


A 36-year-old female presented to the emergency department following foreign body ingestion. Thirty minutes before arrival to the emergency department, while fitting her husband’s clothing, she had accidentally swallowed a tailor’s pin (Figure 1).

Example of a tailor’s pin.
Presenting symptoms included a mild sore throat and nonradiating abdominal pain described as “soreness” and “pressure” located left of the umbilicus. She denied fever, chills, cough, wheezing, shortness of breath, choking sensation, chest pain, nausea, vomiting, hematemesis, coffee-ground emesis, hematochezia, melena, inability to swallow saliva, dysphagia, regurgitation, diarrhea, or constipation.
The patient’s medical history was insignificant with no surgical or noteworthy family history. She noted occasional use of alcohol and no use of tobacco, illicit drugs, anticoagulants, antiplatelets, or nonsteroidal anti-inflammatory drugs. She lived in a house with her husband and worked as a chemist. At initial presentation, her vital signs included the following:
Blood pressure 143/89 mm Hg
Pulse 71 beats per minute
Temperature 97.9°F (36.6°C)
Respiratory rate 16 breaths per minute
Oxygen saturation 99% on room air
Body mass index 26 kg/m2.
On physical examination, the patient was alert and oriented to person, place, and time, looked comfortable, and was not in acute distress. There were no obvious signs of bleeding from the mouth or upper airway, no scleral icterus. Her lungs were clear to auscultation, she had a regular heart rate and rhythm without murmurs, rubs, or gallops, and no crepitus on palpation of neck and chest. Her abdominal exam was soft, nontender, nondistended, without guarding or rebound tenderness, and exhibited positive bowel sounds.
Initial laboratory results were all within normal limits, including complete blood cell count, comprehensive metabolic panel, and liver enzyme tests.
NEXT STEPS: IMAGING
1. What radiologic test would you obtain next?
Computed tomography (CT)
Barium esophagography
Magnetic resonance imaging of abdomen
Abdominal radiography
Foreign body ingestion is common among pediatric and adult populations, more frequent in the former, and foreign bodies can further be categorized as food and nonfood.1 Nonfood foreign body ingestion, a true foreign body ingestion, is more commonly seen in incarcerated adults and adults with psychiatric comorbidities.1–4 Although there are multiple radiologic tests for providers to order, biplane radiographic imaging is the preferred choice following foreign body ingestion.1,4
Abdominal radiographic imaging can confirm presence of the foreign body as well as the location, size, and shape of the object and is standard practice for management of foreign bodies based on American Society for Gastrointestinal Endoscopy guidelines.1 Furthermore, both chest and abdominal radiography are used to evaluate for foreign body aspiration and signs of free air that suggest perforation.1 This is important because insufflation of air into the upper gastrointestinal tract via endoscopy can increase perforation size and delay life-saving surgery.
Nonetheless, radiographic imaging does have limitations. Certain animal bones may not be visualized on radiography, such as fish or chicken bones. Furthermore, radiolucent materials such as plastic, glass, wood, and thin radiopaque metals may not be visualized. Although CT could assess foreign bodies, it is expensive and may not locate the aforementioned, radiolucent materials.1 If indicated, three-dimensional reconstruction could be used to improve detection; however, radiographic imaging should be used first.5 Any imaging that uses contrast, such as barium esophagogram, should not be performed as it may increase the risk of aspiration and decrease visualization of the foreign body during endoscopy.1 Lastly, magnetic resonance imaging is not recommended in this patient owing to the ingestion of a metal foreign body. Therefore, abdominal radiography is the imaging test of choice in this patient.
Findings on imaging
Ninety minutes after ingestion, initial biplane chest radiography did not identify a foreign body or signs concerning for perforation, such as free air or mediastinal air. Her abdominal radiography 2 hours after ingestion showed a foreign body measuring 18 mm in the left upper quadrant, likely in the stomach. No free air was noted, and shortly thereafter, 3 hours after ingestion, the gastroenterology team was consulted for further evaluation.
NEXT STEPS: TREATMENT
2. What is the most appropriate endoscopic timing for the ingested foreign body in this patient?
Emergent endoscopy
Urgent endoscopy
Nonurgent endoscopy
Monitor clinically
Endoscopy is commonly performed in foreign body ingestion.1,6 However, depending on the age and clinical condition of the patient and type of foreign object ingested, endoscopy timing may be emergent, urgent, or nonurgent1 with different endoscopic tools used to help retrieve the foreign body including forceps, nets, and snares.1,6
Emergent endoscopy is defined as immediate, within 6 hours of ingestion, and is indicated for complete esophageal obstruction, disk batteries in the esophagus, or sharp-pointed objects in the esophagus.1,7,8 Emergent endoscopy is especially important for complete esophageal obstruction owing to risk of aspiration from the inability to manage secretions and chest discomfort.7–10 Disk batteries are critical to remove owing to potential risk of liquefactive necrosis increasing the risk of esophageal perforation.1,11 It is important to retrieve button batteries as soon as possible, as they are considered an emergency in the pediatric population and an urgent case in the adult population.1 Lastly, sharp-pointed objects include animal bones (such as fish), dental bridgework, and needles, and when found in the esophagus, increase the risk of esophageal perforation, thereby indicating emergent endoscopy.8,12
Urgent endoscopy is defined as taking place within 24 hours of ingestion. It is indicated for esophageal food impaction without complete obstruction, esophageal foreign objects that are not sharp-pointed, sharp-pointed objects in the stomach or duodenum, objects greater than 6 cm in length at or above the proximal duodenum, and magnets within endoscopic reach.1 Because incomplete obstruction of esophageal food impaction has a decreased risk of aspiration compared with complete obstruction, endoscopy can be deferred for 24 hours. Furthermore, esophageal foreign objects that are not sharp-pointed can also be deferred up to 24 hours.1 Sharp-pointed objects in the stomach and duodenum must be endoscopically retrieved within 24 hours as the narrow lumen and fixed position of the duodenum makes maneuvering more difficult.1,13
Nonurgent endoscopy typically occurs within 48 hours and is most appropriate for foreign objects such as coins in the esophagus, objects in the stomach with a diameter greater than 2.5 cm, and disk and cylindrical batteries that are in the stomach of patients without signs of gastrointestinal injury.1 Coins in the esophagus can be observed for 12 to 24 hours before endoscopic removal in asymptomatic patients. If symptomatic, endoscopic removal is recommended.1,14 Foreign objects in the stomach that are greater than 2.5 cm in diameter are recommended to be removed within 24 hours because the chance of passage across the pylorus is less likely when the diameter is more than 2.5 cm.1,13,14 Lastly, disk and cylindrical batteries in the stomach without signs of gastrointestinal injury can be observed for up to 48 hours before endoscopic removal. Once the battery passes the duodenum, 85% pass through the body within 3 days. An abdominal radiograph is recommended every 3 to 4 days to assess progression through the body.1
Conservative management is appropriate in asymptomatic patients with gastric foreign objects that do not meet the emergent, urgent, or nonurgent criteria.1 Because such foreign bodies can take up to 4 weeks to pass, these patients can resume their regular diet, monitor their stool for foreign body passage, and obtain weekly abdominal radiographic imaging.1 If a foreign body distal to the duodenum does not migrate after 1 week and can be retrieved endoscopically, endoscopic removal is recommended. If the foreign body cannot be removed endoscopically, surgical consultation is recommended.1,13
Lastly, magnets within endoscopic reach should be retrieved within 24 hours because magnets that trap bowel tissue between another magnet or metal foreign body can cause pressure and bowel wall necrosis increasing the risk of obstruction, fistula formation, and perforation.1,15 If the magnet cannot be endoscopically reached, close monitoring and surgical consultation is recommended if the magnet fails to migrate.1
CASE CONTINUED
Because our patient had a sharp-pointed object observed in the left upper quadrant of the abdominal radiograph, suggesting the tailor’s pin was in the stomach, the most appropriate next step in management was urgent endoscopy. About 5 hours after ingestion, gastroenterology clinicians performed an upper endoscopy using a flexible adult esophagogastroduodenoscopy scope with no sign of the tailor’s pin up to the third portion of the duodenum. Consequently, the esophagogastroduodenoscope was exchanged for a flexible pediatric colonoscope to perform a push enteroscopy in efforts to locate the pin. Unfortunately, no pin was found up to the proximal jejunum.
3. What is the next best step in management?
Proceed with colonoscopy
Computed tomography
Consult surgery
Serial abdominal radiography
Capsule endoscopy
If a sharp-pointed foreign body cannot be retrieved endoscopically, daily radiographs should be performed to track the migration through the gastrointestinal tract.1,4,13 Laxatives may expedite passage through the gastrointestinal tract and can be used to decrease transit time if initial endoscopy is unsuccessful.1 If a sharp-pointed object fails to progress in 3 days, surgical consultation is recommended.13
While sharp-pointed objects that enter the stomach often pass through the remainder of the gastrointestinal tract, complications can occur.1 Indications for immediate surgical intervention include development of complications such as obstruction or perforation.
Lastly, although CT can locate the foreign body, abdominal radiography can also do this, although abdominal radiography is less expensive and exposes the patient to less radiation.
ENTEROSCOPY: EXAMINATION OF THE SMALL INTESTINE
There are multiple endoscopic techniques that can be used to examine the small intestines and retrieve foreign bodies.16 Upper endoscopes commonly used in esophagogastroduodenoscopy are first used to retrieve foreign bodies in the esophagus, stomach, and duodenum. Although some upper endoscopes can reach the jejunum, this rarely occurs. Therefore, the upper endoscope is exchanged for a colonoscope, which is longer, wider, and stiffer and is passed orally and pushed to its maximum distance (“push enteroscopy”).
Pediatric colonoscopes can reach 45 to 60 cm from the ligament of Treitz, whereas dedicated enteroscopes can reach 25 to 80 cm from the ligament of Treitz.16 However, the colonoscope and endoscope are used to advance as far as possible until looping limits the ability to progress. Therefore, device-assisted enteroscopy, including single- and double-balloon enteroscopy and spiral enteroscopy, was designed to improve reach into the small intestine by pleating the small bowel while propelling the scope for greater insertion depth as the balloon expands. The scope can be passed anterograde via the mouth to reach the ileum, or retrograde via the rectum to reach the ileum.
In contrast to balloon-assisted enteroscopy, spiral enteroscopy, a simpler and faster technique, does not use a balloon; it is designed to pleat the small intestine by spiraling clockwise with its spiral ridged overtube.16
Single-balloon enteroscopy can reach 133 to 270 cm for anterograde and 73 to 199 cm for retrograde examination, double-balloon enteroscopy can reach 220 to 360 cm anterograde and 124 to 183 cm retrograde, and spiral enteroscopy can reach 175 to 262 cm anterograde.16
A new balloon-assisted device that allows “on-demand” enteroscopy involves passing a balloon through the endoscope or colonoscope working channel.16 As in balloon enteroscopy, it also helps pleat the small intestine shorter by anchoring the balloon to the small intestine and pulling the scope toward the balloon distally. It can reach 120 to 190 cm anterograde and 89 to 110 cm retrograde. Device-assisted enteroscopy is more expensive than push enteroscopy.
Lastly, intraoperative enteroscopy can be considered. Intraoperative enteroscopy is performed in the operating room with a surgical team.16 After obtaining access via laparoscopy or laparotomy, the surgeon pleats segments of the intestine while pushing the enteroscope into the small intestine. However, this is the most invasive technique available. Intraoperative enteroscopy can reach up to the ileocecal valve.
Foreign bodies in the colon and terminal ileum may be retrieved using either adult or pediatric colonoscopes in a retrograde approach.16,17 However, these colonoscopes can only reach a few centimeters into the terminal ileum. Therefore, single- and double-balloon enteroscopes can be inserted retrograde to assess the ileum.
CASE CONTINUED
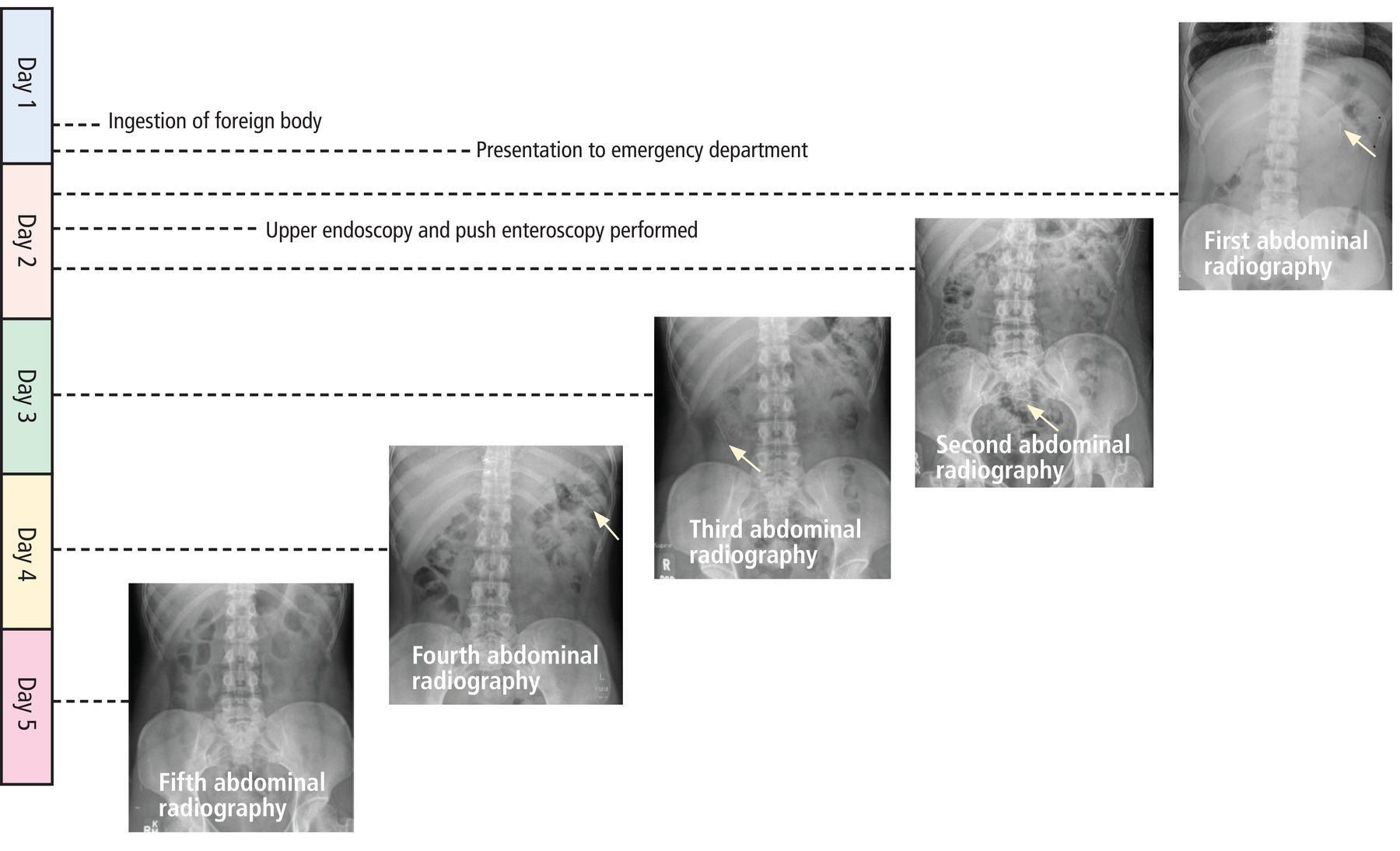
Colonoscopy and capsule endoscopy were not appropriate for our patient as she did not complete bowel preparation, and the exact location of the foreign body was not specifically known. Because endoscopic retrieval failed and the object was presumed to have already passed distal to the proximal jejunum, and because the patient did not have complaints indicating obstruction or perforation, the decision was made to manage conservatively with daily serial outpatient abdominal radiography for 3 days (Figure 2). It was determined that if the object did not pass after 3 days or if she developed acute symptoms such as increased abdominal pain, nausea, or fever concerning for obstruction or perforation, hospital admission and CT scan of her abdomen and pelvis would be performed with immediate surgical consultation. She was advised to return to the emergency department immediately if any of the concerning symptoms occurred.

Timeline of foreign body ingestion, endoscopy, and abdominal radiography.
About 18 hours after ingestion, she underwent repeat abdominal radiography following endoscopy that had taken place earlier in the morning. The foreign body was visualized over the superior pelvis. Shortly after the radiology report, the patient was called to provide an update as well as assess for any symptoms. She denied any pain and felt well.
About 42 hours after ingestion, she completed her third abdominal radiography following endoscopy. The foreign body now appeared over the right upper quadrant. Again, the patient was called to review radiography results and to assess for any symptoms. She denied abdominal pain, fever, chills, sweats, hematochezia, or melena stool. She endorsed 3 soft bowel movements that same day as well as some bilateral rib soreness, but otherwise noted no complaints.
About 66 hours after ingestion, she completed additional abdominal radiography showing that the tailor’s pin was located in the left upper quadrant. She again reported no symptoms. Although the guidelines recommend surgical consultation for retained sharp-pointed foreign object after 3 days of observation and the patient failed to pass the tailor’s pin on day 4, it was decided to observe for 1 more day and add a laxative to help expedite foreign body passage as the patient was asymptomatic and the foreign body was advancing every day. She was prescribed 2 L of polyethylene glycol to help expulse the foreign body.
About 90 hours after ingestion, the patient reported passing the pin. She received confirmatory abdominal radiography reporting no foreign body.
CASE MANAGEMENT
Urgent endoscopic management within 24 hours is indicated for ingested sharp-pointed foreign bodies that appear to be in the stomach or duodenum at presentation.1 However, if endoscopy can be performed within 4 hours of foreign body ingestion, endoscopy is also recommended as expedited foreign body removal avoids admissions, repeat radiography, and potential complications. If endoscopic retrieval of the foreign body fails, conservative management with serial abdominal radiography for 3 days is appropriate, and supplementation with bowel preparation can be offered to assist passage of the foreign body.1,13 If a sharp-pointed foreign body fails to progress within the aforementioned timeframe or if the patient develops symptoms of perforation, then CT with surgical consultation is recommended. In this case, the decision to proceed with endoscopic evaluation early was made to increase the chance of foreign body retrieval within the proximal gastrointestinal tract.
TAKE-HOME POINTS
Complications of foreign body ingestion may be severe and include perforation, obstruction, and aortoesophageal fistula and tracheoesophageal fistula formation.10,15
Timing of endoscopy for ingested foreign objects is dependent on the clinical condition of the patient; the size, shape, content, and anatomic location of the ingested object; and the time since ingestion.1 Based on these details, the patient may qualify for emergent, urgent, or nonurgent endoscopy, or expectant management.
If endoscopic retrieval of a sharp-pointed foreign body fails, conservative management may be appropriate with daily abdominal radiography for 3 days.13
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2023 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.