


Article Figures & Data
Figures
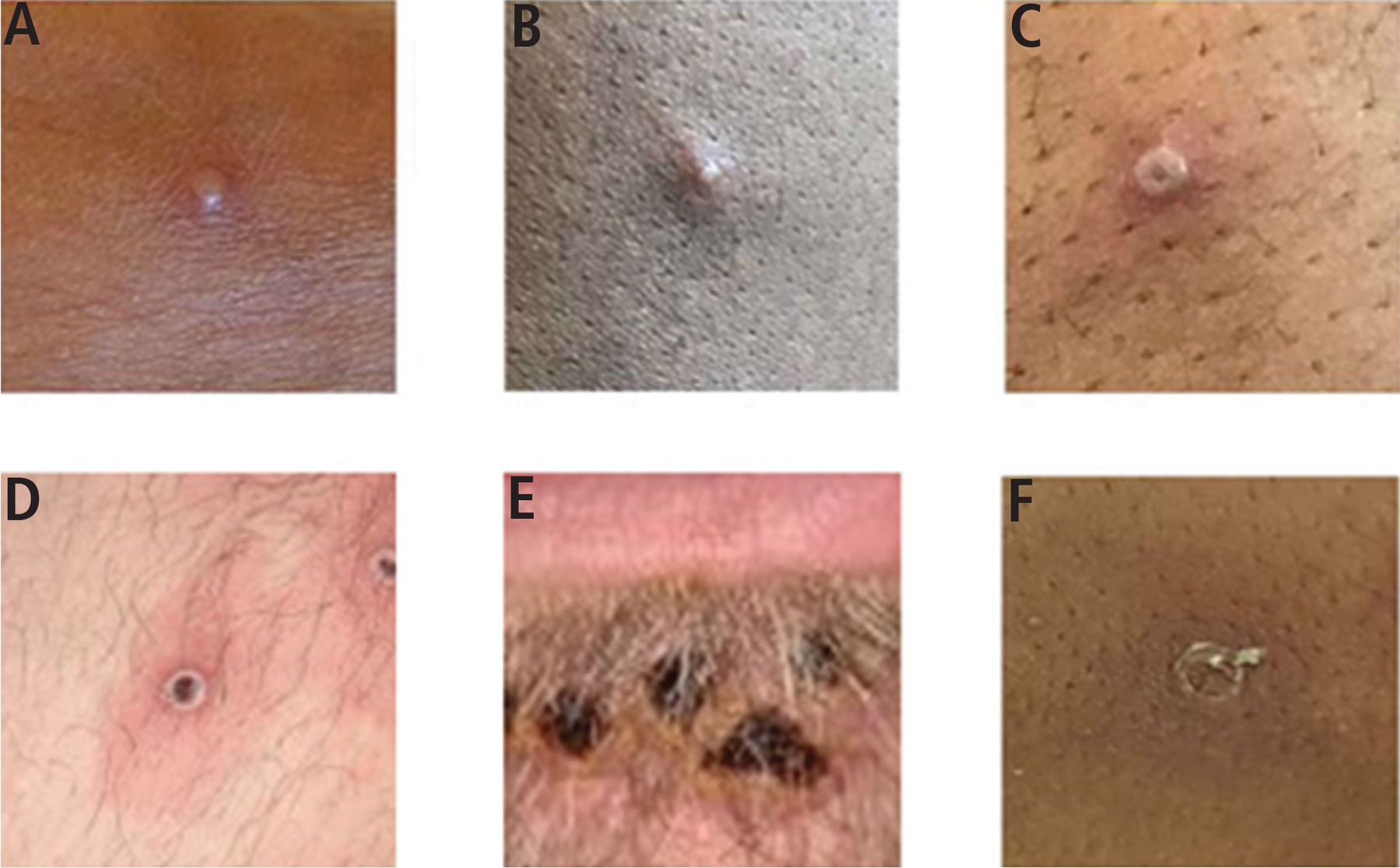
- Figure 1
Mpox lesions in various stages of development: (A) early vesicle, (B) small pustule, (C) umbilicated pustule, (D) ulcerated lesion, (E) crusted mature lesions under the lower lip, and (F) partially removed scab.
Adapted from reference 15.
- Figure 2
Sites of mpox lesions in an observational cohort study in southern France. (A) Primary inoculation site showing an irregular pustule with necrotic crust of the right nipple. (B) Pustular lesions with a crusted center on the mucosa of the upper lip, close to the left oral commissure and left nasal orifice. (C) Pustules circumferentially distributed on the anal margin and perianal skin of varying sizes and stages of evolution, some with central necrotic crusts. (D) Perineally extended purpuric lesions. (E) Scrotal lesions of varying sizes and stages of evolution, with edema surrounding the larger ulcero-hemorrhagic ulcers. (F) Scattered papules, pustules, and umbilicated pustules surrounded by an erythematous halo on the back. (G) Reddened and swollen right palatine tonsil with a fibrin-covered ulcer. (H) Pustular lesion on the nose with a necrotic central crust, whitish deposit, and erythematous halo.
Adapted from reference 16.


Tables
- TABLE 1
Our recommended screening for sexually transmitted infections in patients with mpox
Sample site Screening Blood HIV-1/HIV-2 antigen-antibody immunoassay (screening test) a
Nontreponemal test (eg, rapid plasma reagin), reflexively followed by treponemal test, if positive
Hepatitis C antibody b
Hepatitis B surface antibody, surface antigen, and core antibody cUrine Gonorrhea and chlamydia nucleic acid amplification test Rectum
(if patient participates in receptive anal intercourse or has rectal symptoms)Gonorrhea and chlamydia nucleic acid amplification test Oropharynx
(if patient participates in oral intercourse or has oropharyngeal symptoms)Gonorrhea and chlamydia nucleic acid amplification test Vagina, cervix
(if patient participates in vaginal intercourse or has vaginal symptoms)Gonorrhea and chlamydia nucleic acid amplification test Lesion
(when clinically unable to differentiate between mpox and herpesvirus)HSV-1 and HSV-2 polymerase chain reaction test
Varicella virus polymerase chain reaction testNot recommended Serologic testing for HSV-1 and HSV-2 antibodies (does not distinguish current from previous infection)
Serologic HSV or varicella virus polymerase chain reaction test (insensitive and nonspecific for dermatologic infection)↵a HIV-1/HIV-2 antigen-antibody immunoassay will detect HIV about 17 days after HIV acquisition. For patients with a potential exposure < 17 days and concern for acute retroviral syndrome, send for HIV nucleic acid amplification testing (viral load). Caution in patients on preexposure prophylaxis, which can result in delayed seroconversion and indeterminate results on HIV differentiation assay.
↵b Sexually active men who have sex with men should undergo hepatitis C virus screening at least annually.
↵c Men who have sex with men without serologic evidence of immunity to hepatitis B should undergo vaccination.
HIV = human immunodeficiency virus; HSV = herpes simplex virus
Severe disease
Hemorrhagic disease
Confluent lesions
Organ involvement (central nervous system, lungs, eyes)At risk for severe disease
Extremes of age
History of dermatologic condition, including atopic dermatitis
Pregnant or breastfeeding
Secondary bacterial infection
Dehydration
ImmunocompromisedHigh-risk sites of infection
Oropharyngeal lesions
Anogenital lesionsDosing of oral tecovirimat Patient weight 40 to < 120 kg: 600 mg every 12 hours
Patient weight ≥ 120 kg: 600 mg every 8 hoursPatient counseling Tecovirimat is generally well-tolerated
The most frequently reported side effects are headache, nausea, and abdominal pain
Tecovirimat must be administered with a full meal with high fat content (ideally 600 calories and 25 g of fat)a
For patients who cannot swallow capsules, the capsules may be opened and the entire contents mixed with 30 mL of liquid or soft food↵a If the patient cannot consume a high-fat meal, providers should consider using the intravenous formulation to ensure adequate drug levels are achieved.
Any person who has had anal or vaginal sex in the past 6 months with: A partner who is HIV-positive with unknown or detectable viral load
One or more partners of unknown HIV status and inconsistent condom use
Any bacterial sexually transmitted infection (chlamydia, gonorrhea, syphilis) in the past 6 monthsa
People who inject drugs and share injection equipment Any individual who does not meet the above criteria, but requests preexposure prophylaxis ↵a CDC guidelines note that this does not include chlamydia in women who have sex with men and men who have sex with women, but local HIV incidence should be taken into consideration.
HIV = human immunodeficiency virus
In this issue




{kind=link}
{kind=link}
Jump to section
- Article
- ABSTRACT
- RELATED TO SMALLPOX
- SHIFTING EPIDEMIOLOGY
- THE CLINICAL PRESENTATION HAS CHANGED
- DIFFERENTIAL DIAGNOSIS
- TESTING FOR MPOX
- MANAGEMENT
- INFECTION CONTROL IN HEALTHCARE SETTINGS
- INFECTION CONTROL AT HOME
- HIV PROPHYLAXIS
- VACCINIA VACCINATION
- CONDOMS ARE NOT EFFECTIVE PROTECTION AGAINST MPOX
- LESSONS LEARNED, LESSONS TO BE LEARNED
- DISCLOSURES
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics