


A 44-year-old woman presented to the emergency department following 1 week of sudden, painless, central vision loss in the left eye and 1 day of headache preceded by intermittent floaters and flashing lights. The headache was a dull, aching pain in the left temple. For the preceding 2 months, she had been treated by an outside ophthalmologist for bilateral anterior uveitis, unresponsive to topical prednisolone. She additionally noted recent hair loss and a rash on the palms. She denied light sensitivity, eye pain, trauma, blurred vision, fever, chills, chest pain, shortness of breath, abdominal pain, nausea, dizziness, blurred vision, or syncope prior to presentation.
Medical comorbidities included 15 years of systemic lupus erythematosus (SLE) and antiphospholipid syndrome that first manifested as a cerebrovascular accident (CVA). Serum analysis at time of SLE diagnosis revealed strongly positive antinuclear antibodies, elevated Sjögren syndrome antibodies, double-stranded DNA, beta-2-glycoprotein immunoglobulin G, anticardiolipin immunoglobulin G, and lupus anticoagulant.
The patient’s presentation of vascular thrombosis with positive antiphospholipid antibodies met the Sydney criteria for diagnosis of triple-positive antiphospholipid antibody syndrome. Following appropriate anticoagulation, she experienced occasional skin rashes, Raynaud phenomenon, and sicca symptoms. Other medical comorbidities included migraines and focal epilepsy. Her regular medications included prednisone 7.5 mg daily, methotrexate, hydroxychloroquine, warfarin, and topiramate. She was sexually active.
INITIAL EVALUATION AND MANAGEMENT
At presentation, the patient’s temperature was 99.1°F (37.3°C), heart rate 80 beats per minute, blood pressure 131/80 mm Hg, respiratory rate 20 breaths per minute, and oxygen saturation 100% on room air. She was alert and oriented and mildly uncomfortable but not in distress. Head examination demonstrated patchy alopecia. Extremity sensation and strength were normal. Skin examination revealed a scaly, erythematous rash on both palms. Her joint examination was unremarkable, and there was no cervical, supraclavicular, axillary, or inguinal lymphadenopathy.
Visual acuity was 20/20 in the right eye and 3/200 in the left eye. Pupils were equally round and reactive to light without an afferent pupillary defect. Confrontation visual field testing revealed central scotoma in the left eye. Extraocular muscles functioned properly in both eyes. Slit-lamp microscope examination demonstrated mild to moderate anterior chamber and vitreous cellular reaction, indicating the presence of anterior and intermediate uveitis. Dilated funduscopic examination demonstrated blunted foveal reflex suggestive of retinal involvement and bilateral panuveitis.
Laboratory test results
Notable results of blood testing at presentation were as follows:
Hemoglobin 10.6 g/dL (reference range 11.6–15.0)
Mean corpuscular volume 93.7 fL (78.2–97.9)
Red blood cell distribution width 15.5% (12.2–16.1)
Platelet count 296 × 109/L (157–371)
Total leukocyte count 8.2 × 109/L (3.4–9.6)
Neutrophils 6.43 × 109/L (1.56–6.45)
Lymphocytes 1.19 × 109/L (0.93–3.07)
Monocytes 0.53 × 109/L (0.26–0.81)
Eosinophils 0.04 × 109/L (0.03–0.48)
Basophils 0.03 × 109/L (0.01–0.08)
International normalized ratio (INR) 3.6 (0.9–1.1)
Activated partial thromboplastin time (aPTT) 48 seconds (25–37)
Glucose 152 mg/dL (70–140)
C-reactive protein 0.4 mg/dL (≤ 0.8)
Serum creatinine 0.79 mg/dL (0.59–1.04).
Findings on imaging
Computed tomography of the head without contrast revealed no evidence of acute intracranial or orbital bleed, infarction, or mass effect. There was evidence of old infarction in the frontoparietal region and left parietal lobe, mild generalized cerebral atrophy, and ex vacuo ventricular dilation.
DIFFERENTIAL DIAGNOSIS
1. What is the most likely cause of the patient’s symptoms?
SLE
Sarcoidosis
Lyme disease
Syphilis
After a full day of an associated headache, the patient experienced unilateral, painless, progressive vision loss for 1 week following a 2-month history of bilateral anterior uveitis that was unresponsive to corticosteroids. Her lab results revealed mild normocytic anemia, appropriate anticoagulation, and mildly elevated random glucose in the absence of diabetes. Given her CVA history and antiphospholipid syndrome diagnosis, imaging studies appropriately ruled out CVA and intracranial bleeding, and ophthalmic examination excluded retinal artery or vein occlusion. Additionally, retinal toxicity owing to chronic hydroxychloroquine use was rejected based on examination and pattern of vision loss (central vs ringed scotoma). Overall, ocular examination and history were consistent with chronic panuveitis.
Uveitis refers to inflammation of the uveal tissues, specifically the iris, ciliary body, and choroid.1 It also commonly affects tissue or space adjacent to the uvea such as the anterior chamber, vitreous humor, or retina.2 It is subdivided by anatomic location (Table 1).2 Each form of uveitis may present with vision loss, necessitating a detailed ophthalmologic workup augmented by serum testing to determine underlying cause.3 Anterior uveitis encompasses inflammation of the iris or ciliary body and typically presents with a red, painful eye and cellular reaction in the anterior chamber on slit-lamp biomicroscopy.1 Intermediate uveitis includes inflammation of the vitreous and peripheral retina and presents with worsening eye floaters, decreased vision, and cells in the vitreous on examination.4 Posterior uveitis involves inflammation of the retina and choroid and presents with deteriorating vision and visual field changes.5 Panuveitis involves global inflammation that may present with symptoms from each of the previous categories.6
Uveitis
Systemic lupus erythematosus
Though SLE can involve any structure within the eye, uveitis is an uncommon ophthalmologic manifestation of SLE (0.47%).7 SLE more commonly causes corneal manifestations such as keratoconjunctivitis due to secondary Sjögren syndrome.8 Retinal vasculopathy is another common ocular finding that additionally presents with cotton wool spots on funduscopic examination in SLE patients.8 Given our patient’s uveitis and lack of corneal manifestations or retinal vasculopathy, an SLE flare was unlikely to be contributing.
Sarcoidosis
Ocular sarcoidosis occurs in 25% to 50% of patients with systemic sarcoidosis.9–12 Ocular sarcoidosis typically presents in younger individuals as anterior uveitis compared with panuveitis in middle and older age patients.9 Advanced disease can affect all structures of the eye.9 Most sarcoid uveitis is bilateral, and approximately 90% of patients experience chronic sarcoid uveitis, as our patient. However, it is rare for adults to present with sarcoid uveitis without concurrent pulmonary manifestations.13–15 Thus, sarcoidosis is less likely.
Lyme disease
Infection causes roughly 20% of all uveitis, including, but not limited to, viruses (cytomegalovirus, herpes simplex virus, varicella-zoster virus), bacteria (Lyme disease, syphilis, tuberculosis, bartonellosis), and parasites (toxocariasis).16–18 Borrelia burgdorferi, the spirochete responsible for Lyme disease, can directly invade the eye to produce acute or chronic visual symptoms.19,20 The principal symptom of Lyme ophthalmic involvement is decreased vision.21 Although there are reports in the literature, uveitis due to Lyme is exceedingly rare and should only be suspected if the patient has systemic signs and symptoms in combination with plausible risk factors for Lyme disease, such as outdoor activities, known tick bite, and a characteristic rash.22,23 The absence of these characteristics places Lyme uveitis low on the differential.
Syphilis
Treponema pallidum is the spirochete responsible for syphilis.24,25 Ocular syphilis is a form of neurosyphilis characterized by involvement of the eye. It can present at any stage of a syphilitic infection but is quite rare with estimates of 0.6% of patients with syphilis presenting with ocular syphilis.24 The most common manifestation of ocular syphilis in an HIV-negative patient is posterior uveitis, though anterior uveitis and panuveitis can occur.26 These can all present as decreased vision, necessitating further ophthalmologic workup and serum treponemal testing.3
Our patient’s presentation of decreased vision associated with panuveitis, in addition to patchy alopecia and previous rash on the hands raises suspicion for ocular syphilis. Of note, neurosyphilis can present as acute ischemic stroke with the prodromal symptom of a mild headache.25 Reassuringly, imaging studies ruled out ischemic stroke in our patient.
NEXT STEPS
In the setting of uveitis, further investigation hinges on advanced ocular imaging and appropriate lab testing for an underlying cause, which includes syphilis testing, angiotensin-converting enzyme for sarcoidosis, Lyme serologies, and QuantiFERON gold or purified protein derivative for tuberculosis. Multidisciplinary evaluation is essential and advanced ocular imaging may include macula optical coherence tomography, fundus autofluorescence, and fluorescein angiography to reveal subtle details not appreciated clinically.
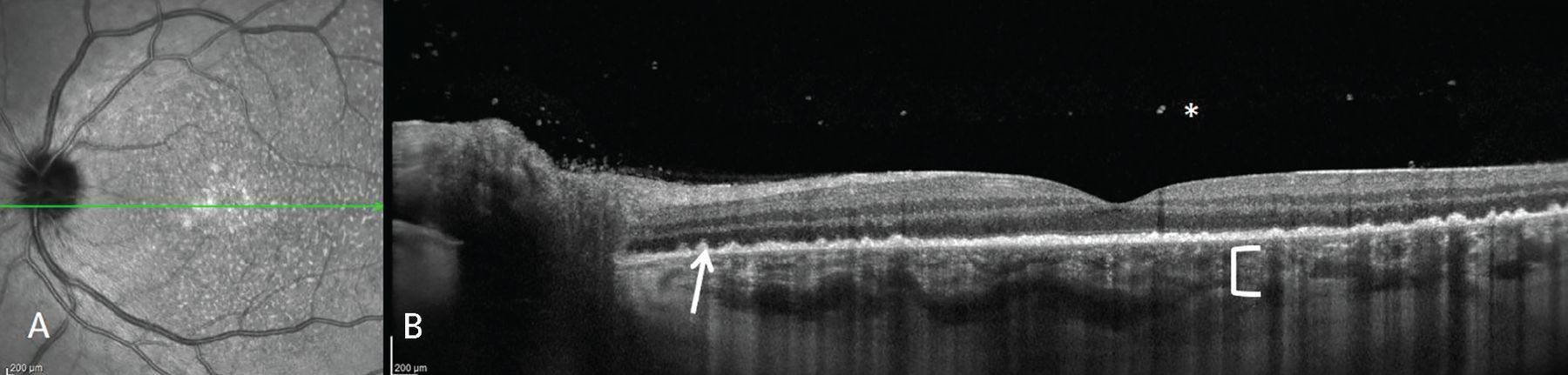
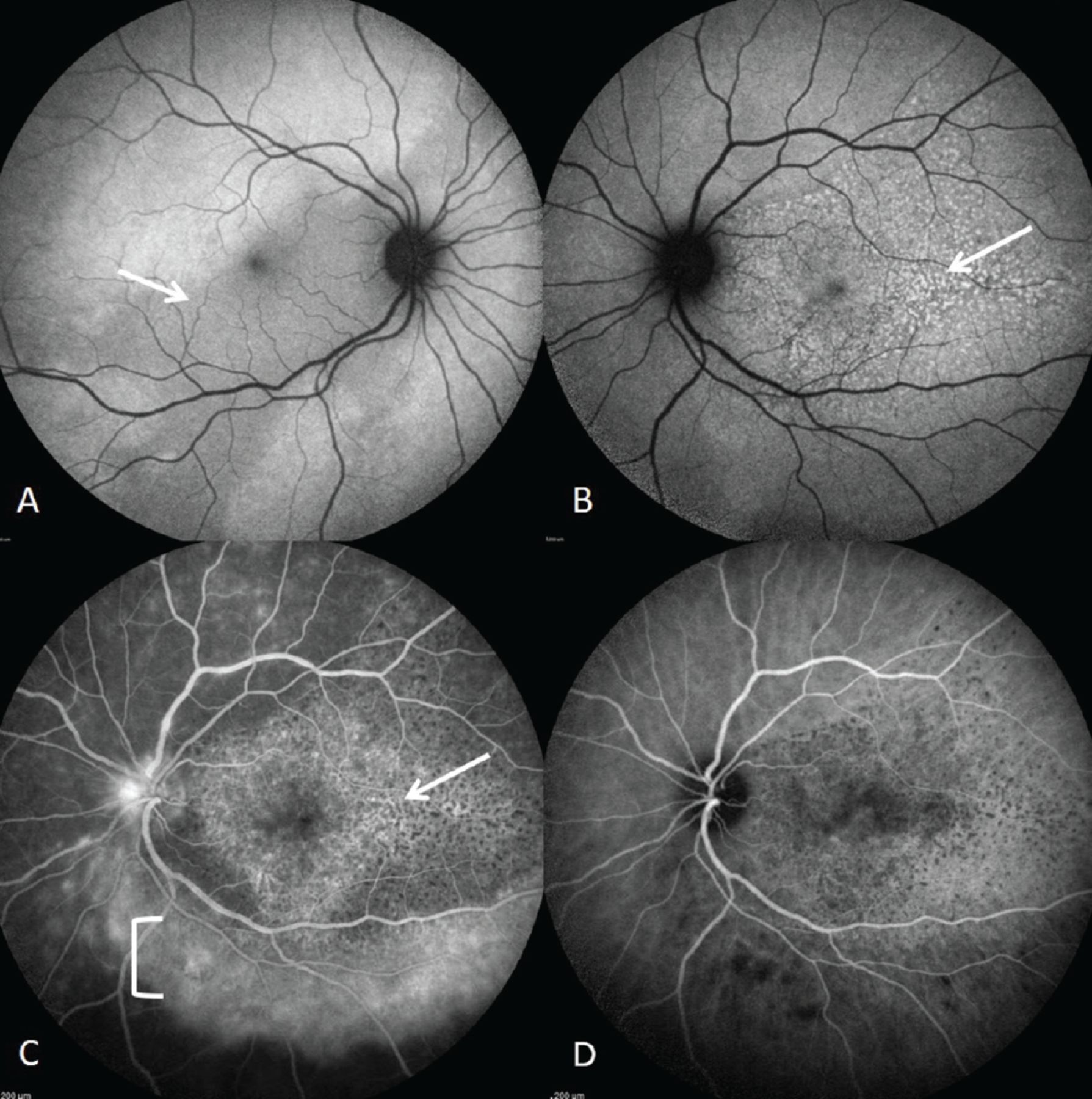
Ocular imaging in our patient demonstrated inflammatory cells in the vitreous as well as retinal and subretinal infiltrates (Figure 1). When combined with autofluorescence imaging that revealed a pattern of mixed hypo- and hyperautofluorescence of the retina, commonly referred to as “leopard spotting,” these findings were characteristic of acute syphilitic posterior placoid chorioretinitis—a hallmark finding of ocular syphilis (Figure 2).27
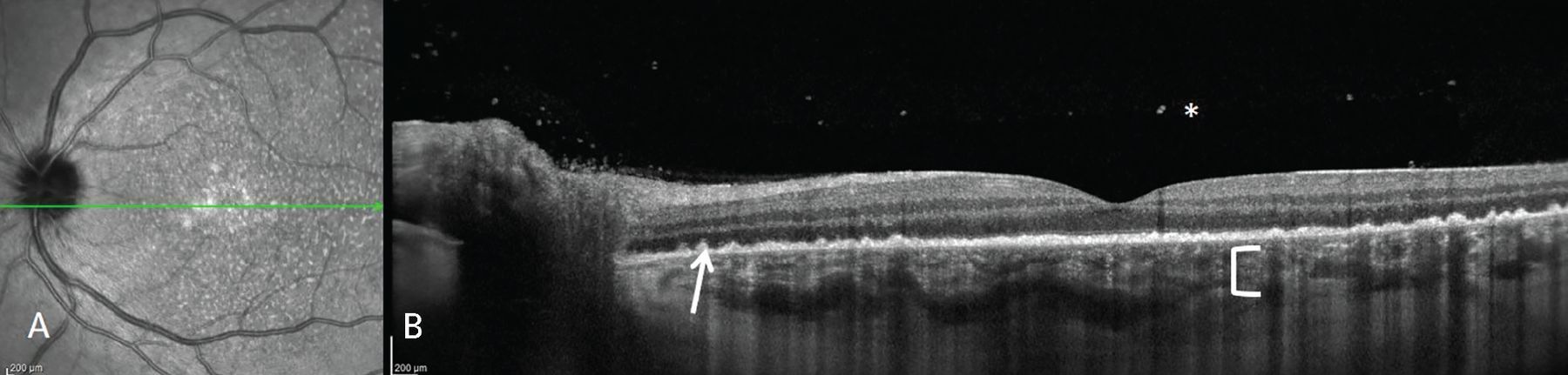
(A) Near infrared reflectance and (B) corresponding macula optical coherence tomography of the left eye, derived from the green line in image (A), demonstrate subretinal infiltrates (white arrow) and increased choroidal hypertransmission (white bracket) due to outer retinal atrophy. Vitritis is shown with a white asterisk.

Fundus autofluorescence of right and left eye. (A) In the right eye, there is a placoid appearance in the macula (white arrow). (B) In the left eye, there is a stippled pattern of hyperautofluorescence and hypoautofluorescence scattered throughout the macula (white arrow). (C) Fluorescein angiography and (D) indocyanine green angiography of the right eye demonstrate a stippled pattern of hyperfluorescence with regions of hypofluorescence owing to blocking consistent with the location of the subretinal infiltrates (white arrow in C; similar finding in D). Just inferior to the inferior vascular arcade, there is a band of perivascular hyperfluorescence consistent with perivascular staining (white bracket).
2. What is the most appropriate testing sequence for syphilis in this patient?
Nontreponemal (eg, rapid plasma reagin [RPR] or venereal disease research laboratory [VDRL]), treponemal (eg, fluorescent treponemal antibody absorption [FTA-ABS]), cerebrospinal fluid (CSF) testing
Treponemal, nontreponemal, CSF testing
Darkfield microscopy
CSF testing, treponemal, nontreponemal
Nontreponemal tests rely on reactivity of antibodies in patient serum to cardiolipin-cholesterol-lecithin antigen.28 Titration of nontreponemal tests provides quantitative measure of disease. Examples include RPR and VDRL titers. Treponemal tests detect antibodies against specific T pallidum antigens. The most common example is the FTA-ABS test.28
Treponemal tests have historically been more complex and expensive to perform than nontreponemal tests, leading to traditional screening of an initial nontreponemal test followed by confirmatory treponemal test, if reactive.28 However, newer versions of treponemal tests are automated, facilitating ease of use.28
Thus, the most appropriate testing sequence for this patient is a treponemal test, such as FTA-ABS followed by reverse screening with a nontreponemal test, such as an RPR or VDRL titer.29,30 Reverse screening is also preferred in suspected late stage syphilis—as with most ocular syphilis—where serum nontreponemal tests may be negative but treponemal tests remain positive.31
Because ocular syphilis is a manifestation of neurosyphilis, in patients with suspected neurosyphilis, VDRL can be performed on CSF after positive serum testing, but should not delay initiation of treatment.32 This is particularly useful in determining diagnosis in patients without ocular symptoms or examination findings.32 Darkfield microscopy is complex and no longer routinely recommended or available.33
Of special consideration in our patient, nontreponemal tests may return false-positive in patients with antiphospholipid syndrome when anticardiolipin antibodies are present.34 The reverse screening technique is particularly useful in this circumstance, as FTA-ABS and other treponemal tests do not rely on reactivity of cardiolipin in patient serum.28
CASE CONTINUED
The patient’s serum FTA-ABS returned positive, and serum RPR titer was reactive and remained reactive to a titer of 1:512. The patient revealed having an unprotected sexual encounter 4 months prior. The patient was admitted to inpatient medicine for lumbar puncture to confirm neurosyphilis and treatment. Because of her history of CVA in the setting of antiphospholipid syndrome, the patient required bridging anticoagulation for the lumbar puncture to be performed safely. Lumbar puncture and CSF analysis revealed elevated protein of 68 mg/dL (reference range 0–35), normal glucose of 57 mg/dL (50–80), 37 nucleated cells per microliter (0–5), and CSF VDRL that remained reactive to a titer of 1:1—consistent with neurosyphilis. Serum HIV testing was negative.
3. What should be the next step in this patient’s management?
Intravenous penicillin G infusions 3 million units every 4 hours
Intramuscular procaine penicillin G 2.4 million units daily and oral probenecid 500 mg
Intramuscular ceftriaxone injections
Close monitoring, testing for additional sexually transmitted infections, and repeat lumbar puncture studies in 3 months
Intravenous penicillin G infusions of 3 to 4 million units should be given every 4 hours for 10 to 14 days, or penicillin G 24 million units as a continuous infusion for 10 to 14 days.30 Allergic patients should undergo penicillin desensitization and proceed with either of the above 2 options.32
Intramuscular procaine penicillin G injections plus probenecid has not been well studied in the treatment of neurosyphilis, and central nervous system levels of oral/intramuscular penicillin are often undetectable.35–37 Oral probenecid is believed to increase the bioavailability of penicillin in the CSF by inhibiting excretion of penicillin in the urine through blockade of the organic anion transporter in the proximal convoluted tubule.35,36 Though early data suggest effectiveness of lumbar puncture penicillin plus pro-benecid in the treatment of neurosyphilis,32,38 intravenous penicillin remains the preferred treatment.37
Intramuscular ceftriaxone injections are an appropriate alternative to intravenous penicillin G in patients allergic to penicillin who remain poorly responsive after resensitization and challenge.30,39,40
Close monitoring. Following penicillin infusion, monitoring for Jarisch-Herxheimer reaction after antibiotic treatment is essential.30 Endotoxins released from lysed spirochetes induce fevers, chills, myalgias, headache, tachycardia, and vasodilation with resultant mild hypotension and flushing.30 It occurs within 2 to 24 hours of antibiotic administration and resolves within 12 to 24 hours.30 Treatment is symptomatic, and acetaminophen is the preferred agent.30,41
SYPHILIS
Syphilis is a sexually transmitted systemic disease caused by infection with the spirochete bacteria T pallidum.30 A moniker of “the great imitator” befits syphilis for its numerous and often vague clinical presentations.30,42 Syphilis classically progresses through 3 stages of increasing severity.42 Primary syphilis commonly presents with a solitary, painless genital chancre in response to local invasion by the bacteria.42 Chancres can present on any skin surface that was in direct contact with an infected lesion, including the digits, nipples, and oral mucosa.42 Secondary syphilis results from systemic hematogenous bacterial dissemination of an untreated primary infection.43 The clinical manifestations in this stage are often nonspecific, but can include condyloma lata, a generalized maculopapular rash involving the hands and feet, and alopecia, in addition to symptoms of myalgia, headache, and malaise among many others.43 Primary and secondary syphilis often improve within weeks but can regress into a latent phase only detectable by serologic testing. Months or years later, some patients progress to the tertiary (late) stage, characterized by cardiovascular involvement resulting in aortic aneurysm, valvulopathy, and/or organ infiltration with gummas.44,45
Neurosyphilis refers to T pallidum spread into the central nervous system and can manifest in any stage of the disease. Five types of neurosyphilis exist, with severity ranging from asymptomatic in early forms to general paresis and tabes dorsalis in the late forms, years or decades after initial infection.30 CSF non-treponemal testing should be performed in patients with suspected neurosyphilis.
Ocular syphilis is a form of neurosyphilis that often presents as posterior uveitis or panuveitis, though almost any ocular structure can be involved.46 Posterior placoid chorioretinitis is a characteristic yellowish plaque lesion near the macula that may be identified through fundoscopy in patients with secondary and tertiary syphilis.47
Management considerations
Broad testing for sexually transmitted infections and repeat lumbar puncture with basic labs should be considered at 3 months.48,49 Repeat lumbar puncture is not indicated in most patients, however, should be considered in immunocompromised patients, such as ours. Patients need to be followed with serial non-treponemal tests at 3 months and every 6 months thereafter to confirm disease eradication.50
Failure of titers to be reduced by 4-times within 6 to 12 months indicates inadequate response to treatment (eg, 1:64 to 1:16).32 A clinical cure is indicated by seroreversion—loss of antibodies and negative nontreponemal test. Retreatment is indicated if a patient fails to experience a 4-fold decrease of CSF VDRL titer by 1-year post-treatment, if there is a 4-fold increase in CSF VDRL titer, or if CSF white blood cell count has not decreased after 6 months or normalized after 2 years.50
CASE CONCLUSION
Intravenous penicillin was initiated and tolerated well without development of Jarisch-Herxheimer reaction. Two weeks of continuous penicillin infusion yielded full visual recovery to 20/20 acuity in both eyes. Given the patient’s immunocompromised status and recommendation of our Infectious Disease colleagues, repeat CSF evaluation was performed at 3 months to monitor disease resolution, which confirmed eradication.
TAKE-HOME POINTS
Syphilis is an important consideration for patients presenting with subacute vision loss.
Identify syphilis using preferred “reverse screening” of treponemal assay followed by nontreponemal assay for confirmation.
Treatment of neurosyphilis should include penicillin G infusion with close monitoring for Jarisch-Herxheimer reaction.
Confirm eradication of disease with nontreponemal tests, consider repeat CSF testing for eradication in immunocompromised patients, and pursue broad testing for other sexually transmitted infections and related age-appropriate cancer screening (cervical cancer).
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2023 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.