


Article Figures & Data
Figures
- Figure 1
Bidirectional ventricular tachycardia in a patient with digoxin toxicity. The QRS axis alternates with each QRS complex (see rhythm strip for lead II).
- Figure 2
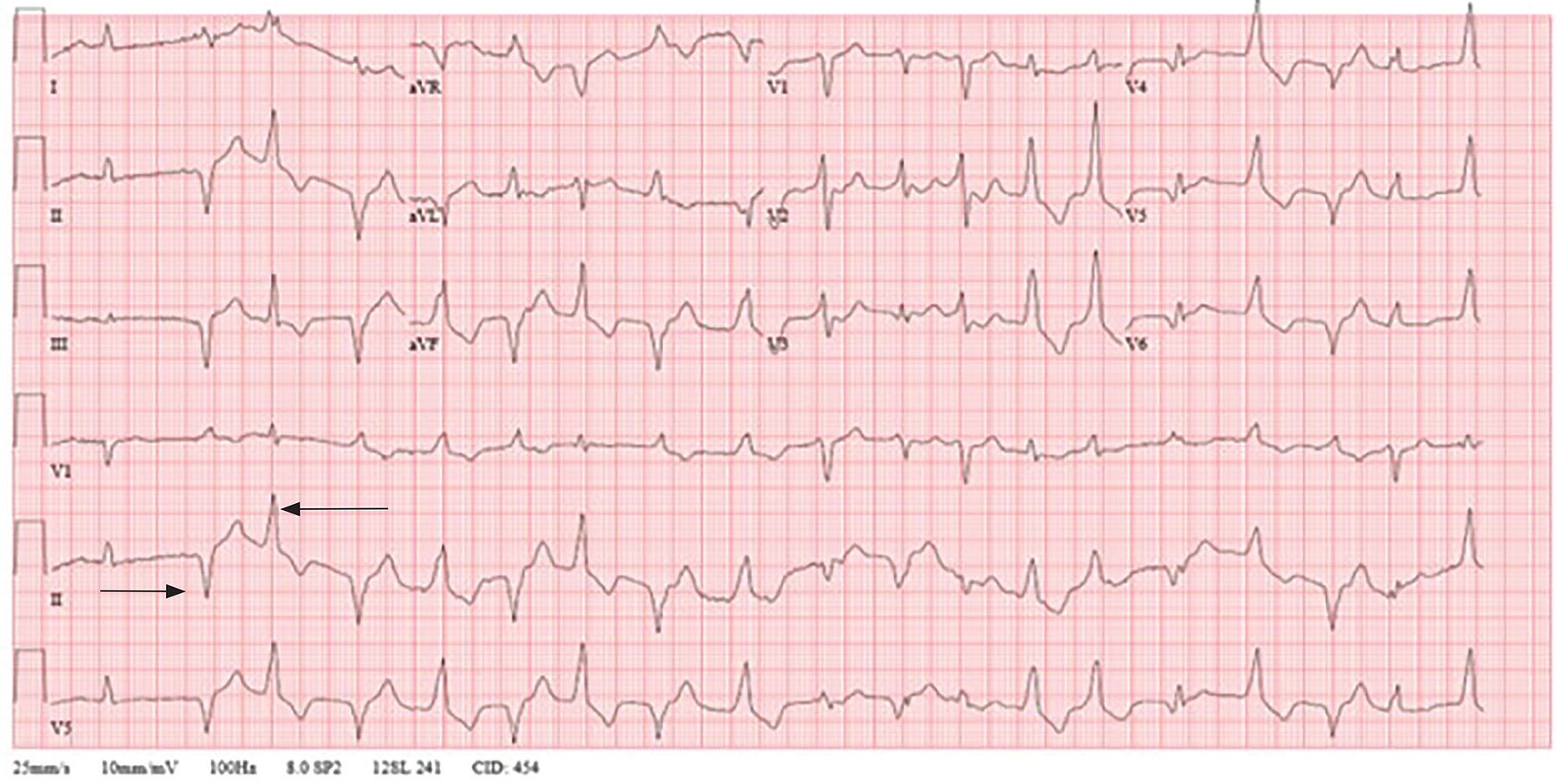
Electrocardiogram showing “sagging” ST depressions, most notably in leads V3–V6 and lead II, and ventricular ectopy in a patient with digoxin toxicity with a serum level of 8.0 ng/mL (normal range 0.6–1.2).
- Figure 3
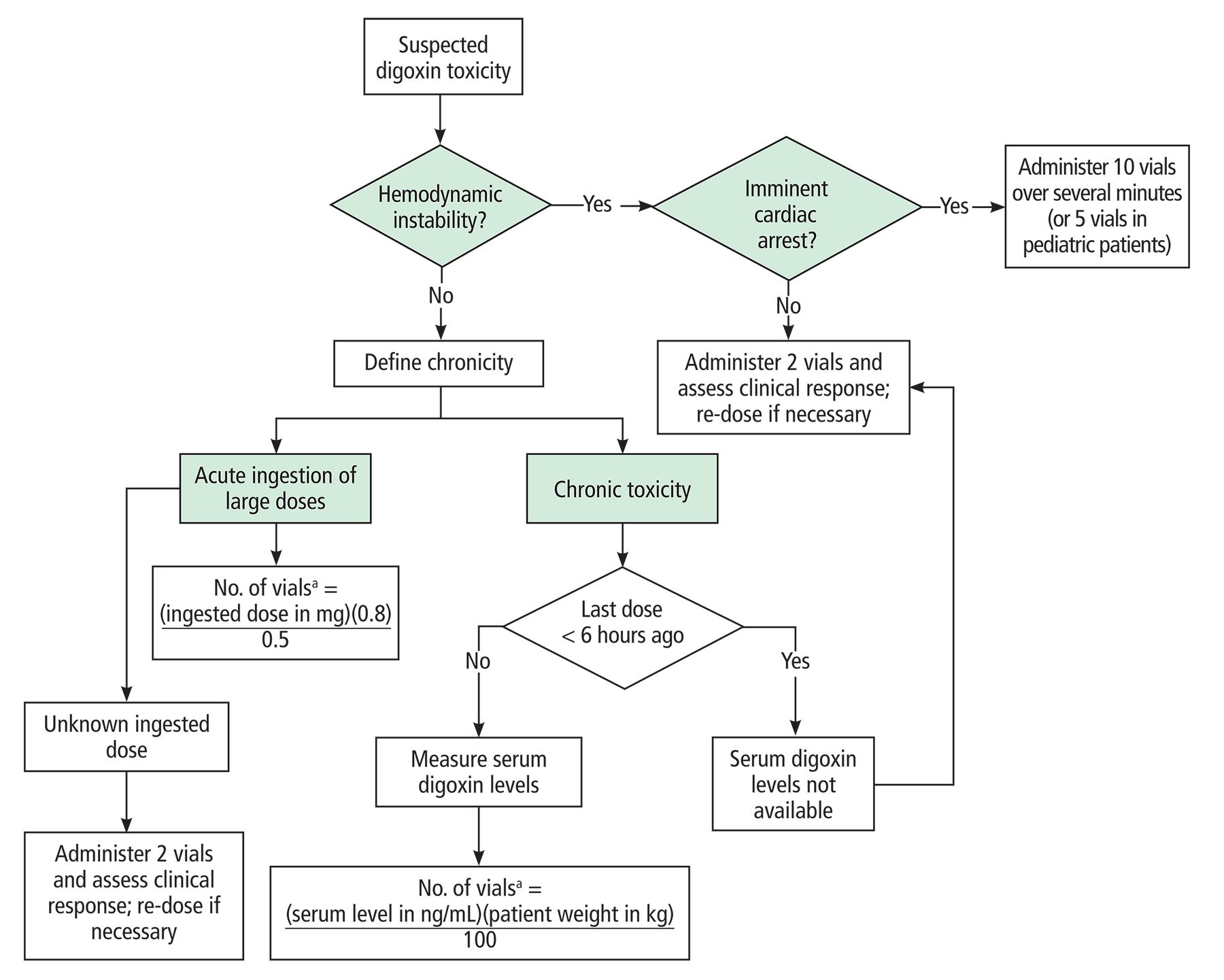
Treatment of severe digoxin toxicity with digoxin-fab.
aThe calculated number of vials should be rounded up to the nearest digit. Each vial contains 38 to 40 mg of digoxin-fab.
Based on information from reference 29.



Tables
Indication Dosing Desired serum concentration Comments Symptomatic heart failure with reduced ejection fraction despite guideline-directed medical therapy 0.125–0.25 mg daily, modified according to nomogram of Jelliffe and Brooker6 0.5–0.9 ng/mL No need for loading dose
Low doses (0.125 mg daily or every other day) should be used initially if the patient is > 70 years, has impaired renal function, or has a low lean body massRate control in atrial fibrillation with decreased left ventricular function or hemodynamic instability Loading dose: 0.25 mg intravenously with repeat dosing every 6 hours to a maximum of 1.5 mg over 24 hours
Maintenance dose: 0.125–0.25 mg daily0.5–1.2 ng/mL For individuals with low body weight (45–70 kg) and renal dysfunction, loading doses should be reduced to 0.7 to 1.0 mg in the first 24 hours Based on information from references 3–5.
Medication Mechanism of interaction Comments Amiodarone, quinidine, dronedarone, nondihydropyridine calcium channel blockers (diltiazem and verapamil), propafenone, flecainide, clarithromycin, cyclosporine, itraconazole Inhibition of P-glycoprotein, a drug efflux pump that mediates secretion of digoxin in the kidney, liver, and gut Digoxin dose may have to be decreased to half when starting any of these medications
Check digoxin levels 1 week after starting any P-glycoprotein inhibitorMacrolides (azithromycin, clarithromycin, erythromycin) and tetracycline Decreased initial degradation of digoxin by gut microflora, leading to increased drug absorption Monitor levels closely when co-administering digoxin with these antibiotics Diuretics, amphotericin B Decreased glomerular filtration rate and hypokalemia can increase digoxin toxicity Monitor potassium levels to avoid hypokalemia Nonsteroidal anti-inflammatory drugs, angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, cyclosporine Decreased glomerular filtration rate and acute kidney injury Telmisartan increases digoxin concentration by about 50% Beta-blockers, nondihydropyridine calcium channel blockers Slowing of atrioventricular conduction can lead to bradycardia compounding on digoxin’s vagotonic effects Increased risk of bradycardia; carvedilol can increase digoxin concentration Amiodarone, sotalol, quinidine, procainamide, dofetilide, ibutilide, quinolones, macrolides, azole antifungals, tricyclic antidepressants, antipsychotics, methadone QT-prolonging agents increase risk of life-threatening arrhythmias as digoxin increases early afterdepolarizations, which can lead to R-on-T phenomenon and torsade de pointes Monitor QT closely when adding any of these medications Based on information from references 17 and 18.
Risk factor Comments Advanced age Reduced volume of distribution due to lower muscle mass and reduced renal drug clearance can lead to higher serum concentrations of digoxin in the elderly
Digoxin use has been linked to higher mortality in patients age 65 and older with atrial fibrillation and heart failure19Renal dysfunction Digoxin is primarily excreted by the kidneys and its clearance is directly proportional to the glomerular filtration rate
Reduced renal clearance results in higher serum digoxin concentration, and dose should be reduced in patients with renal dysfunction
Any condition that leads to acute renal injury (eg, dehydration, sepsis, glomerular or tubular disease, or decompensated heart failure) can predispose to toxicity
Digoxin use in patients with end-stage kidney disease undergoing hemodialysis is associated with a 28% increase in mortality and is therefore not recommended20
If needed in end-stage kidney disease, a loading dose of 3 to 5 μg/kg (0.25–0.375 mg) is recommended, followed by a maintenance dose of 0.0625 mg every 48 hoursHypokalemia Decreased potassium levels result in decreased competition for the binding spot of digoxin in sodium-potassium adenosine triphosphatase, favoring binding of digoxin to the ionic pump17 Drug interactions Diuretics, antiarrhythmic drugs, and antibiotics can increase serum digoxin concentration or enhance digoxin action17,18 Cardiac Tachyarrhythmias Bidirectional ventricular tachycardia Ventricular tachycardia Ventricular fibrillation Atrial fibrillation Supraventricular tachycardia Bradyarrhythmias Sinus bradycardia Atrioventricular block Asystole Increased ectopy Atrial ectopy Ventricular ectopy Ventricular bigeminy Gastrointestinal Nausea Vomiting Abdominal pain Mesenteric ischemia and diarrhea (rare) Central nervous system Color perception disturbances (xanthochromia) Visual disturbances (halos) Headaches Confusion Apathy Electrolyte abnormalities Hyperkalemia Constitutional Fatigue Anorexia Based on information from references 15,19,20,22,23.




{kind=link}
{kind=link}
{kind=link}