


Article Figures & Data
Figures
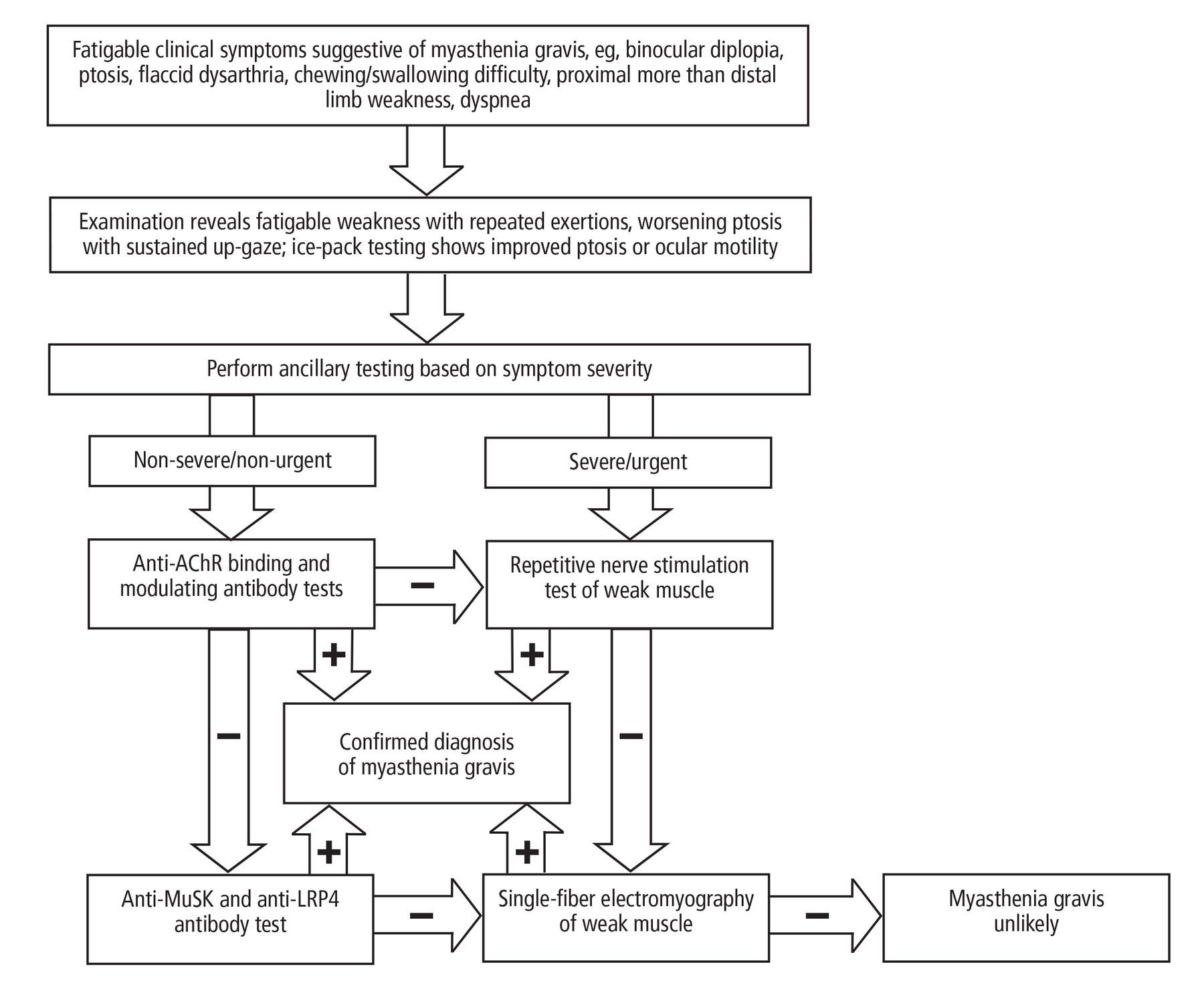
- Figure 1
Diagnostic algorithm for myasthenia gravis. If the anti-AChR binding and modulating antibody tests are negative, two options are reasonable, as indicated.
AChR = acetylcholine receptor; LRP4 = lipoprotein-related protein 4; MuSK = muscle-specific tyrosine kinase

Tables
Disorder Similarities to myasthenia gravis Differences from myasthenia gravis Lambert-Eaton myasthenic syndrome Weakness and fatigue Less prominent ocular or oculobulbar features
Areflexia or hyporeflexia
Autonomic features (dry mouth, erectile dysfunction)
Positive antibody against P/Q voltage-gated calcium channel
High-frequencey repetitive nerve stimulation testing shows an incremental response (ie, a progressive increase in motor amplitude)Botulism Ocular findings (diplopia and ptosis), bulbar dysfunction, generalized weakness Acute attack, possible history of food poisoning
Descending paralysis
Dilation of the pupil (mydriasis)
Prominent autonomic dysfunction
Monophasic course
High-frequency repetitive nerve stimulation testing shows an incremental responseAmyotrophic lateral sclerosis Bulbar dysfunction and weakness Slow progressive course
No ocular findings
Symptoms do not fluctuate
Findings of upper motor neuron dysfunction (eg, hyperreflexia, spasticity)
Electromyography showing prominent active and chronic denervation or reinnervation, or bothMyopathy Proximal limb weakness Relative absence of ocular findings
Symptoms do not fluctuate
Creatine kinase elevation and presence of myositis-specific antibodies in cases of autoimmune or inflammatory myositis
Repetitive nerve stimulation testing is normal, while needle electromyography shows short-duration, low-amplitude, polyphasic motor-unit potentials, with or without abnormal spontaneous activityGuillain-Barré syndrome and chronic inflammatory demyelinating polyradiculoneuropathy Generalized weakness Sensory symptoms such as pain and paresthesia
Symptoms do not fluctuate
Hyporeflexia or areflexia
Cerebrospinal fluid has protein elevation, no significant pleocytosis
Nerve conduction studies reveal findings consistent with demyelinationThyroid eye disease Diplopia Ptosis is infrequent
Symptoms do not fluctuate
Other ocular findings such as edema, redness, conjunctival injection and exophthalmos
Magnetic resonance imaging showing extraocular tissue enlargementOculopharyngeal muscular dystrophy Ptosis, diplopia, dysphagia Slowly progressive course
Absence of symptomatic fluctuation
Relative absence of prominent limb weakness
Elevation of creatine kinase
Mutations in the PABPN1 gene; mostly autosomal dominant pattern of inheritanceComplement inhibitor Zilucoplan Neonatal Fc receptor inhibitors Batoclimab Nipocalimab Rozanolixizumab B-lymphocyte depletion therapy Obinutuzumab Ofatumumab Ublituximab Blinatumomab Inebilizumab Cytokine inhibitor Tocilizumab Janus kinase inhibitors Ruxolitinib Baricitinib Tofacitinib Hematopoietic stem cell transplantation Chimeric antigen receptor T-cell therapy
In this issue




{kind=link}
Jump to section
- Article
- ABSTRACT
- WHICH POPULATIONS ARE AT RISK?
- WHEN SHOULD A CLINICIAN THINK ABOUT THIS DIAGNOSIS?
- WHAT TESTS SHOULD BE ORDERED?
- HOW DOES THE NATURAL COURSE AFFECT THE TREATMENT STRATEGY?
- WHAT INSTRUCTIONS SHOULD PATIENTS RECEIVE?
- WHICH MEDICATIONS ARE BEST AVOIDED?
- HOW SHOULD PYRIDOSTIGMINE BE USED?
- WHEN SHOULD CORTICOSTEROIDS BE USED?
- WHEN SHOULD OTHER IMMUNOSUPPRESSIVES BE USED?
- WHAT IS THE ROLE OF THE THYMUS? WHO SHOULD UNDERGO THYMECTOMY?
- HOW CAN MYASTHENIC CRISIS BE PREVENTED, RECOGNIZED, AND TREATED?
- WHAT NEW TREATMENTS ARE ON THE HORIZON?
- DISCLOSURES
- REFERENCES
- Figures & Data
- Info & Metrics