


ABSTRACT
Respiratory syncytial virus (RSV) is a threat to infants globally causing bronchiolitis and pneumonia. Despite decades of research, RSV outbreaks occur with only modest advancements in prevention or treatment. Vaccine development faced challenges because past attempts caused enhanced disease and treatment options demonstrated limited efficacy. Recent advancements, including maternal vaccines focusing on the prefusion form of the F glycoprotein are now showing significant benefits in preventing severe RSV-related illness in infants. Additionally, monoclonal antibodies offer prevention directly to newborns within 1 week of birth. These innovations have the potential to substantially change the impact of RSV.
RSV disease severity is high in early childhood, particularly in vulnerable infants, including those born prematurely or with underlying conditions such as chronic lung disease, congenital heart defects, or weakened immune systems.
The first RSV vaccine in 1966 led to worsened RSV disease in vaccinated infants, known as enhanced RSV disease (ERD), hindering the development of RSV vaccines for decades.
The identification and characterization of the prefusion conformation of the F glycoprotein was an important step forward resulting in the promising new RSV vaccines and monoclonal antibody prophylaxis now available.
Respiratory syncytial virus (RSV) is one of the most significant pathogens of early childhood. Following its recognition in 1956, it was quickly implicated as a leading cause of bronchiolitis and pneumonia among infants globally.1,2 Despite extensive research over the previous decades, RSV disease severity remains high, particularly in vulnerable infants, including those born prematurely or with underlying conditions such as chronic lung disease, congenital heart defects, or weakened immune systems.3 Various factors also increase the risk of RSV-related hospitalization including male gender, age below 6 months, birth during or immediately prior to RSV circulation, and underlying comorbidity.4
RSV disease occurs through initial infection of the upper airway epithelial cells via large droplet inoculation.5 Symptoms of upper airway involvement occur approximately 4 to 7 days following infection and include rhinorrhea, sore throat, cough, and low-grade fevers, which are common to many respiratory viruses. After replicating in the nasopharynx, RSV may spread to the lungs directly through the respiratory epithelium or by aspiration of secretions. Approximately 30% of infected infants progress to lower respiratory tract disease (LRTD) typified by development of bronchiolitis. Bronchiolitis occurs from necrosis and destruction of epithelial cells leading to airway obstruction, air trapping and increased airway resistance heralded by symptoms of worsening cough, increased work of breathing with accessory respiratory muscle use and wheezing.3 While viral pneumonia may also occur following infection, bacterial superinfection following RSV is uncommon.6 Globally, over 30 million RSV-associated lower respiratory infection episodes in young children occur annually, with lower-income countries most affected.7 In the United States, bronchiolitis caused by RSV and closely related metapneumovirus account for over 2 million outpatient visits, nearly 20% of pediatric hospitalizations, and 10% of pediatric intensive care unit (ICU) admissions annually.8
RSV outbreaks typically occur during winter months in the northern regions with temperate climates, with peak circulation in January or February. Thereafter, only sporadic cases occur between the spring and fall. However, the timing of outbreaks varies regionally. In tropical regions, RSV season typically spans from May to September often coinciding with the rainy season. While these surges in RSV disease are expected, they place tremendous strain on the pediatric hospital systems. This was most evident in the recent years following the COVID-19 pandemic when RSV circulation became displaced into the late summer leading to substantial pediatric bed shortages (Figure 1).9

RSV circulation displaced into late summer following the pandemic. Violin plots of RSV detection by International Organization for Standards week (month displayed for ease of reading) for 2020 through 2023 within Cleveland Clinic System at Ohio and Florida campuses.
Dashed line (blue) = median week of circulation; dotted line (white) = upper and lower interquartile distribution
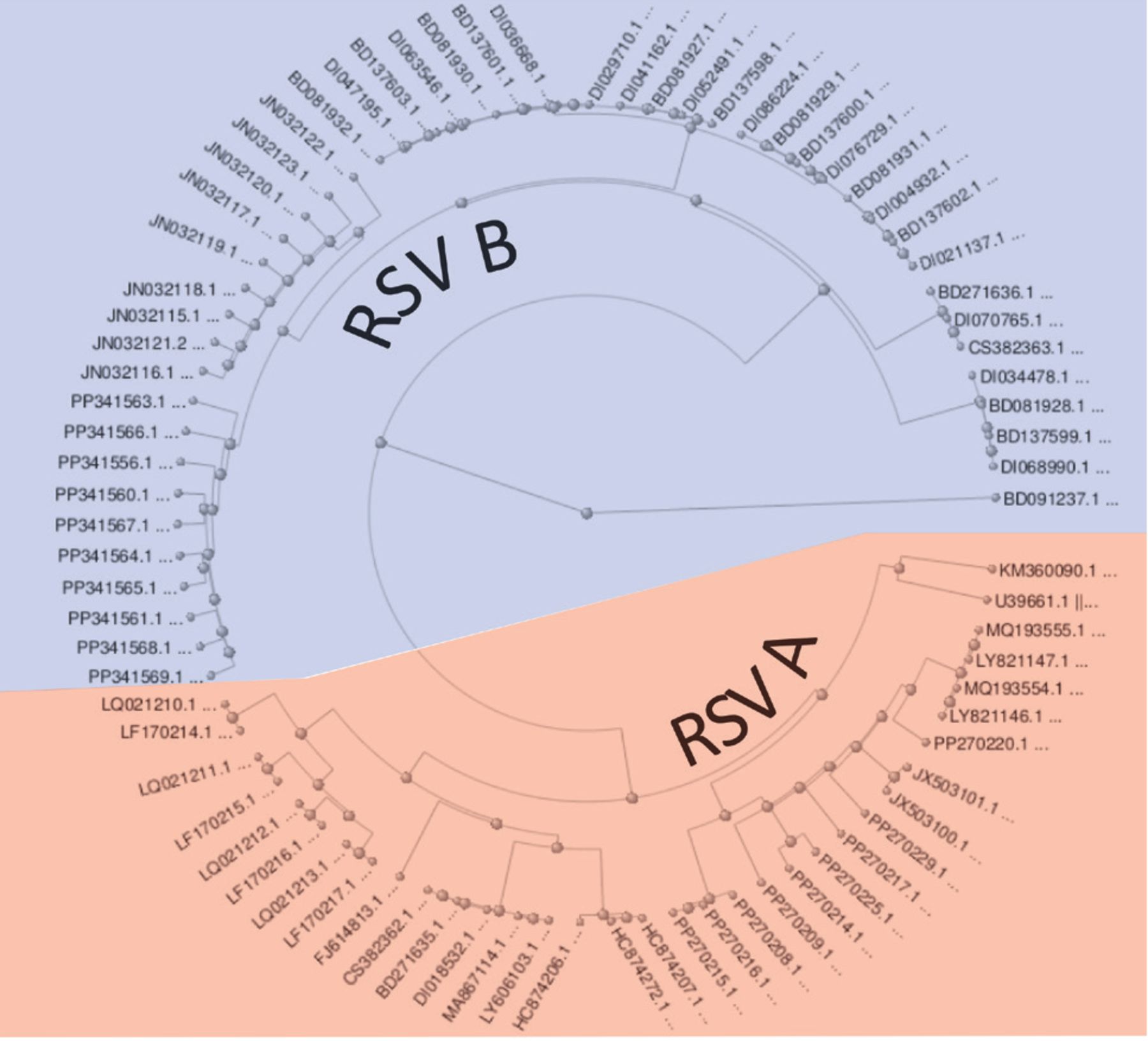
RSV is a single-stranded negative-sense RNA virus belonging to the Paramyxoviridae family and circulates within the community with multiple genotypes between the 2 major antigenic subgroups, RSV A and RSV B (Figure 2).10 The RSV genome is approximately 15 kb long and produces 11 proteins. Two of the most relevant are the G glycoprotein (mediating viral attachment) and the F glycoprotein (responsible for viral penetration and syncytium formation).3 Neutralizing antibodies produced following infection are predominantly directed against the G and F glycoproteins.11 The F glycoprotein has been a focus of vaccine research for decades with emphasis on the postfusion form of the F glycoprotein. The structure of unstable prefusion F glycoprotein was initially characterized in 2006; however, recent work introduced stabilizing mutations that allowed it to be used as the basis for vaccine and antibody development.12,13 It is now realized that several neutralizing antibodies unique to the prefusion F glycoprotein (especially site Ø) can prevent transition to the postfusion state, and significantly disrupt RSV infection much more so than antibodies targeting the postfusion state.14 Additionally, the F glycoprotein is highly conserved among RSV isolates from both A and B subgroups. Despite widespread exposure to RSV by age 2, immunity is short-lived and reinfections are common throughout life.

RSV genome subtypes A (red) and B (blue) with multiple genotypes. Eighty-one RNA sequences (accession numbers displayed) representing complete RSV genomes retrieved from GenBank.10
The development of an effective prevention and treatment for RSV has been challenging. Factors such as inadequate natural immunity, ill-defined vaccine response measures, and concerns regarding safety have hampered vaccine development.15 Numerous therapies for infected individuals have also been developed but with very limited success. Here we describe the challenges and future directions in developing effective prevention and treatment against RSV in children.
RSV VACCINES
RSV vaccine development began soon after discovery of the virus. One of the initial vaccines was the formalin-inactivated (FI) RSV vaccine in 1966. Following a 3-dose vaccination series with FI RSV, 43% of infant vaccinees demonstrated a 4-fold or greater rise in serum neutralizing antibody levels and 91% displayed a rise in serum complement-fixing antibody levels.16–19 However, it was quickly observed that vaccinated children not only did not exhibit protection against natural infection, but RSV illness became more severe in RSV-naïve vaccinated infants compared with the control group. Nearly 80% of RSV vaccine recipients required hospitalization with RSV infection, compared with 5% in the control group. Two immunized children died as a consequence.18 This aberrant immunity elicited by FI-RSV vaccine was subsequently termed enhanced respiratory disease (ERD).17
Over the decades, much research has been devoted to understanding the structural and immunological mechanisms of ERD.20,21 From this initiative, it was realized that ERD is linked to the induction of antibodies with weak avidity and reduced neutralizing activity in RSV-naïve children. This aberrant response leads to exaggerated complement fixation and immune complex deposition and T helper type 2-biased memory CD4 + T cell responses, which cause an exaggerated inflammatory response leading to worsened fever, airway constriction, and bronchopneumonia.20 The occurrence of ERD has led to caution in the development of RSV vaccines, emphasizing the importance of carefully assessing vaccine candidates for this specific outcome.
The concerns for ERD hindered the development of RSV vaccines for many years. Researchers developed multiple, live-attenuated vaccines modified to prevent enhanced disease, but efficacy was poor in clinical trials. The transition from inactivated whole virus vaccines to structure-based vaccines led to trials using subunit based, and purified fusion protein-based vaccine candidates without successful results.22 One example includes an RSV F-protein recombinant nanoparticle vaccine candidate that progressed to phase 3 trials in 2016 but failed to demonstrate efficacy against moderate to severe LRTD caused by RSV.23 Another RSV vaccine subunit vaccine (MEDI-7510) using soluble postfusion conformation of the F glycoprotein along with a TLR4 agonist adjuvant was discontinued after a phase 2b trial due to poor response.17
While RSV has traditionally been associated with infections in children, substantial disease was soon recognized in older adults when virus outbreaks occurred in long-term care facilities.24,25 Since then, additional studies have increasingly recognized RSV as an important cause of morbidity and death among elderly and high-risk adults.26 Due to concerns for ERD and the difficulty recruiting young children for clinical trials, the development of an RSV vaccine for elderly adults became a more plausible option for the vaccine industry.27
The recognition that the prefusion conformation of the F glycoprotein generates more potent neutralizing antibodies became a significant step forward in RSV vaccine development.14 Considerable progress has been made focusing on vaccine candidates targeting this prefusion form. In 2023, data on 2 prefusion vaccines to prevent disease in adults was published by GSK (RSVPreF3 OA) and Pfizer (RSVpreF).28,29 For the GSK vaccine, efficacy was estimated at 94.1% (95% confidence interval [CI], 62.4–99.9) against severe RSV-related LRTD and 71.7% (95% CI, 56.2–82.3) against RSV-related acute respiratory infection.28 For the Pfizer vaccine, efficacy was estimated at 66.7% (96.7% CI, 28.8–85.8) against RSV-associated lower respiratory tract illness (LRTI) with at least 2 signs or symptoms and 85.7% (96.7% CI, 32.0–98.7) against more severe illness (3 or more signs or symptoms).29 The U.S. Food and Drug Administration subsequently approved both RSV vaccines for adults 75 and older and those 60 to 74 who are at increased risk of severe RSV disease.
Furthermore, to prevent severe RSV disease in newborns while averting the risk of ERD, maternal vaccination compared with placebo was evaluated in 2 studies.30,31 The MATISSE (Maternal Immunization Study for Safety and Efficacy) trial used 2 primary efficacy end points: medically attended severe RSV-associated LRTI and medically attended RSV-associated LRTI in infants within 90, 120, 150, and 180 days after birth.30 RSVpreF vaccination of the mother reduced infant risk of severe LRTI by 81.8% (99.5% CI, 40.6–96.3) within 90 days after birth and by 69.4% (97.58% CI, 44.3–84.1) within 180 days after birth. Efficacy for medically attended RSV-associated LRTI within 90 days after birth was 57.1% (99.5% CI, 14.7–79.8) and at 180 days after birth was 51.3% (97.58% CI, 29.4–66.8). The incidence of adverse events in infants and pregnant women were comparable between the vaccine and the placebo group. However, more preterm births and preeclampsia were observed among those who received vaccine compared with placebo, although this was not statistically significant. While available data was insufficient to establish or exclude a causal relationship between preterm birth and maternal vaccination, there did appear to be an increased incidence in events when the vaccine was administered earlier in the third trimester. Thus, due to an abundance of caution, the FDA and U.S. Centers for Disease Control (CDC) and Prevention Advisory Committee on Immunization Practices (ACIP) recommend the Pfizer RSVpreF vaccine for pregnant persons as a one-time dose 32 through 36 completed weeks gestation during seasons of RSV circulation (September to January in most of the continental United States).32,33
A recent phase 3 trial on RSV prefusion F protein-based maternal vaccine from GSK showed a vaccine efficacy of 65.5% (95% credible interval [CrI], 37.5–82.0) for medically assessed RSV-associated LRTD and 69.0% (95% CrI, 33.0–87.6) for severe medically assessed RSV-associated LRTD.34 The enrollment was stopped early because of safety concerns. Though the results show that the risk of medically assessed RSV-associated LRTD among infants was lower with the candidate RSV vaccine than with placebo, it is to be noted that the risk of preterm birth was higher in the vaccine group compared with placebo (relative risk, 1.37; 95% CI, 1.08–1.74; P = 0.01).
RSV TREATMENTS AND PREVENTION
The significant RSV morbidity and mortality prompted trials of multiple therapeutic strategies to treat active disease. Beyond standard supportive care, treatment modalities for RSV bronchiolitis may be categorized as RSV nonspecific and RSV specific. RSV-nonspecific modalities, such as corticosteroids and bronchodilators, have been trialed based on host pathophysiology. Conversely, RSV-specific interventions, including antivirals and immunoglobulins, focus on disruption of vital viral mechanisms.
RSV-nonspecific treatments
The presence of wheezing, common in infants with bronchiolitis, prompted the trial of ß-adrenergic bronchodilators, which exert their effect primarily through the relaxation of airway smooth muscle to alleviate bronchoconstriction.35 A 2014 Cochrane review found that bronchodilators in infants with bronchiolitis showed no overall impact on oxygen saturation, need for hospitalization, length of hospital stay, or illness duration.35 However, risk of tachycardia, tremors, and hypoxia were increased. While prior American Academy of Pediatrics guidelines suggested a one-time trial of bronchodilators with observation of response,36 the lack of objective support for the use of bronchodilators and the possibility for harm have led to more recent recommendations to not administer bronchodilators in infants with bronchiolitis.37 Nonetheless, there may be a subset of children who may benefit from bronchodilator therapy (eg, patients with a previous history of reactive airways).38 Corticosteroids also have a limited impact on acute disease or long-term lung function and are therefore not recommended.37 Furthermore, there is data that suggest that corticosteroids may prolong viral shedding.39
Many other nonspecific treatments have been trialed: hypertonic saline, deoxyribonuclease, and N-acetylcysteine have been used as mucolytics. However, data regarding these therapies are either lacking or suggest minimal benefit and are not recommended.40,41 Nebulized epinephrine was found in 1 large trial to have a beneficial effect in reducing hospitalization when given in combination with dexamethasone but was not statistically significant when adjusted for multiple comparisons.37,42 Chest physiotherapy to assist in clearance of mucus in the airways was analyzed in a 2016 Cochrane review and reportedly lacked benefit in time to recovery or clinical stability.43 An increase in adverse events such as transient respiratory destabilization and vomiting during the procedure was noted. Lastly, other non-specific therapies, including leukotriene inhibitors to block inflammation, bronchoconstriction, and mucous production, lack evidence to support their use.40
RSV-specific treatments
Direct antiviral treatments have similarly had a poor impact with few exceptions. Ribavirin, a nucleoside analogue, introduced in the early 1970s, was found to have efficacy against viral replication in a broad range of viruses, including RSV.44 Ribavirin’s RSV antiviral activity includes directly inhibiting viral RNA polymerase, mutagenesis of the virus genome leading to a “error catastrophe,” and indirect viral inhibition through increasing antiviral gene expression.45 Nonetheless, despite these varied mechanisms, ribavirin appears to have a limited effect in treating disease in the normal host.46 This limited benefit is compounded by risks associated with aerosolized administration including bronchospasm, dyspnea, and chest pain. Furthermore, risk even extends to family and healthcare workers where headache and vomiting can occur. Moreover, animal studies prompted concern for possible teratogenicity, though this has not been demonstrated in humans.40 More recent research suggests a possible role for ribavirin in highly immunocompromised hosts (eg, bone marrow transplant recipients) but only at early stages of infection to prevent progression to LRTD and data is lacking in children.47 Additional studies now show that oral ribavirin has similar efficacy to aerosolized, significantly easing administration and decreasing cost.40
Several other RSV-specific therapies have been attempted, all with limited success. Among these is small interfering RNA, which work through silencing viral messenger RNA. It showed initial promise in reducing complications following RSV in lung transplant recipients, but follow-up research failed to replicate this effect.48 Similarly, the RSV fusion inhibitor, presatovir, did not affect viral load or lower respiratory tract complication in hematopoietic stem cell transplant patients.49 Lumicitimab, an oral nucleoside inhibitor, failed to advance beyond phase 2b due to lack of efficacy.50
Immunoglobulins are broadly used for prophylaxis against RSV bronchiolitis. Due to the stymied development of RSV vaccines, immunoglobulins were explored as passive prophylaxis to neutralize viral particles prior to infection. Among these, the first to be approved was respiratory syncytial virus immune globulin intravenous (RSV-IVIG)—a polyclonal antibody preparation derived from human donors with high neutralizing antibody titers.51 As research identified the F protein as critical for a protective immune response, a monoclonal antibody against the postfusion F protein, palivizumab, was developed. Both medications were expensive and limited in efficacy for treatment. RSV-IVIG was supplanted by palivizumab, which remains restricted to select high-risk patients.52 Palivizumab, and later motavizumab, which was derived from palivizumab but never approved for use, have been trialed for the treatment of RSV disease. However, a 2023 Cochrane review found no benefit for the use of immunoglobulins for patients with active disease.53
Palivizumab became the mainstay of RSV prevention from 1998 until recent recommendations prioritized the use of nirsevimab.54 The medication was initially recommended based on a large, randomized trial in high-risk infants that demonstrated a 55% reduction in RSV-related hospitalizations.55 Although, the definition of high-risk individuals was broadened in subsequent guidelines, palivizumab was not recommended for use in most newborns.56 The cost, monthly dosing requirement during the RSV season (up to 5 months), and difficulties predicting RSV circulation especially following the pandemic were all major determinants in transitioning away from palivizumab.
Recognition of the immunogenicity of the prefusion form of the F protein prompted development of the monoclonal antibody, nirsevimab.13 Nirsevimab has been demonstrated to be efficacious in reducing medically attended RSV (defined as a positive RSV test result with clinical findings and symptoms of respiratory disease) by 79%, hospitalization due to RSV by 80.6%, and RSV lower respiratory tract infection associated with ICU admission by 90%.54 Additionally, this antibody was modified to provide an extended half-life allowing for single-dose protection for an entire season. Of note, the initial nirsevimab study was conducted prepandemic when RSV circulation was “normal,” which may skew the efficacy results to appear more impressive. Still, nirsevimab was approved by the CDC ACIP in 2023 for all infants under the age of 8 months entering their first RSV season and for at-risk children aged 8 to 19 months entering their second RSV season. It is currently recommended that all children born between October through March receive nirsevimab within 1 week of birth if the mother did not receive the maternal RSV immunization.54 To expand coverage, nirsevimab was added to the CDC Vaccines for Children program and placed on the child immunization schedule in 2023. Early reports of use are promising with an estimated 90% effectiveness in preventing infant hospitalization during its first season of use.57
CONCLUSION
RSV continues to be a formidable pathogen for infants and young children. While select RSV vaccines have exhibited encouraging outcomes in adults and by way of maternal immunization, challenges remain in developing a safe and effective vaccine that provides long-lasting protection in the youngest age groups who remain vulnerable to severe RSV infection. The overall limited efficacy of RSV treatments is also noteworthy. Supportive care remains the mainstay of treatment for all children. Still, recent advances in prevention of disease have the potential to substantially change the impact of this pathogen.
DISCLOSURES
Dr. Negi reports no relevant financial relationships which, in the context of their contribution, could be perceived as a potential conflict of interest; Dr. Shabab has disclosed teaching and speaking for Moderna; Dr. Esper has disclosed being an advisor or review panel participant for Procter & Gamble.
- Copyright © 2024 The Cleveland Clinic Foundation. All Rights Reserved.
![]()
Clicking the link below will connect you to begin the credit-claiming process for CME . After clicking on the link, scroll to the bottom of the page and click on “Complete the CME Process.” You will need your myCME login information to access this.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.