appear as epithelial cells arranged in rows growing from a central aberrant hair follicle, surrounded by a thick connective-tissue stroma.1
Other dermatologic manifestations may include trichodiscomas, perifollicular fibromas, and acrochordons. These benign tumors, including fibrofolliculomas, are considered hamartomas (ie, abnormal development of normal tissue) of the hair follicle. They may be indistinguishable from each other, and some argue that they are variants of the same lesion.4 Fibrofolliculomas and trichodiscomas present as multiple, small, whitish papules, most commonly on the face, neck, and upper trunk. Acrochordons are small, pedunculated outgrowths of epidermal and dermal tissue in the neck, eyelids, upper chest, and axillae, and they may be reported as fibrofolliculomas on histology.4
Pulmonary involvement commonly develops
Over 80% of patients develop multiple, bilateral pulmonary cysts in the fourth to fifth decades,1,2,4 with up to 38% of patients experiencing at least one pneumothorax.1 Larger number and size of cysts are associated with greater likelihood of spontaneous pneumothorax, but no clear association of BHD syndrome with pulmonary cancers has been found.4
Risk of renal carcinoma is markedly increased
Patients with BHD may have a 7-fold higher risk of renal cell cancer than the general population, with an estimated prevalence between 27% and 34%.1 Frequent histologic subtypes are chromophobe and oncocytic hybrid tumors, but they rarely show sarcomatoid transformation and generally have a favorable prognosis.5 Tumors in the same kidney may also be of different histologic types, but the significance of this for prognosis is not clear.2
MONITORING
An exact monitoring strategy has not been universally established. Risk of excessive radiation exposure from repeated computed tomography scans must be balanced with the relatively low risk of the slow-growing renal cancers associated with BHD syndrome: 12% to 34% of patients with BHD develop renal tumors.4
Most recommend periodic magnetic resonance imaging of the kidney, with the schedule (1 or 2 years) depending on past findings.6 Routine lung screening is not recommended.7 Periodic monitoring for cancers in other organs that may be associated with BHD syndrome—including the parotid, thyroid, and colon—is also recommended.7
TAKE-HOME POINTS
BHD syndrome is a genetic disorder caused by FLCN gene mutations that predispose patients to develop lung cysts, spontaneous pneumothorax, and renal neoplasms.
Multiple fibrofolliculomas and trichodiscomas are benign cutaneous lesions that provide a clue to BHD.
Upon diagnosis of BHD, screening with regular imaging is prognostically crucial for these patients, since identification of lung cysts and renal malignancies at early stages significantly improves life expectancy.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.