


ABSTRACT
Access to and use of glycemic data are central to optimal management of diabetes. Use of continuous glucose monitoring (CGM) data to guide the management of diabetes has increased dramatically thanks to improved ease of use, accuracy, and availability. Retrospective CGM data collected throughout the day and night allow clinicians to visualize glycemic patterns, and single-page summary views like the Ambulatory Glucose Profile (AGP) Report make rapid interpretation both feasible and intuitive. A systematic approach that integrates retrospective CGM-generated data at clinic visits and other clinical interactions with personal use of CGM data can optimize glycemic management.
CGM is recommended for patients with type 1 diabetes and patients with type 2 diabetes treated with insulin.
The single-page AGP Report allows for rapid and intuitive interpretation of CGM data by displaying patterns of clinically relevant hypoglycemia, hyperglycemia, and glucose variability.
When reviewing the time-in-ranges bar, focus on increasing time in range to more than 70% and decreasing time below range to less than 4% to improve glycemia.
Focus also on lifestyle and medication changes that make the AGP curve more flat, narrow, and in-range.
Continuous glucose monitoring (CGM) technology, first developed in the early 2000s, has evolved to include devices with longer wear times that do not require calibration with fingerstick blood glucose monitoring, and with dramatically improved ease of use and availability.1 In parallel with the evolution in CGM technology, there has been a dramatic increase in clinical use of CGM, both in type 1 diabetes, where CGM has become standard of care, and in insulin-treated type 2 diabetes.2
OVERVIEW OF CGM DEVICES
Current-generation blood glucose monitoring relies on measurement from whole blood obtained by fingerstick, while CGM technology derives glucose values from interstitial fluid via a tiny electrode inserted beneath the skin. Because diffusion of glucose from blood into the interstitial compartment is slightly delayed, interstitial glucose values are processed mathematically to improve approximation and concordance with capillary glucose levels. Although device-related delays have been minimized in recent CGM devices, typically there is a 5- to 10-minute lag between interstitial and blood glucose levels,3 and this should be communicated to clinicians and patients.
CGM technology can be broadly divided into 2 categories: devices for personal use by patients to monitor glucose on an ongoing basis and professional devices, or clinic-owned devices used intermittently to evaluate glucose metrics and patterns at clinic visits and to guide counseling and management suggestions. Personal use has largely overshadowed professional use. Professional CGM remains useful for individuals for whom personal systems are either not needed or not available and in specialized research settings. Personal CGM remains the technology of choice for most users.
Personal CGM devices can be categorized as real-time devices that measure and display glucose values continuously while worn or intermittently scanned devices (Table 1). The latter are somewhat simpler devices that require the user to scan a sensor worn on the body to gather glucose data. Both types of CGM devices can collect 24-hour retrospective data for evaluating patterns and glycemic metrics, and both have utility in the management of type 1 and type 2 diabetes.
Currently available continuous glucose monitoring systems
EVIDENCE AND GUIDELINES ARE EVOLVING
Evidence from multiple randomized controlled trials supports the value of CGM in the management of diabetes, especially for patients who manage their diabetes with insulin.4–9 CGM improves both hemoglobin A1c and hypoglycemia relative to fingerstick blood glucose monitoring in type 1 diabetes.4,5 In patients with type 2 diabetes who use insulin, CGM improves hemoglobin A1c or decreases hypoglycemia to a greater degree than fingerstick blood glucose monitoring.6–9
Evidence-based guidelines created by specialty and advocacy groups have evolved based on this growing body of evidence. The 2024 American Diabetes Association Standards of Medical Care in Diabetes supports CGM for all individuals with diabetes on insulin therapy (Grade A recommendation for real-time CGM, Grade B recommendation for intermittently scanned CGM),2 while the American Association of Clinical Endocrinology strongly recommends CGM for all patients with diabetes using basal and bolus insulin (ie, treated with both background and mealtime bolus insulin [Grade A; high strength of evidence]) and for patients with type 2 diabetes treated with less intensive insulin regimens (basal insulin only [Grade B; intermediate strength of evidence]).10
THE POWER OF CGM: 2 TYPES OF DATA
Medical nutrition and noninsulin and insulin therapies directly target physiologic processes to improve glucose management; CGM improves care indirectly by facilitating changes in lifestyle or diet and improving medication adherence without any direct physiologic impact. The power of CGM is in the 2 types of data it provides.
Point-in-time data: A patient with diabetes can view, on demand, a point-in-time glucose value, a trend arrow indicating whether the glucose is rising or falling, and a profile of recent glucose levels that typically represents 8 hours of data. With point-in-time data patients can see the impact of diet choices, lifestyle choices, and medications at any time, which allows real-time physiologic feedback to directly guide management of diabetes day to day.
Retrospective data: CGM technology has the capability to collect and display thousands of glucose data points retrospectively as composite glucose metrics, and visually as composite and daily views for retrospective analysis.
Point-in-time and retrospective data support diabetes management in complementary ways. Retrospective data allow for shared decision-making and optimized evaluation of the safety and efficacy of glycemic management during clinical interactions. The power of retrospective CGM data lies not in the thousands of individual data points, but in composite summary reports. Just as electrocardiographic reports have evolved toward a standardized layout, presentation of CGM data has evolved toward the Ambulatory Glucose Profile (AGP), a standardized single-page summary report (Figure 1). Major CGM manufacturers use slight variations of the AGP Report to display data in a format that is familiar and accessible. While reports vary by manufacturer and device, AGP reports typically include the data elements described in this article.

Example of an Ambulatory Glucose Profile Report. (A) The time-in-ranges graph quickly shows whether glycemic goals are being met and whether action is needed. Average glucose and glucose management indicator metrics provide additional information about the need to take action. Glucose variability reports variations over the course of the report period. Increased variability is a risk factor for hypoglycemia. (B) The ambulatory glucose profile curve presents a 24-hour picture of all glucose readings collected during the report period. (C) Ambulatory daily glucose profiles are thumbnails of daily values.
©2024 International Diabetes Center, Minneapolis, MN. Used with permission. Visit AGPreport.org for more information.
There are several mechanisms for obtaining retrospective CGM and AGP data. CGM data from the sensor are sent to a reader or smartphone device either in real time or when the device is intermittently scanned. For intermittent scanning, the sensor should be scanned at least every 8 hours to capture all retrospective CGM data. Once transferred to a receiver or smartphone, the data can be uploaded from the device to an industry-based cloud data repository from which they can be easily viewed by the patient or, with permission (typically by an email invitation), remotely by the diabetes care team. All major CGM manufacturers have proprietary cloud-based repositories. If a clinician does not have access to a patient’s cloud-based data, it is feasible in clinical settings to view retrospective data on a smartphone or reader directly. Glycemic metrics and the AGP are typically available on these devices, although the format is slightly less accessible.
THE AMBULATORY GLUCOSE PROFILE: 3 STEPS
Because CGM technology can capture glycemic data of a 24-hour day-night cycle over several weeks, CGM-derived glycemic metrics and patterns displayed in an AGP Report provide a robust picture of glycemia on both a daily and time-averaged basis. Consensus panel guidance recommends at least 14 days of CGM data with a minimum of 70% sensor wear to generate an AGP Report that enables optimal analysis and decision-making.11 This recommendation is based on data suggesting a strong correlation between 14-day CGM metrics that measure time within recommended ranges and CGM metrics collected over longer periods of time.12,13 The more complete the data, the more reliable the CGM metrics will be. This can be especially important when counseling people using intermittently scanned CGM technology. More frequent scanning leads to more complete data collection, with better insights into day and night patterns, frequency of hypoglycemia, and variability in glucose levels throughout the day.
Central to optimal and efficient use of CGM data is a structured approach to its evaluation. To guide decision-making, we employ a 3-step evaluation process: Determine Where to Act.
Step 1: Determine whether action is needed
Time in ranges. The upper third of the AGP Report (Figure 1A) provides a summary of glycemic metrics. The time-in-ranges bar graph allows rapid determination of whether glycemic goals are being met and whether action is needed to improve glucose management. The time-in-ranges graph displays:
Percentage of time spent in prespecified glycemic ranges for the number of days included in the AGP Report—arguably the single most important measure in determining the need for action regarding the adequacy and safety of the patient’s glycemic regimen
Time above range, defined as the high range of 181 to 250 mg/dL and very high range greater than 250 mg/dL
Time-in-range target of 70 to 180 mg/dL
Time below range, in the low range of 69 to 54 mg/dL and clinically significant very low range below 54 mg/dL.
Comparison of time in range to consensus goals on the time-in-ranges graph permits the clinician or patient to decide quickly whether to act.
The patient represented in Figure 1 has not met any of the 5 time-in-ranges goals. Action is needed because the patient has too much time below range at 9% (goal < 4%) and too much time above range at 25% (goal < 25%). Optimized glycemic management should focus on increasing time in range (70–180 mg/dL) while minimizing time below range (< 70 mg/dL). Another approach is to focus on “more green” (more time in the target range of 70 to 180 mg/dL) and “less red” (less time with a glucose level below 70 mg/dL). This is also a patient-friendly way to communicate what the goal for CGM “time in ranges” is. Time in range and time below range can be thought of together as a composite measure reflecting the adequacy of glycemic management.14
The goals for time above range, time in range, and time below range were chosen by the International Consensus on Time in Range (Table 2).15 Time in range greater than 70% has been shown in multiple analyses to correlate loosely with a hemoglobin A1c of about 7.0%.16,17 A hemoglobin A1c target of 7.0% or less is supported by multiple landmark diabetes studies, including the UK Prospective Diabetes Study and the Diabetes Control and Complications Trial data.18,19 Additionally, evidence continues to build supporting time in range itself as a key indicator of long-term complication risk.20–25 Interest is also building for using time in range as a surrogate for hemoglobin A1c, or even as a direct glycemic measure in place of hemoglobin A1c, for purposes of quality measurement.
Glucose targets in healthy and at-risk adults
Time in range also provides glucose data over a much shorter timeframe than hemoglobin A1c. This frees clinicians from the traditional hemoglobin A1c– based 3-month cycle for visits, allows for more frequent changes to the diabetes regimen, and potentially reduces clinical inertia. The same international CGM consensus committee has created modified (less stringent) time-in-range goals for individuals with reduced life expectancy or significant comorbidities.15
Average glucose and glucose management indicator, 2 glycemic metrics on the AGP Report (Figure 1A), may help determine whether action is needed. The average glucose reflects values over the data collection period. The directly related glucose management indicator, expressed as a percentage, can be used clinically to estimate the hemoglobin A1c, a measure familiar to clinicians and patients.
The glucose management indicator is a calculation based on CGM-derived average glucose, and often does not align exactly with laboratory-measured hemoglobin A1c for a variety of reasons.26 It is based purely on glycemia over the period reflected on the AGP Report and can vary from the 3-month time-averaged hemoglobin A1c due to short-term clinical impacts (eg, change in diet, use of steroids, or short-term stress). Calibration accuracy of individual sensors can impact the accuracy of glucose management indicator estimates. Additionally, the glucose management indicator is a derived value based on a linear regression equation and may not accurately correlate with laboratory hemoglobin A1c at the extremes of hemoglobin A1c values (ie, people with hemoglobin A1c in the normal range or above 10%). Conversely, laboratory-measured hemoglobin A1c can vary significantly from measures of true glycemia based on many factors impacting the life span of red blood cells.27,28
Variance between the glucose management indicator and hemoglobin A1c is common, expected, and often related to known factors impacting hemoglobin A1c measures. More recent data suggest that extending the data collection period for CGM metrics beyond 14 days may decrease the impact of short-term behavioral or other changes, improving the reliability of the glucose management indicator measure.29
Glucose variability is a measure of variation in glucose readings at a given time of day over the course of the AGP Report period (Figure 1A). Increased glucose variability is an important risk factor for hypoglycemia and likely correlates with longer-term vascular risk.30 Glucose variability is expressed on the AGP Report in terms of percent coefficient of variation. An important clinical correlate is that if the percent coefficient of variation is elevated (> 36%), the likelihood of hypoglycemia is high; by consensus, the target for glucose variability is 36% or less.15,31 Often, high glycemic variability is associated with changes in diet, physical activity, or lack of adherence to medication, such as skipping insulin doses or taking rapid-acting insulin after the meal rather than before.
Step 2: Identify where action is needed
Evaluation of time in range allows rapid determination of whether a change in therapy is needed. Further data are needed to determine where the changes are needed. For that, it is necessary to review the AGP curve and the daily glucose profiles.
The AGP curve is a “modal day” view, representing all the glucose readings from the entire AGP Report period combined and presented over a single 24-hour period (Figure 1B). The AGP curve has a thick median line, 25% to 75% interquartile range lines (indicating where 50% of the values fall at that specific time), and 5% to 95% lines as outer boundaries. The curve allows evaluation of crucial questions:
Is there a pattern of dangerous hypoglycemia at a certain time of day?
Is there a postprandial pattern or hyperglycemia throughout the entire day or night or both?
Is there excessive variability suggesting a role for modifying diet, physical activity, or medication adherence?
The AGP curve shows patterns of hypoglycemia (time below range) and hyperglycemia (time above range) that indicate quickly where action is needed.
The goal of glycemic therapy is to optimize normoglycemia while minimizing hypoglycemia. Therefore, the AGP curve can help focus therapies on interventions that reduce variability (ie, “flattening” the median line and reducing the spread of the 95% and 5% lines) while decreasing hyperglycemia and hypoglycemia by improving time in range. The goal in evaluating therapies based on the AGP curve is to move from a profile of excessive variability to a profile that is as close to normoglycemia as can be done safely. Focusing first on hypoglycemia is important in improving short-term safety; decreasing excessive variability can dramatically improve hypoglycemia risk. The focus should be on making the AGP curve flat, narrow, and in range by keeping the median line as flat as possible, the spread between the 95% and 5% lines as narrow as possible, and the whole curve in range between 70 and 180 mg/dL to the extent possible.
Daily glucose profiles provide thumbnails of daily values (Figure 1C). When a glycemic concern is identified on the AGP curve, daily glucose profiles facilitate further evaluation:
Is the issue caused by a glycemic pattern observed on multiple days or a single day?
Is there a difference on specific days of the week (eg, weekday vs weekend)?
Is an outlying value causing the pattern in the AGP curve (a target for discussion of lifestyle and dietary issues that can impact glycemia) or an artifact?
Possible causes of artifacts in CGM data can include compression of the CGM sensor during sleep, displaced or malfunctioning sensor electrodes, or connectivity problems. Typically, artifactual CGM data, or data for which there is no rational clinical explanation, may be dismissed in evaluating the AGP Report.
Step 3: Act on the glycemic data
The AGP Report augments shared decision-making with the patient, enhancing the ability to work together to develop a plan focused on lifestyle and medication changes that address glycemic patterns identified in Step 2. Abnormal patterns can be a target for intensification or reduction in therapy; they can also suggest potential changes such as reducing carbohydrate intake or increasing physical activity to improve troublesome patterns. For safety, we address patterns of hypoglycemia first and then consider hyperglycemia patterns, either at the current or at subsequent visits, to further optimize glycemic patterns. We recommend focusing on no more than 1 or 2 glycemic patterns of concern at a time.
CASE PRESENTATION
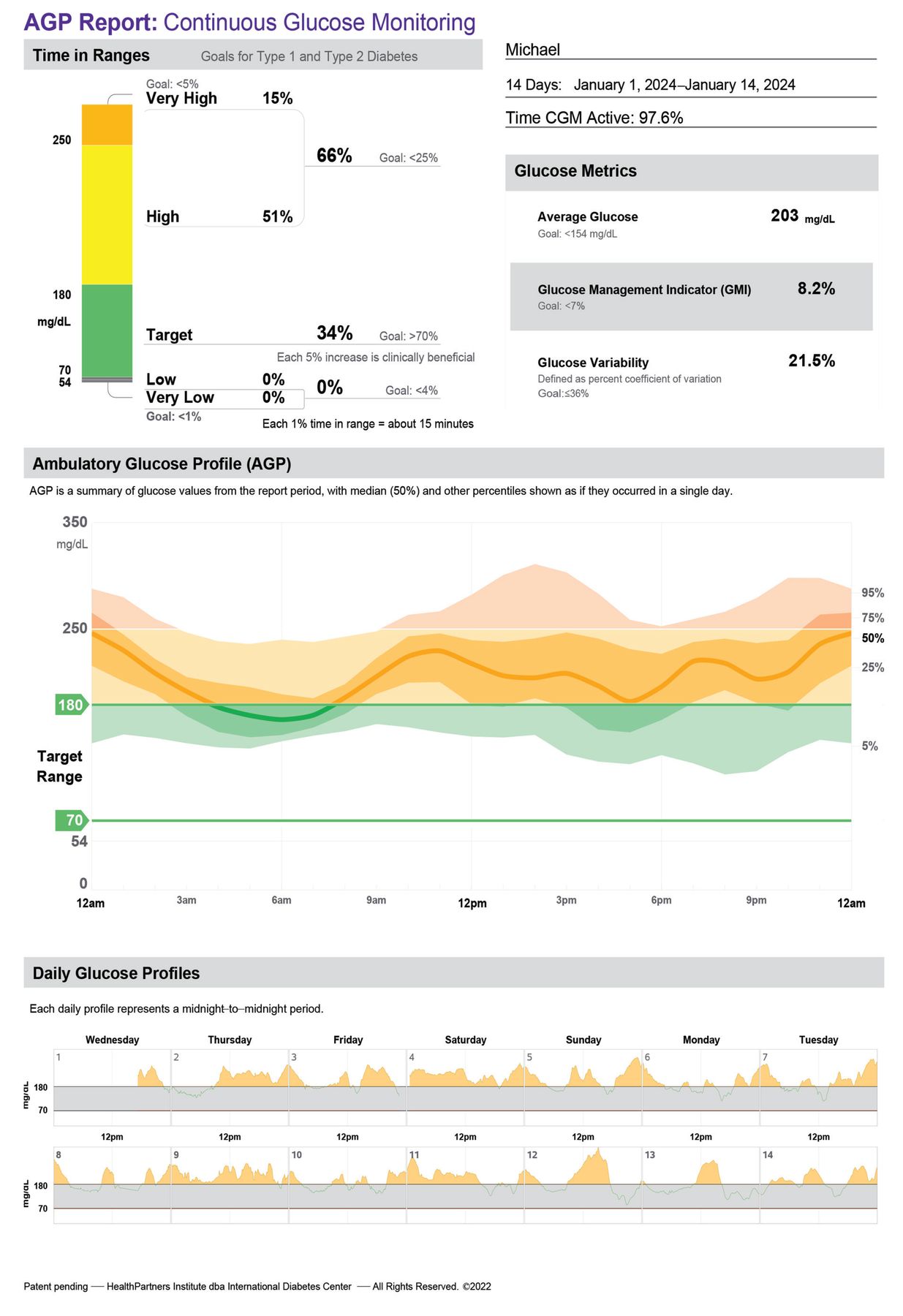
Michael, a 65-year-old man on a regimen of basal and bolus insulin (background and mealtime bolus insulin) along with noninsulin therapies, is not meeting glycemic goals. His demographic and clinical data are outlined in Table 3 and his glucose data in Figure 2.
Case presentation: clinical data

Patient’s Ambulatory Glucose Profile Report.
©2024 International Diabetes Center, Minneapolis, MN. Used with permission. Visit AGPreport.org for more information.
Based on the “Determine Where to Act” guide, the first step is to review time-in-ranges metrics, with special attention to time below range. Michael’s time in range, 34%, is well below the clinical target of 70% or greater, and his time below range is 0%. We quickly determine that action is needed to improve his glycemic profile.
Step 2, “Identify where to act,” requires review of the AGP curve and daily glucose profiles. Several patterns are apparent. Michael has a “stairstep” rise in glycemia during the day, corresponding with breakfast, dinner, and an evening snack. Overnight, median glucose drops from 250 mg/dL at midnight to 170 mg/dL at 6 am. The pattern of an exaggerated overnight drop in glucose and a stairstep rise during the day suggests too much basal (background) insulin and too little bolus (mealtime bolus) insulin. Michael’s average glucose of 203 mg/dL without hypoglycemia also demonstrates that the total daily dose of insulin is inadequate.
Step 3, “Act on the glycemic data,” involves adjusting Michael’s therapies. We address any pattern of hypoglycemia first, as that is the biggest short-term risk to patients with diabetes. Michael has no significant hypoglycemia, so our next move is to optimize insulin therapy to address hyperglycemia. Michael’s insulin regimen contains an excessive amount of basal insulin relative to mealtime insulin. As a rule of thumb, the balance between basal and bolus insulin is typically 50:50 (with some individual variation in this balance).32 This imbalance is reflected in the AGP curve, which shows a drop in glucose overnight (due to too much basal insulin), then a rise, with meals, throughout the day (due to too little mealtime insulin). A reasonable intervention would be to increase the total daily dose of insulin by 10%, then divide the total daily dose of insulin equally between basal insulin and bolus insulin. This would “rebalance” the basal and bolus insulin by redistributing the total daily dose of insulin 50:50 between basal and bolus.
With a current total daily insulin dose of 90 units (60 units of basal and 30 units of bolus insulin), we would add 10% (roughly a total daily dose of 100 units), split that between basal (50 units) and bolus (50 units) dosing, and then divide the bolus insulin between the 3 meals for a new insulin regimen of 50 units of glargine at bedtime with 16 units of lispro with meals. CGM-based management allows a more rapid cycle time. We could revisit titration in 2 weeks with a new AGP profile and continue titration until the regimen is optimized to match individual basal and bolus insulin needs.
CGM CLINICAL PEARLS
Modern CGM technology is typically straightforward and easy to use. Online videos and web-based instruction can be helpful at start-up. Additionally, care team–based resources like trained and designated staff can help ensure that data are available to clinicians at the time of clinical interactions. Building the team is a worthwhile effort to ensure success. Coding for CGM is shown in Table 4.
Coding for continuous glucose monitoring
Difficulties encountered by users of CGM technology often revolve around problems with sensor adhesion or with skin irritation and dermatitis. Trimming of body hair in the area of sensor placement can be helpful, and various available skin protectants and barriers can help both with adhesion and irritation issues. Adhesive overlays are widely available and can address adhesion issues. For patients experiencing significant challenges, local diabetes educators often have significant expertise in overcoming these challenges and can be an ideal resource.
Some commercially available CGM sensors have not been approved for use with magnetic resonance imaging, computed tomography, or radiographic technologies, and consideration should be given to removal before such testing. We recommend checking with the manufacturer’s recommendation for use of CGM sensors with these technologies.
Therapeutic substances can variably interfere with glucose sensing by CGM sensors. Interference by therapeutic quantities of acetaminophen has largely been overcome, but high-dose aspirin and vitamin C can affect glucose readings, as can hydroxyurea and, for some sensors, alcohol.33 Review of interfering substances based on CGM manufacturer recommendations is advisable.
Finally, no technology is immune from variance and errors. Neither blood glucose monitoring nor CGM technology is a “gold standard” in evaluating glucose, and variations between readings and between devices are to some degree expected. All CGM sensors are known to be less accurate in the hypoglycemia range. Concerning symptoms or discordant data may warrant confirmation with an alternate technology. Unexpected or outlying CGM data should optimally be confirmed with blood glucose monitoring if there are questions regarding the validity of data.
DISCLOSURES
Dr. Martens has disclosed consulting for Sanofi; serving as an advisor or review panel participant for Eli Lilly; teaching and speaking for Abbott Diabetes Care, Dexcom, and Eli Lilly; serving as a research principal investigator for Abbott Diabetes Care, Dexcom, and Novo Nordisk; serving as a co-principal investigator for Capillary Biomedical, Eli Lilly, Insulet Corporation, Sanofi, and Tandem Diabetes Care. Dr. Simonson has disclosed consulting for Abbott Diabetes Care and teaching and speaking for Abbott Diabetes Care and Sanofi. Dr. Bergenstal has disclosed intellectual property rights (royalties or patent sales) for Medtronic; consulting for Abbott Diabetes Care, Dexcom, Lilly, Medtronic, Novo Nordisk, and Tandem Diabetes; serving as an advisor or review panel participant for Abbott Diabetes Care, Dexcom, Lilly, Medtronic, and Novo Nordisk; serving as a research principal investigator for Abbott Diabetes Care, Insulet Corporation, Lilly, Medtronic, Novo Nordisk, and Tandem Diabetes; and serving as a research co-principal investigator for Abbott Diabetes Care, Dexcom, Insulet Corporation, Lilly, Medtronic, Novo Nordisk, and Tandem Diabetes.
The authors’ employer, nonprofit HealthPartners Institute, contracts for their services and no author receives personal income for these services.
- Copyright © 2024 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}