


A 22-year-old man presented to the otolaryngology clinic with a 3-month history of painless oral lumps and intermittent sore throat. He had no significant medical history, was sexually active with other men, and was otherwise well.
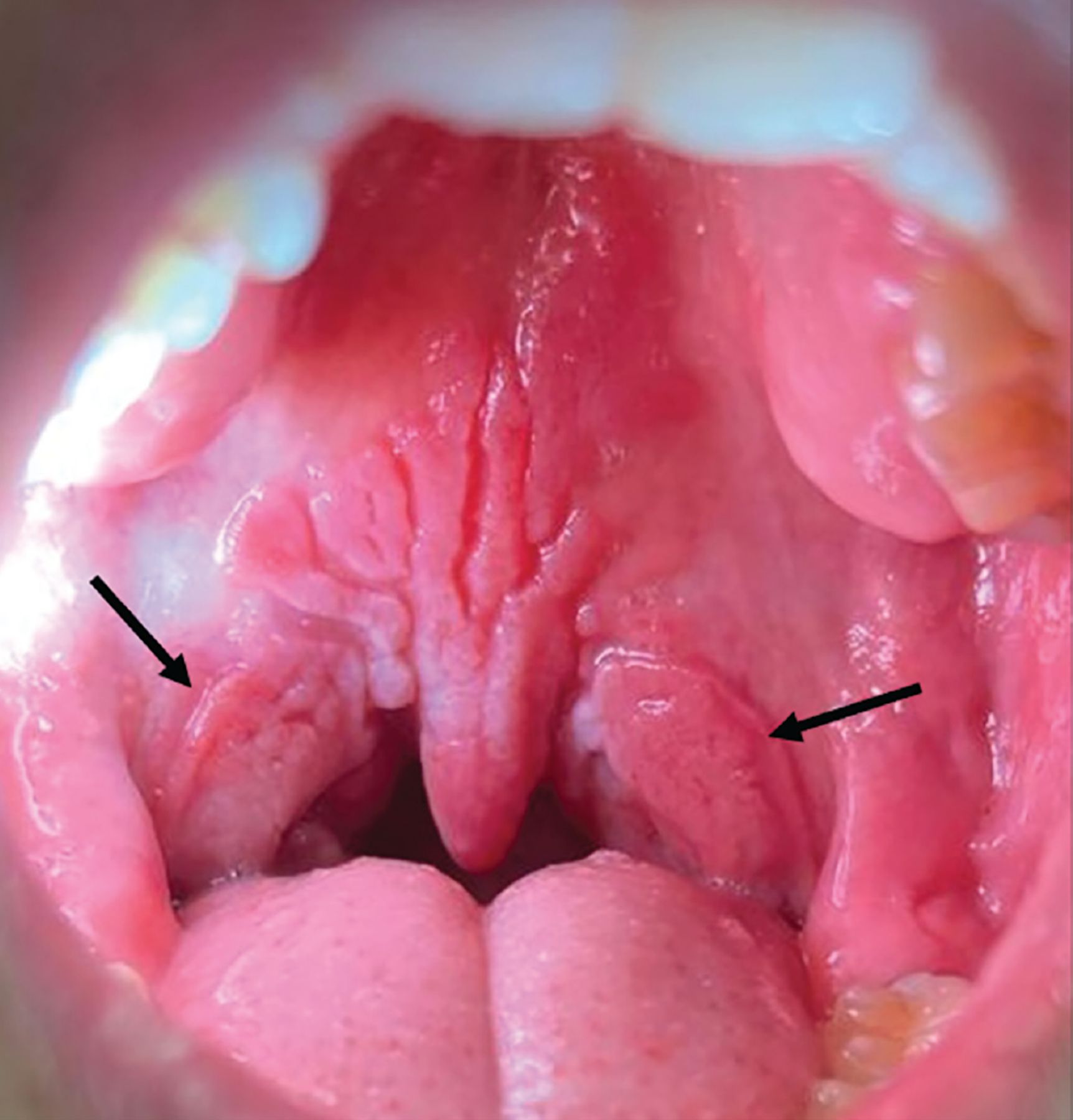
Physical examination revealed diffuse edema of the oropharynx and nontender, well-demarcated mucosal patches on the soft palate, including the uvula and both palatoglossal arches (Figure 1). Examination of the entire body revealed no evidence of rash, lymphadenopathy, or anogenital lesions.

Oral condylomata lata of secondary syphilis (black arrows).
Biopsy of the soft-palate lesion showed intense acute and chronic inflammation, with large numbers of spirochaetal organisms within the surface epithelium (Figure 2). Screening tests for human immunodeficiency virus, Chlamydia trachomatis, and Neisseria gonorrhoeae were negative. However, a rapid plasma reagin test was positive (titer 1:256).

High-power image (1,000 × original magnification) of immunohistochemistry staining positive for Treponema pallidum showing numerous long, thin, spirally coiled organisms stained brown (red arrows) within the surface epithelium.
The patient’s clinical findings were consistent with oral condylomata lata of secondary syphilis. He was subsequently treated with 1 dose of intramuscular benzylpenicillin, with full resolution of the oral lesions within 2 weeks.
ORAL MANIFESTATIONS OF SYPHILIS
Syphilis is a sexually transmitted infectious disease caused by Treponema pallidum. The incidence of primary and secondary syphilis has been increasing in the United States and worldwide in recent years.1,2
Oral manifestations of syphilis may occur in all 4 stages of the infection—primary, secondary, latent, and tertiary—but are most common in the secondary stage.2 The occurrence, however, of purely oral lesions, such as in this case, is a rarely reported entity.3
The clinical presentation and histology of oral lesions differ depending on the stage of syphilis. In primary syphilis, a single painless oral chancre is characteristic. Chancres are generally asymptomatic and present as a single ulcerated, erythematous lesion at the site of inoculation.2
Without adequate treatment, about one-quarter of primary infections will progress to secondary syphilis within 4 to 6 weeks after the appearance of the primary lesion.4 Immunohistochemistry confirms the diagnosis and demonstrates numerous spiral-shaped spirochetes that infiltrate the epithelium.1 Oropharyngeal manifestations in secondary syphilis are typically multiple, reflecting the hematogenous dissemination of the microorganism. These include highly infectious macules, papules, and ulcers, with patients often presenting with pharyngitis, tonsillitis, and laryngitis and nonspecific systemic symptoms such as malaise and fatigue.2 Condylomata lata, a classic finding in secondary syphilis, are firm, moist, gray or white papules most often found in the anogenital region. They are infrequently reported in the oral cavity.5
Without treatment, the infection progresses to a latent phase in which the clinical signs of secondary disease resolve but patients retain positive serology.2 It is generally an asymptomatic phase, although patients may experience mucocutaneous lesions.
A portion of infections will then progress over time to late or tertiary disease. The tertiary phase of infection may manifest in the mucus membranes with oral syphilitic gummas. These generally have a necrotic base and can be associated with destruction of the hard and soft tissue, including palatal perforation.1,4 Gummas that affect the tongue can cause diffuse atrophy, termed “luetic glossitis.”1
These varied oropharyngeal presentations are often one of the first signs of infection. Because some patients with undiagnosed syphilis may present only with oral lesions, early recognition of oropharyngeal condylomata lata with serologic confirmation should allow for definitive diagnosis and treatment, which may eliminate the need for biopsy if the lesions respond to treatment.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2024 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.