


Article Figures & Data
Figures
- Figure 1
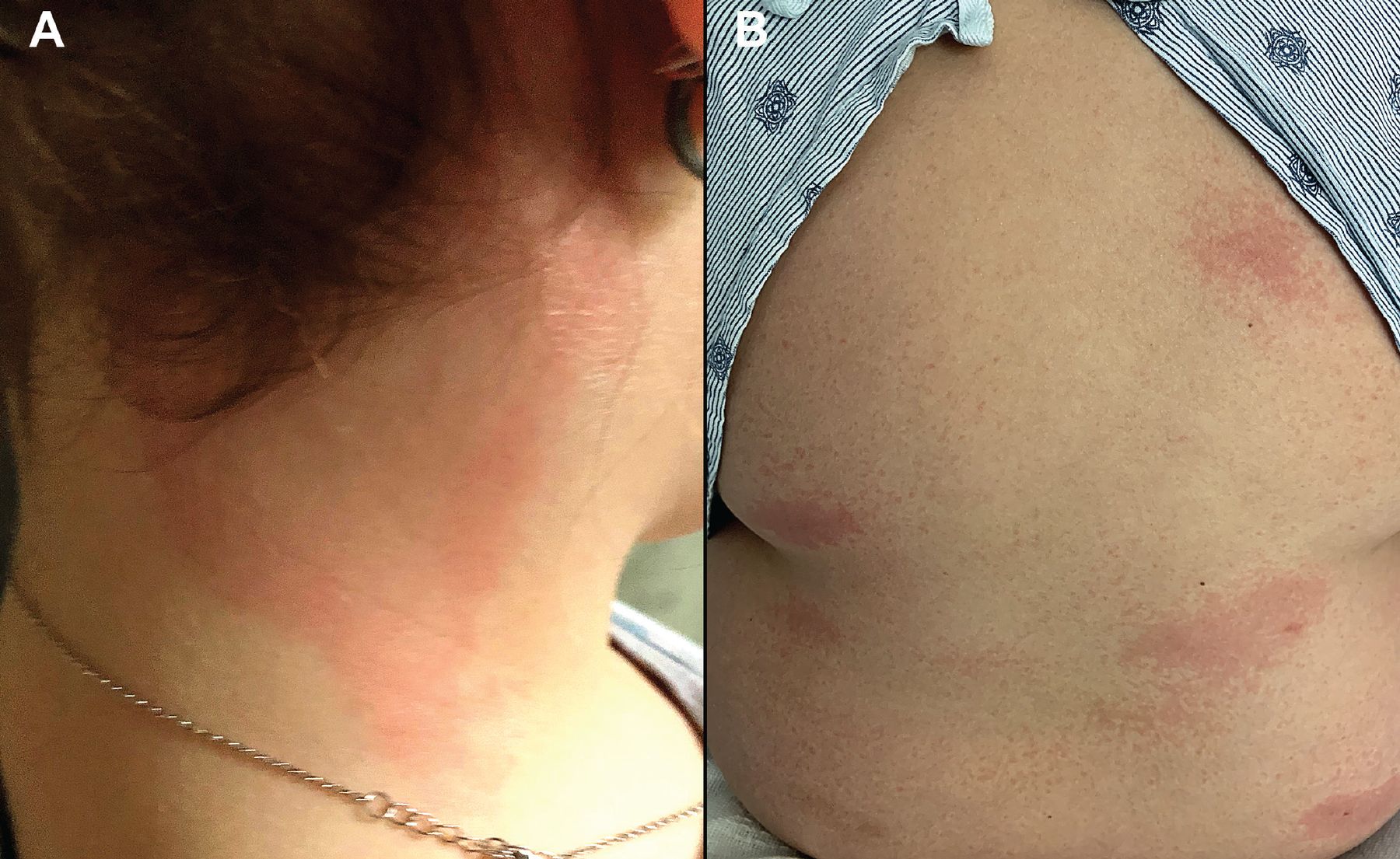
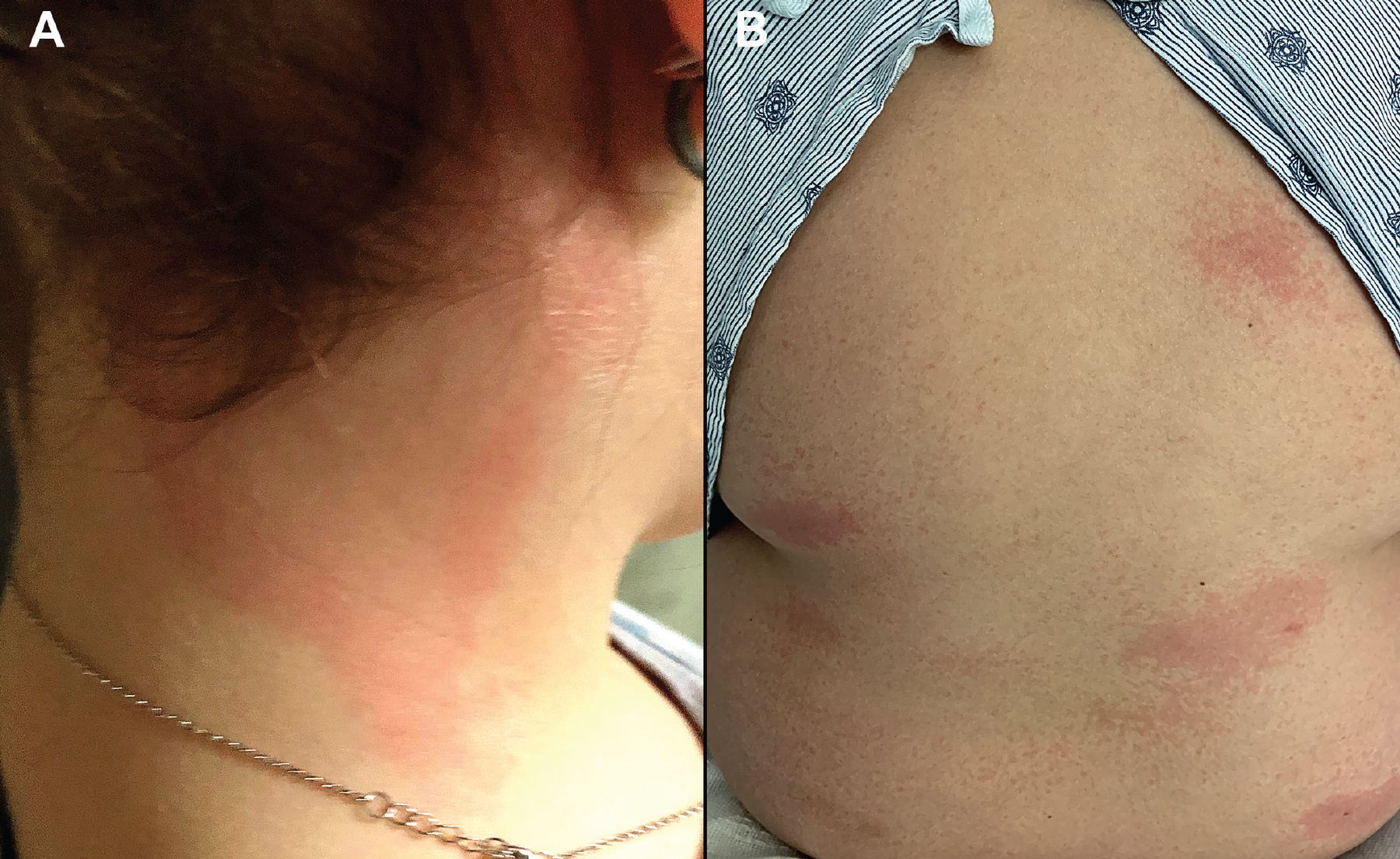
(A) A previously healthy 11-year-old girl with known COVID-19 exposure was hospitalized after 5 days of fever along with bilateral neck erythema and swelling. Workup revealed mildly reduced left ventricular ejection fraction of 47%, elevated erythrocyte sedimentation rate of 60 mm/hr, and a highly elevated C-reactive protein of 15.3 mg/dL, resulting in a diagnosis of multisystem inflammatory syndrome in children. The patient was treated with intravenous immunoglobulin G, steroids, and antithrombotics, with subsequent improvement in left ventricular ejection fraction and rash. She was discharged home with close clinical follow-up. (B) A previously healthy 10-year-old boy was admitted to the pediatric intensive care unit with 5 days of fever, nausea, vomiting, and erythematous, blanchable patches on the back and extremities that began 1 month after confirmed COVID-19 infection. His condition stabilized after treatment with intravenous steroids and immunoglobulin G, and broad-spectrum antibiotics, and he was ultimately discharged home on oral steroids and aspirin, with resolution of the rash confirmed at outpatient follow-up 3 days later.
- Figure 2
A previously healthy 2-year-old girl was admitted with concern for multisystem inflammatory syndrome in children after 5 days of fever, and vomiting, as well as palmar erythema, (seen in photo) a blanchable erythematous rash, conjunctival injection, periorbital edema, and lip erythema with desquamation and fissuring. Results of laboratory testing were notable for an elevated erythrocyte sedimentation rate of 36 mm/hr, a highly elevated C-reactive protein of 26.9 mg/dL, and COVID-19 immunoglobulin G antibody positivity. Because of cardiopulmonary deterioration during intravenous immunoglobulin G infusion, she was transferred to the intensive care unit and started on steroids, diuretics, antithrombotics, and anakinra, with improvement and eventual discharge after a 13-day hospitalization.
- Figure 3
A 74-year-old man, fully vaccinated against COVID-19 and with a remote history of cutaneous leukocytoclastic vasculitis, was seen in the emergency room after developing new purpuric patches, plaques, and bullae (A) on the face, oral mucosa, trunk, and (B) extremities. Testing confirmed acute breakthrough COVID-19 infection, and skin biopsy results were consistent with immunoglobulin A vasculitis. Hospitalization for intravenous steroids and supportive care was complicated by methicillin-resistant Staphylococcus aureus bacteremia and poor food and fluid intake due to oral pain. He was discharged in stable condition after a 22-day hospital stay.
- Figure 4
A 40-year-old woman with no known dermatologic history developed a pruritic maculopapular rash on the trunk following hospitalization for COVID-19 infection. Her COVID-19 course was complicated by bilateral pneumonia requiring supplemental oxygen and treatment with remdesivir and dexamethasone. Her rash was managed with oral antihistamines.
- Figure 5
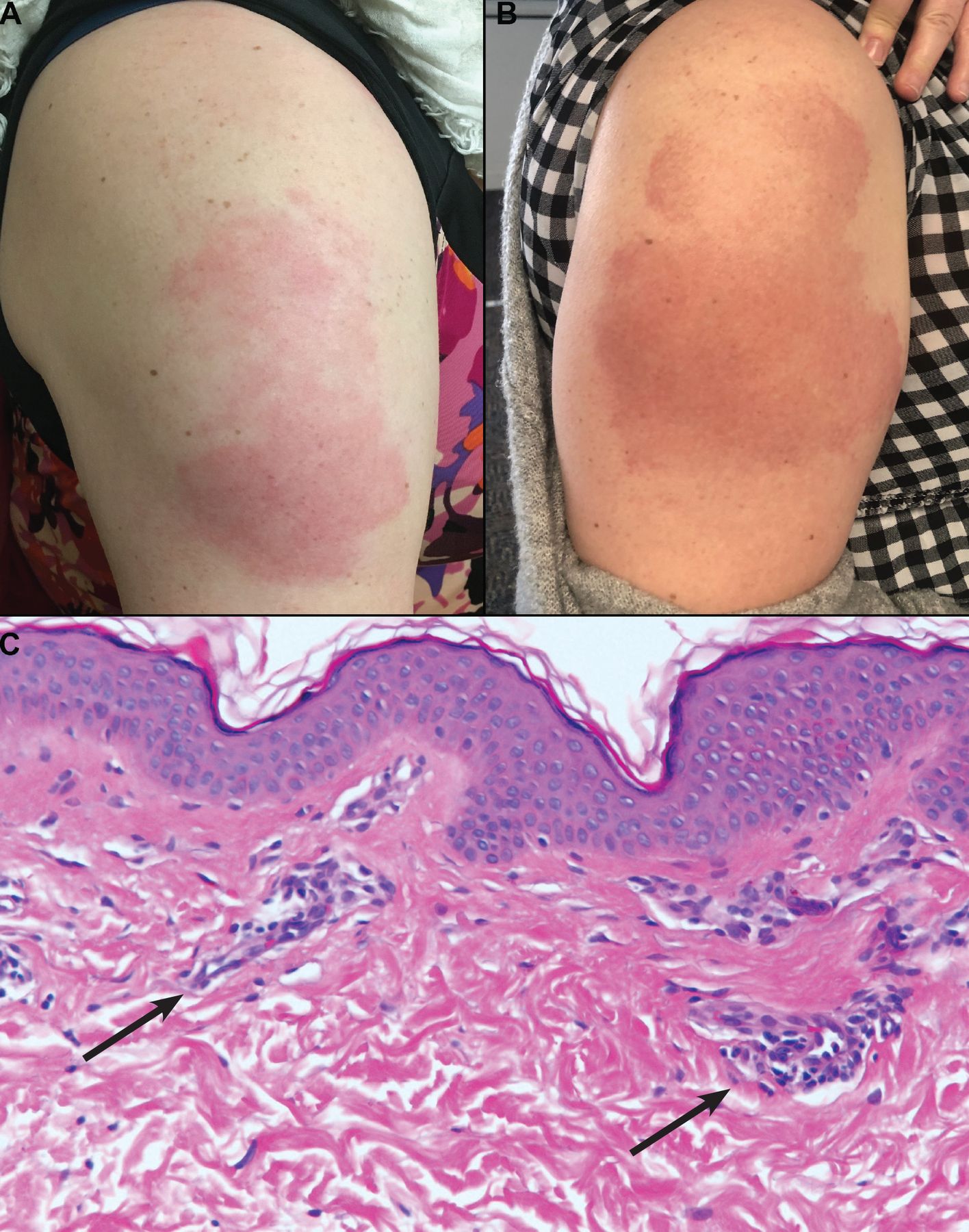
Eight days after her first dose of the Moderna messenger RNA vaccine, a 39-year-old woman developed a warm, confluent, (A) erythematous rash on her arm, characterized by a burning sensation. She also developed a pruritic, erythematous papular eruption on her chest, neck, and upper back 3 weeks after vaccination. Her primary care physician had treated her for presumed cellulitis with clindamycin without improvement. (B) The rash and associated symptoms began to improve by 23 days after vaccination. (C) Biopsy study of the lesions on her chest revealed a mild perivascular inflammatory infiltrate (arrows) consistent with a dermal hypersensitivity reaction. The patient deferred her second dose of Moderna vaccine due to concern for reaction recurrence. She eventually received the Johnson & Johnson COVID-19 vaccine at 10 months after the initial Moderna vaccine dose.
- Figure 6
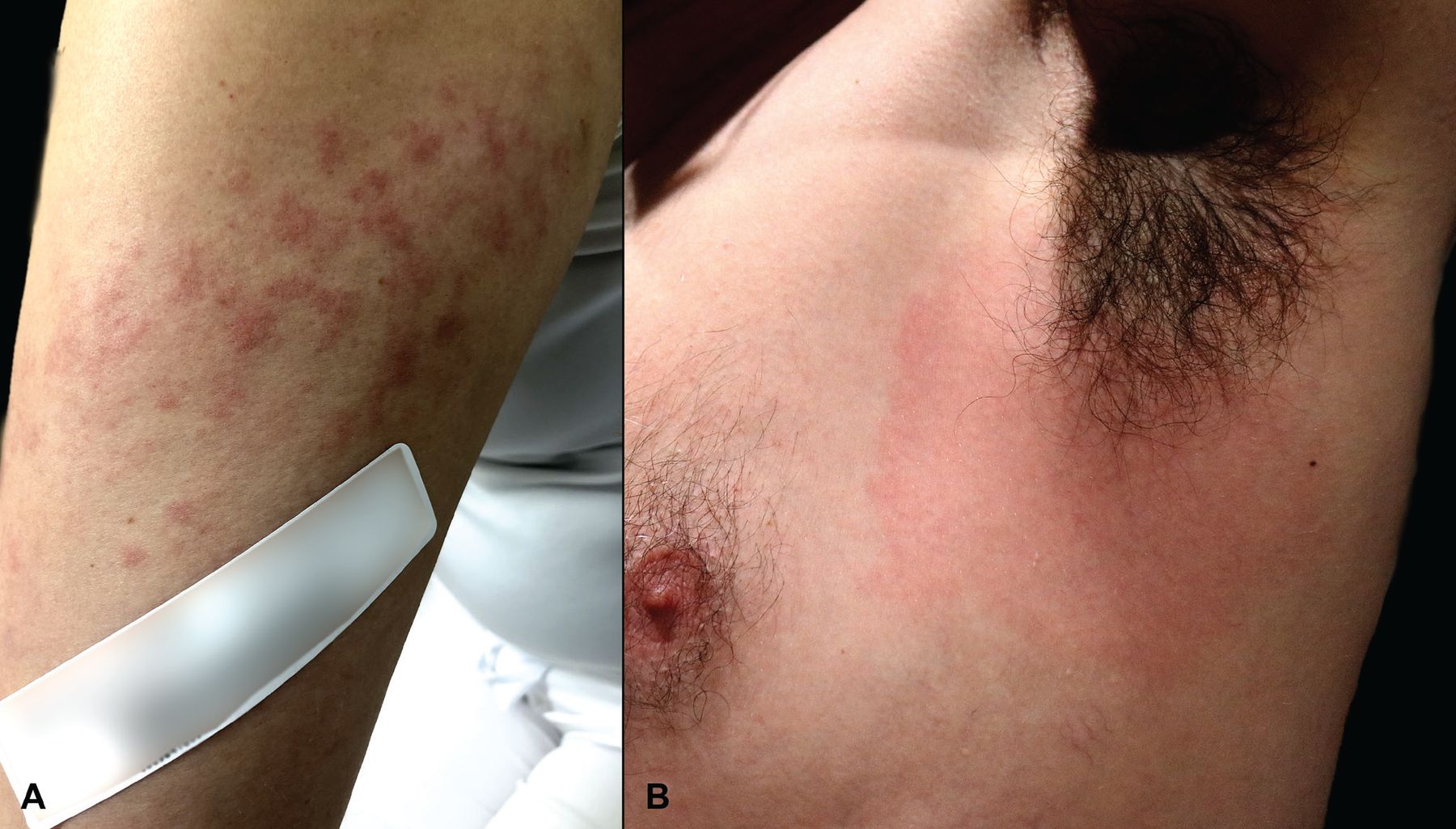
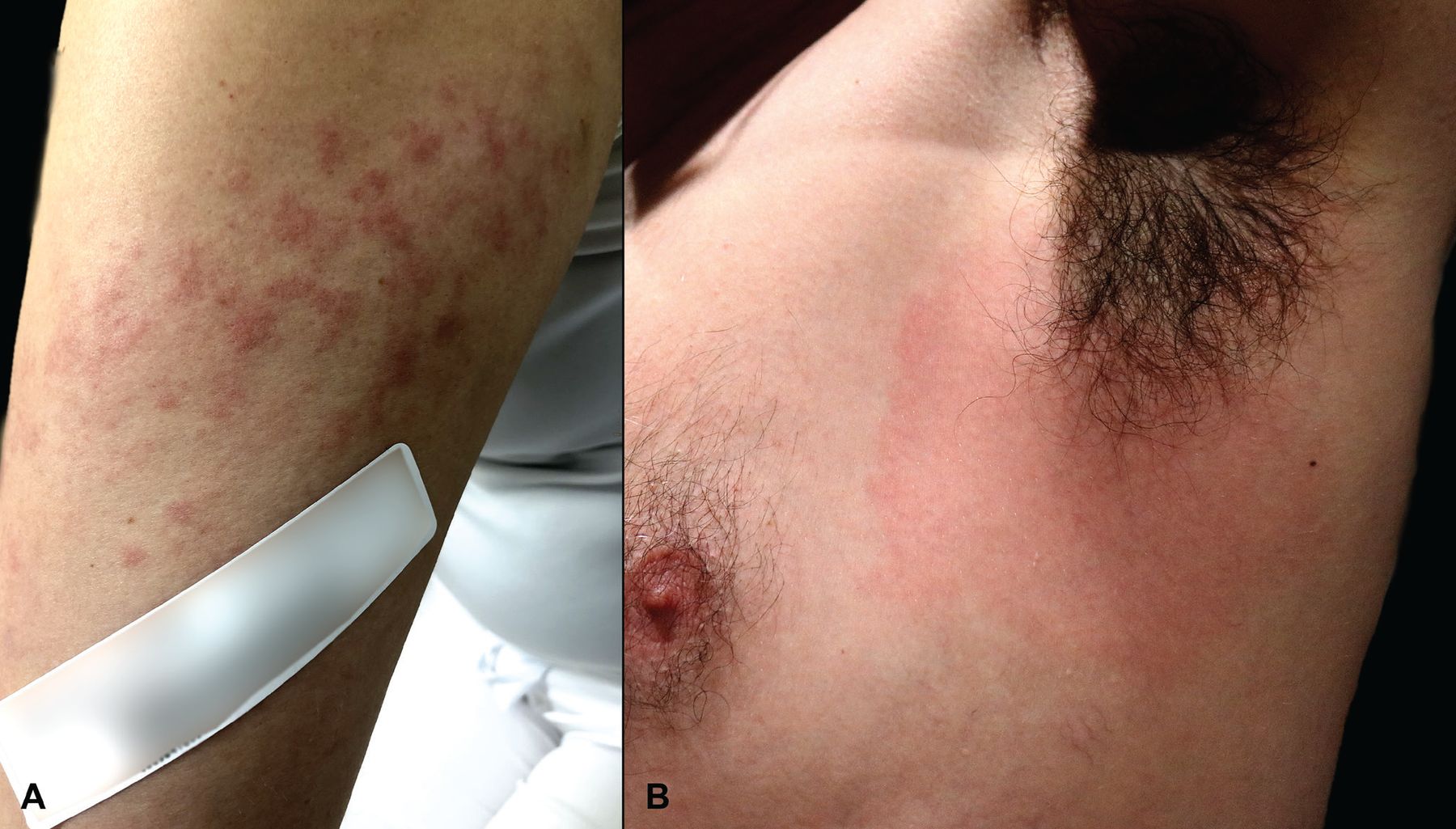
Uncharacteristic COVID-19 vaccine reactions near the injection site. (A) A 28-year-old woman developed a rash localized to the arm after her receiving her second dose of the Moderna vaccine. She developed multiple, ill-defined, erythematous macules and thin papules extending from the vaccination site in the deltoid area distally to the elbow 16 days after vaccination. Treatment with antihistamines, topical steroids, and a methylprednisolone dose pack brought resolution within 1 week. (B) A 51-year-old man developed confluent erythema with mild axillary tenderness and lymphadenopathy 48 hours after a third dose (ie, booster dose) of the Pfizer-BioNTech vaccine. He had experienced no cutaneous reactions after his first or second vaccine doses. His symptoms resolved within 2 days without treatment.
- Figure 7
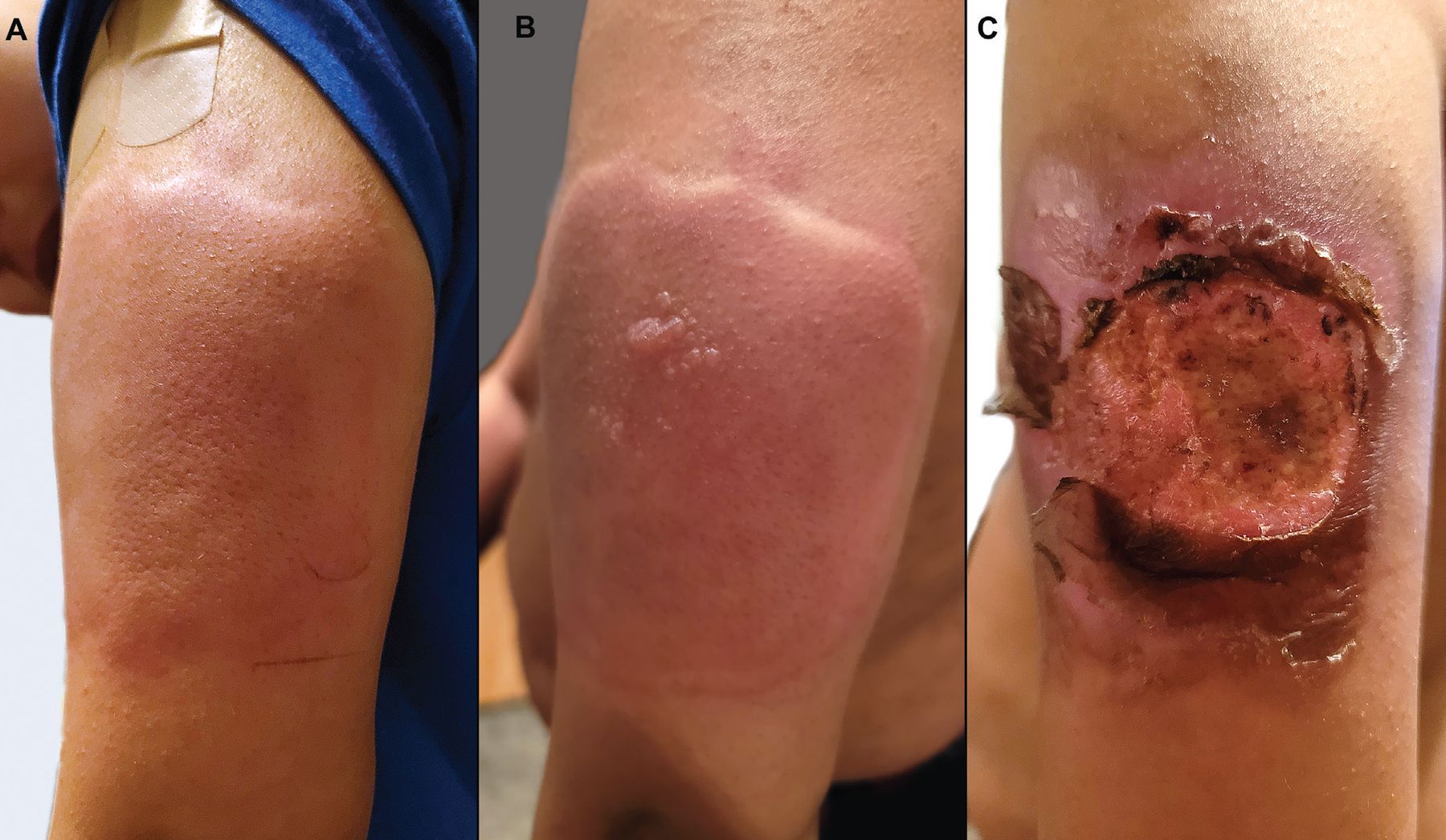
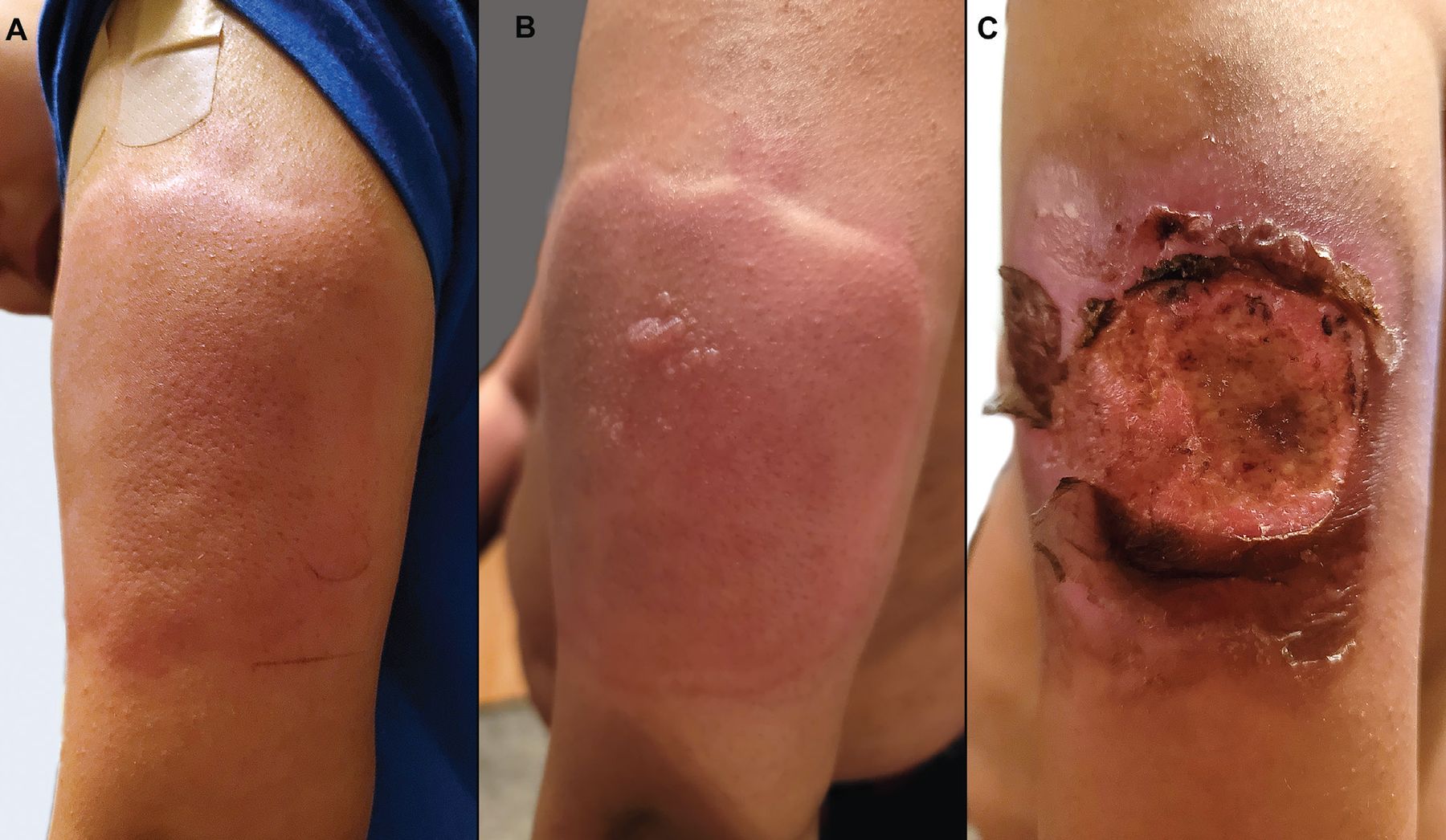
At a well visit with his pediatrician, an 11-year-old boy received 4 age-appropriate vaccines. In the right arm, he received the tetanus, diphtheria, and acellular pertussis vaccine and the meningitis vaccine. In the left arm, he received the Pfizer-BioNTech COVID-19 vaccine (12-year-old dose) and the human papillomavirus vaccine. Within minutes of receiving the vaccines, he developed a large, pruritic, erythematous and edematous plaque on his left arm (A), with subsequent vesiculation (B). Over the next 1 to 2 days, this progressed to a large, painful ulceration (C). He had no systemic symptoms with this reaction, and the lesions eventually healed.




Tables
- TABLE 1
Cutaneous reactions to COVID-19 vaccines in pediatric patients and non-White patients
Category Clinical presentation Timing Prognostic value Notes Multisystem inflammatory syndrome in children22 Kawasaki-like clinical presentation in pediatric patients22 Majority developed fever prior or concurrently with mucocutaneous findings22 Cutaneous findings not correlated with more severe clinical course22 Patients tend to be older and have more gastrointestinal symptoms than in Kawasaki disease22 Non-White patients17–21,23,24 Small reports of decreased rates of specific COVID-19 skin findings23,24
Scalp involvement and telogen effluvium may be more common17–20Hyperpigmentation may provide insight into previous inflammatory process21 No definitive data comparing outcomes based on cutaneous findings Palpation can be identify cutaneous eruptions when erythema is subtle21 Messenger RNA COVID-19 vaccines9,12,25–28 Acute and delayed local reactions most commonly seen, followed by urticarial and morbilliform eruptions9 Median time to onset after first dose was 7 days, occurring in 2 clusters between day 1–3 and day 7–89
Shorter median time from second dose, occurring at day 19Burgeoning data suggest local reactions not strongly associated with immunogenicity25–28 Many non-local reactions mimic the skin findings seen in COVID-19 infection12 Adenoviral vector COVID-19 vaccines29–32 Overall, rare dermatologic adverse events include urticaria and local reactions29 Majority of local dermatologic events were transient with a median duration of 2–3 days29 Associated petechiae may suggest a rare but life-threatening thrombotic reaction30,31 Rare case reports of unusual reactions including generalized Sweet syndrome, leukocytoclastic vasculitis, and a widespread pustular eruption32
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.