


A 47-year-old woman presented with a 2-month history of pruritic eruptions on the left ankle and a complaint of thirst and polyuria for the past year. She was previously healthy and denied a history of insect bites.
Physical examination revealed multiple umbilicated hyperkeratotic papules and nodules with a central round crusted ulcer on the left ankle (Figure 1). Histologic study of the lesions revealed cup-shaped invagination of the epidermis plugged with necrotic inflammatory debris and transepidermal elimination of dermal collagen (Figure 2). Laboratory testing showed the following:
Fasting glucose 7.8 mmol/L [140.4 mg/dL] (reference range 3.9–5.6 [70–100])
Hemoglobin A1c 6.9%
Triglycerides 2.38 mmol/L [210.6 mg/dL] (< 1.7 [< 150])
Total cholesterol 7.21 mmol/L [278.4 mg/dL] (< 5.18 [< 200]).

Multiple umbilicated hyperkeratotic papules (black arrows) and nodules (blue arrows) with a central round crusted ulcer on the left ankle.

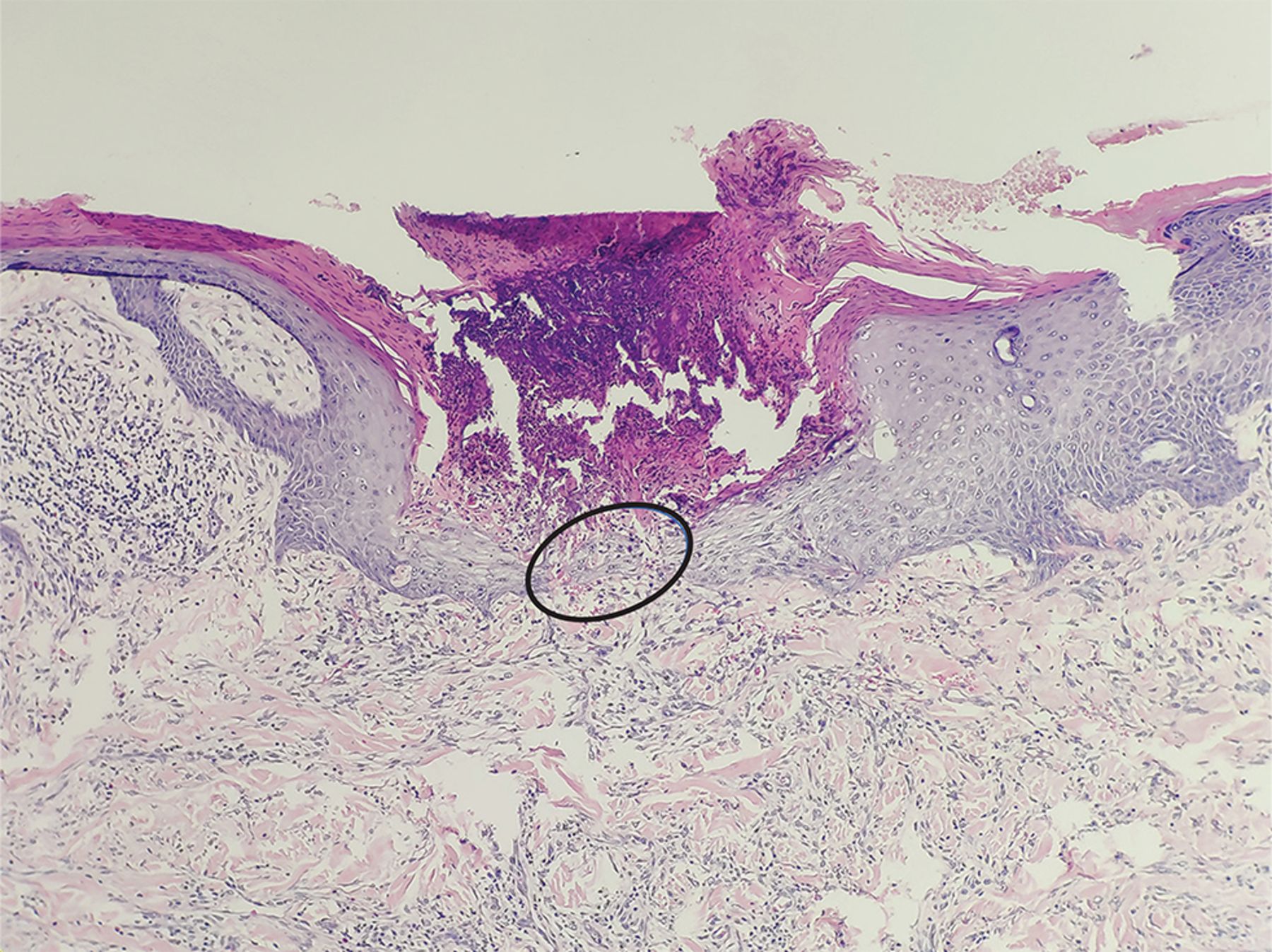
Histologic study of a papule revealed cup-shaped invagination of the epidermis, plugged with necrotic inflammatory debris, and transepidermal elimination of dermal collagen (circled area) (hematoxylin and eosin stain, magnification × 100).
Based on the clinical presentation and the results of histologic study and blood testing, we diagnosed acquired reactive perforating collagenosis and type 2 diabetes. The patient was referred to endocrinology for management, and her lesions improved after 4 weeks of treatment with loratadine and halometasone cream.
ACQUIRED PERFORATING DERMATOSIS
Perforating dermatoses are a group of chronic pruritic cutaneous disorders characterized histologically by transepidermal elimination of dermal components, ie, the components “perforate” the epidermis. They are divided into primary and secondary (ie, acquired) forms and, based on the dermal components of transepidermal elimination, can be further classifed into 4 subtypes: Kyrle disease, reactive perforating collagenosis (as in our patient), elastosis perforans serpiginosum, and perforating folliculitis.1
Acquired perforating dermatosis (APD) usually affects the extensor surfaces of the extremities and trunk and presents as multiple, nonfused, umbilicated, hyperkeratotic papules or nodules consisting of a central round crusted ulcer with a reddish brown raised border.
Symptoms and other features
Epidemiologic studies of APD are lacking. Seven retrospective case series studies have summarized a total of 282 cases of APD.1–7 The condition mainly affects patients in their 40s and 50s. Pruritus was the most common symptom, with a few complaining of pain. Koebner phenomenon was seen in 32% to 56% of patients.2–4,6,7
Patients with APD often have an underlying systemic disease, particularly diabetes (type 1 or type 2) or chronic kidney disease.1–7 Other underlying comorbidities include cardiovascular disease, infection (human immunodeficiency virus, hepatitis virus, and tuberculosis), rheumatic disease, pulmonary disease, malignancy, psychiatric disease, hypothyroidism, pregnancy, and dermatoses (atopic dermatitis, psoriasis, scabies).1–7
Pathogenesis still unclear
The pathogenesis of APD remains unknown. Possible theories include microtrauma caused by scratching prompted by pruritus, microangiopathy, and overloading of urinary metabolites due to renal insufficiency.4 In 1 study, pruritus was the most common symptom, and the presence of the Koebner phenomenon suggests that trauma plays a role in the pathogenesis of APD.4 Chronic pruritus is a symptom of many systemic diseases, including diabetes and chronic kidney disease. Diabetic microangiopathy may be involved in the formation of local hypoxia and necrosis.4
The differential diagnosis
The differential diagnosis includes insect bites, atopic dermatitis, and lichen planus. The lesions of APD typically have a crater-like structure, presenting as rounded, necrotic, dark brown crusts of variable size in the center of papulonodular lesions surrounded by a reddish brown halo. When lesions are atypical or the diagnosis is in doubt, histologic evidence of transepidermal elimination can confirm the diagnosis.
Treatment
Treatment of the underlying disease may help to improve APD.8 First-line therapies include antihistamines and topical emollients, corticosteroids, and keratolytics. Second-line options include intralesional corticosteroid injections and topical tretinoin, tazarotene, and imiquimod. Other potentially effective treatments include systemic drugs (retinoids, allopurinol, doxycycline, and corticosteroids), dupilumab,6 nemolizumab,9 narrow-band ultraviolet B light, and psoralen plus ultraviolet A light.1,2,8
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2024 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.