


ABSTRACT
Insomnia is a common and challenging complaint in older adults (> 65 years) because of age-related alterations in sleep physiology. Cognitive behavioral therapy for insomnia is the gold standard for treatment of insomnia in young as well as older patients. Both clinicians and patients often prefer the simplicity of medication, but risks associated with some hypnotics increase with age. Pharmacologic options for older adults include low-dose doxepin, melatonin, ramelteon, and the dual orexin receptor antagonists. A well-informed clinician can help patients navigate the risks and benefits of both pharmacologic and behavioral options.
The need for sleep does not decrease with age, but changes in sleep physiology and architecture may make it more difficult to get adequate sleep.
Cognitive behavioral therapy for insomnia is the gold standard for treating insomnia in all populations, but it is time-intensive and does not offer immediate results.
Many medications used to treat insomnia do not have regulatory approval and have little evidence to support their use.
Doxepin, melatonin enhancers, and dual orexin receptor antagonists may be relatively safe alternatives to benzodiazepines and Z-drugs (zaleplon, eszopiclone, zolpidem, and others) and have evidence to support their use in older adults.
Sleep, a physiologic process, is vital to overall health.1 The National Sleep Foundation advises that adults 65 and older get 7 to 8 hours of sleep daily—a recommendation based on data that suggest older adults who sleep from 6 to 9 hours daily have better health, quality of life, and cognition compared with older adults who have other sleep durations.2
This article reviews the physiology of sleep and considers the benefits and hazards of pharmacologic and nonpharmacologic treatment options in older patients.
INSOMNIA DEFINED
Insomnia is a disturbance in sleep continuity associated with sleepiness, fatigue, headaches, and other somatic symptoms, as well as concerns about compromised cognitive or occupational functioning and mood disturbance. Insomnia occurs in up to one-third of the adult population worldwide3 and is associated with increased risk of cardiovascular disease, depression, and neurocognitive impairment.4,5 As many as 50% of older adults may have difficulty initiating or maintaining sleep, and 12% to 20% meet criteria for insomnia disorder.6 A clinical diagnosis of insomnia is justified if difficulty sleeping occurs at least 3 times a week for at least 3 months and causes daytime impairments such as fatigue, irritability, and cognitive dysfunction.5,7
NORMAL ADULT CIRCADIAN RHYTHM AND SLEEP PHYSIOLOGY
Circadian rhythms oscillate over about 24 hours and impact physiologic processes, including the sleep-wake cycle. Circadian rhythm is modulated by the light-dark cycle and the 24-hour clock time of the environment via external stimuli, termed zeitgebers (German for “time-givers”). Examples of zeitgebers include light exposure, social endeavors, and exercise. The suprachiasmatic nucleus in the anterior hypothalamus is a key regulator of circadian rhythm homeostasis.8 Light striking the retinal ganglion cells is relayed to the suprachiasmatic nucleus, which then inhibits secretion of melatonin from the pineal gland.8,9 As light fades at the end of the day, a progressive increase in melatonin levels leads to the onset of evening sleepiness.9
Neural circuits also regulate wakefulness and sleep. These wake- and sleep-promoting neurons compete for network dominance, creating a “switch” between wakefulness and sleep.
Wake-promoting neurons include noradrenergic neurons in the locus coeruleus, serotonergic neurons in the raphe nuclei, histaminergic neurons in the tubero-mammillary nucleus, and hypocretin (also known as orexin) -producing neurons of the perifornical nuclei in the lateral hypothalamic area.10 The hypocretin system also initiates arousal and, more important, inhibits rapid eye movement (REM) sleep.11
Sleep-promoting neurons work to keep us asleep. These include the melanin-concentrating hormone-producing neurons in the diencephalon and the gamma aminobutyric acid–producing neurons in the ventrolateral preoptic nuclei (also known as the intermediate nuclei of the preoptic area), median preoptic nuclei, and brainstem parafacial zone.10
Initiation of sleep is mediated in part by adenosine neurotransmission. Extracellular adenosine increases throughout the day, with rising levels activating the sleep-promoting neurons and serving as a “switch” to signal sleep.12
REM and non-REM sleep
Sleep is a rhythmic and cyclic process that alternates between 3 stages of non-REM (NREM) and REM sleep.12 This alternation and cycling is known as sleep architecture; a good night’s sleep includes 4 to 5 cycles. Each cycle lasts about 90 minutes and ends with an episode of REM sleep. NREM sleep is divided into stages NREM1, NREM2, and NREM36,12:
Stage NREM1 is light sleep when arousal is very easy
Stage NREM2 is characterized by slower brain waves, deeper sleep, lower body temperature, and lower heart rate (sleep spindles and K-complexes appear in electroencephalogram tracings during stage NREM2)6
Stage NREM3 is deep sleep, also known as slow-wave or delta sleep,6,12 during which tissue repair and immune strengthening are thought to occur6
REM sleep, which follows stage NREM3, predominates during the second half of the night and is characterized by dreaming and muscle atonia; it is thought that much of memory consolidation occurs during REM sleep.6,12
Normal age-related changes
In healthy people, melatonin is secreted only in the evening, with higher serum levels in young people than in older adults.9 Aging is associated with circadian rhythm changes, with the main change being phase advance, in which older adults have an earlier onset of sleepiness in the evening and earlier morning awakening. Psychosocial factors also may impact sleep, with effects on sleep hygiene and zeitgebers. Older adults, who may no longer have regular schedules and may be socially isolated, may be more prone to irregular bedtimes, increased napping, and poor sleep habits. Similarly, the lack of schedule and isolation may limit exposure to natural zeitgebers, such as light and social activities.2
Total sleep time declines in older adults, as does the amount of time spent in slow-wave NREM3 and REM sleep—phases that are associated with cognitive recovery and enhanced memory and learning.2 Older adults wake up more often after sleep onset, resulting in increased time awake, but usually do not have greater difficulty falling back asleep. It also takes older adults more time than younger people to fall asleep initially, referred to as sleep latency. Finally, there is decreased sleep efficiency, or the percentage of time spent asleep while in bed.
Most of these changes plateau at age 60. Sleep efficiency, however, continues to decline after age 90. This is clinically significant because declining sleep efficiency is associated with greater morbidity.2 The need for sleep does not decrease with age, but the changes in sleep physiology and architecture—especially the decline in sleep efficiency—may make it more difficult to get adequate sleep.2
SCREENING AND EVALUATION OF INSOMNIA
Patients who are symptomatic should maintain a sleep diary for 1 to 2 weeks8 with a daily record of the time they go to bed, approximate time they fall asleep, wake-up time, time they get out of bed, and any naps. Patients also should record any use of caffeine, alcohol, prescription medications, or illicit drugs, and report on whether they use electronic devices or engage in stimulating activities before bed.6 A medication review is important, as many antidepressants, antihypertensives, sedatives, antihistamines, and steroids can interfere with sleep.6 Patients should be asked about daytime fatigue and level of alertness.3
Before starting treatment of presumed insomnia, a thorough review of systems is indicated to rule out other conditions that may contribute to insomnia, such as sleep apnea, untreated psychiatric illness, endocrine disorders, neurologic disorders, chronic obstructive pulmonary disease, asthma, heart failure, and gastroesophageal reflux disease.6 Any positive findings should be addressed or a referral for further evaluation should be made. If no underlying factors are uncovered or if insomnia persists after treatment of causative conditions, then treatment of presumed primary insomnia can be initiated.6
PHARMACOLOGIC TREATMENT
Ideally, medication should be reserved for patients for whom cognitive behavioral therapy for insomnia (CBTI) fails.13 Despite the established efficacy and safety of CBTI, both clinicians and patients may prefer the “quick fix” of medication.14 Many commonly used medications have significant risks and little established efficacy.15 Hypnotics must be used sparingly in older adults, and when used, prescribing them for a short duration and at the lowest effective dose is recommended.16
Benzodiazepines, Z-drugs, and antihistamines
Benzodiazepines have been used for several decades to treat insomnia.6,16 They are effective for short-term treatment of insomnia,6 but the American Geriatrics Society warns that older adults have increased sensitivity to adverse effects of benzodiazepines.13,15 Benzodiazepines, Z-drugs (zaleplon, eszopiclone, zolpidem, and others), and antihistamines such as diphenhydramine and chlorpheniramine are all included in the Beers Criteria list of medications that should be avoided or pose a higher risk in older adults.17 Benzodiazepines and Z-drugs are on the list because they increase the risk of cognitive problems, delirium, falls, accidents, and fractures. Longer-acting agents such as diazepam and chlordiazepoxide are concerning because of their slow metabolism and the consequent risk of accumulating toxic levels. Sedating antihistamine medications such as diphenhydramine have significant anticholinergic effects and are also contraindicated in older adults because of risk of falls and confusion.15
Nonetheless, many patients have been taking these medications for years and are reluctant to discontinue them.16 Given that patients also may resist CBTI because of the effort required,14 it is worthwhile to consider safer medication alternatives. These include sedating psychotropics (both antidepressants and antipsychotics), melatonin enhancers, and the dual orexin receptor agonists.
Antidepressants and antipsychotics
Clinicians have long taken advantage of the sedating effect of many psychotropics to treat insomnia. Unlike benzodiazepines and Z-drugs, psychotropics have few or no reinforcing properties or discontinuation effects. However, much use of psychotropics for insomnia has been off-label and has limited supportive evidence. Many psychotropic drugs have anticholinergic effects at higher doses, which raises cognitive concerns in older adults.18 A few are worth considering, however.
Doxepin is a tricyclic antidepressant that has high affinity for histaminergic (H1) receptors at low doses (< 10 mg), effectively acting as a selective H1 receptor antagonist.18 It is the only antidepressant with US Food and Drug Administration approval for insomnia. It is indicated (3- or 6-mg doses) for patients who have difficulty staying asleep or experience early-morning awakenings.6
A 12-week randomized, double-blind, placebo-controlled trial examined the effects of doxepin, 1 mg and 3 mg, in older persons with chronic insomnia.19 Participants were randomized to receive nightly treatment with doxepin, 1 mg or 3 mg, or placebo. The study found that doxepin at 1 mg and 3 mg resulted in significant and persistent improvements in most sleep variables. In addition, patients who took doxepin did not report any memory problems or complex sleep behaviors, and there was no significant difference in next-day residual sedation between either dose of doxepin and placebo. Anticholinergic effects were not present at the studied doses.
Subsequently, a systematic review of 9 randomized placebo-controlled trials investigated the hypnotic effects of doxepin.18 Three studies of low-dose (< 10 mg daily) doxepin in older populations (≥ 65 years) showed that it had a modest advantage over placebo for sleep maintenance and duration but not for sleep initiation. Headache and somnolence were common side effects. Higher doses should be avoided in older adults because of anticholinergic effects that may cause cognitive difficulties. The low-dose doxepin studies were industry sponsored, and the patented medication remains expensive.
Amitriptyline, another tricyclic antidepressant, that has been used off-label at low doses (10 to 25 mg) to treat insomnia. It is often used in patients with pain syndromes, where it may indirectly improve sleep by relieving pain. At these doses, it is mainly acting on histamine H1 receptors, although it likely has some serotonergic and cholinergic antagonism.20 At higher doses, anticholinergic effects are common and may include urinary retention, constipation, dry mouth, blurred vision, orthostatic hypotension, and confusion.15 There is little evidence of efficacy to support treatment with amitriptyline despite its common use.20
Trazodone is a serotonergic antidepressant that acts as an antagonist at serotonergic (5-HT2) and alpha-1 adrenergic receptors. Despite little evidence of efficacy,13 it is widely prescribed off label in the United States for sleep disorders.20 Studies have shown some efficacy for sleep latency and sleep efficiency that dissipate after a week.20 Common side effects include dizziness, cardiac arrhythmias, orthostatic hypotension, and, potentially, priapism.6
Mirtazapine, an antidepressant with strong 5-HT2 antagonism, few drug interactions, and appetite-stimulating properties, is often used to treat insomnia, particularly in patients with depression.6,21 Studies in adults (mean age 41 years) have shown improvement in sleep latency, sleep efficiency, and decreased awakenings after 2 weeks of treatment.6 Overall limited evidence of efficacy remains, however, and patients may become habituated to its sedative effects. It may be preferable to histaminergic drugs but is not recommended for treatment of insomnia in patients who do not have depression.6
Atypical antipsychotics, particularly quetiapine and olanzapine, have been widely used to treat insomnia despite little controlled trial evidence. Antipsychotics may cause metabolic side effects, extrapyramidal symptoms, and tardive dyskinesia.20 In older adults, they carry an increased risk of stroke and sudden cardiac death.15 Given these potential effects, antipsychotics should not be used to treat insomnia in the absence of a primary indication such as psychosis.20
Melatonin and melatonin agonists
Melatonin and ramelteon enhance the melatonin system.3 Intrinsic production of melatonin decreases with age—hence the rationale for using melatonin-enhancing medications to treat insomnia.6 In the United States, melatonin is available over the counter and unregulated.9 In Europe, a 2-mg prolonged-release formulation of melatonin is approved for insomnia in older adults.6
Ramelteon (8 mg), a melatonin receptor agonist of MT1 and MT2 (G protein–coupled receptors that mediate the effects of melatonin), is approved for treatment of insomnia with sleep-onset difficulty. A European meta-analysis found that both melatonin prolonged release and ramelteon are more efficacious than placebo for insomnia symptoms in adults.22 Their overall clinical impact is modest, but a subgroup analysis suggested that these medications have large effect sizes in older adults.
Additional efforts to examine the effect of these agents in older populations found that patients receiving melatonin prolonged release or ramelteon fell asleep about 14 minutes earlier than those receiving placebo.23 Patients who received melatonin or ramelteon also had an increase in total sleep time (21 minutes) relative to placebo. The authors concluded that melatonin or ramelteon given to older persons with insomnia improved objective total sleep time, sleep latency, and subjective sleep quality. Frequent side effects included somnolence, dizziness, fatigue, and headache. There was no significant rebound insomnia after discontinuation.
Melatonin or ramelteon (8 mg) may be an alternative treatment option for older adults, given their good tolerability and at least some demonstrated efficacy.
Dual orexin receptor antagonists
Dual orexin receptor antagonists, a newer class of medications for insomnia, target the orexin system. Orexin is thought to be part of the neuronal system that promotes wakefulness, and thus blocking orexin 1 and 2 is believed to inhibit the wake drive.3 Three dual orexin receptor antagonists are approved by the US Food and Drug Administration: suvorexant, lemborexant, and daridorexant.
Suvorexant 30 mg for patients 65 and older (40 mg for those < 65) was compared with placebo in a randomized, placebo-controlled trial, which showed significant improvement in subjective total sleep time and subjective time to sleep onset during the first month in the suvorexant group over placebo.24 These improvements persisted during the 1-year phase of the trial completed by approximately 62% of participants who received suvorexant.
The most common adverse events were daytime somnolence, fatigue, and dry mouth. Serious adverse effects, occurring in 5% of the sample, included sleep paralysis, hypnagogic hallucinations, cataplexy, and suicidal ideation. Overall, suvorexant was safe and effective for most patients during the 1-year trial.
Lemborexant was compared with placebo or zolpidem in older adults.25 In a 1-month randomized, double-blind, placebo-controlled trial, lemborexant 5 mg and 10 mg significantly improved sleep latency and efficiency relative to placebo in adults 55 and older. Lemborexant 5 mg did not differ from placebo on cognitive performance and caused less postural instability than zolpidem in both doses. Lemborexant also effectively reduced wakefulness after sleep onset and had significantly less risk of postural instability compared with zolpidem. It was not associated with residual morning sleepiness or reduced functioning, but given its long half-life, this remains a theoretical concern.
Daridorexant is approved in 25- and 50-mg doses. It has been shown to produce significant improvement in sleep parameters compared with placebo at 1 and 3 months, with improved daytime functioning.26 It has also shown good tolerability in older adults. Daridorexant has the shortest half-life of the available dual orexin receptor antagonists (8 hours compared with 12 hours for suvorexant and 17 to 19 hours for lemborexant), which in theory may reduce risk for impaired next-day functioning.
Numbers needed to treat (NNT) and numbers needed to harm (NNH) for dual orexin receptor antagonists have been calculated as follows:
Suvorexant: NNT = 8, NNH = 1327
Lemborexant: NNT = 3, NNH ≥ 1028
Daridorexant 50 mg: NNT < 10, NNH = 78.29
These studies suggest good efficacy with low risk of harm.27–29 Dual orexin receptor antagonists may be a safer and more effective long-term option than other pharmacologic products,26 but as these medications remain patented, cost and insurance coverage may be limitations.30
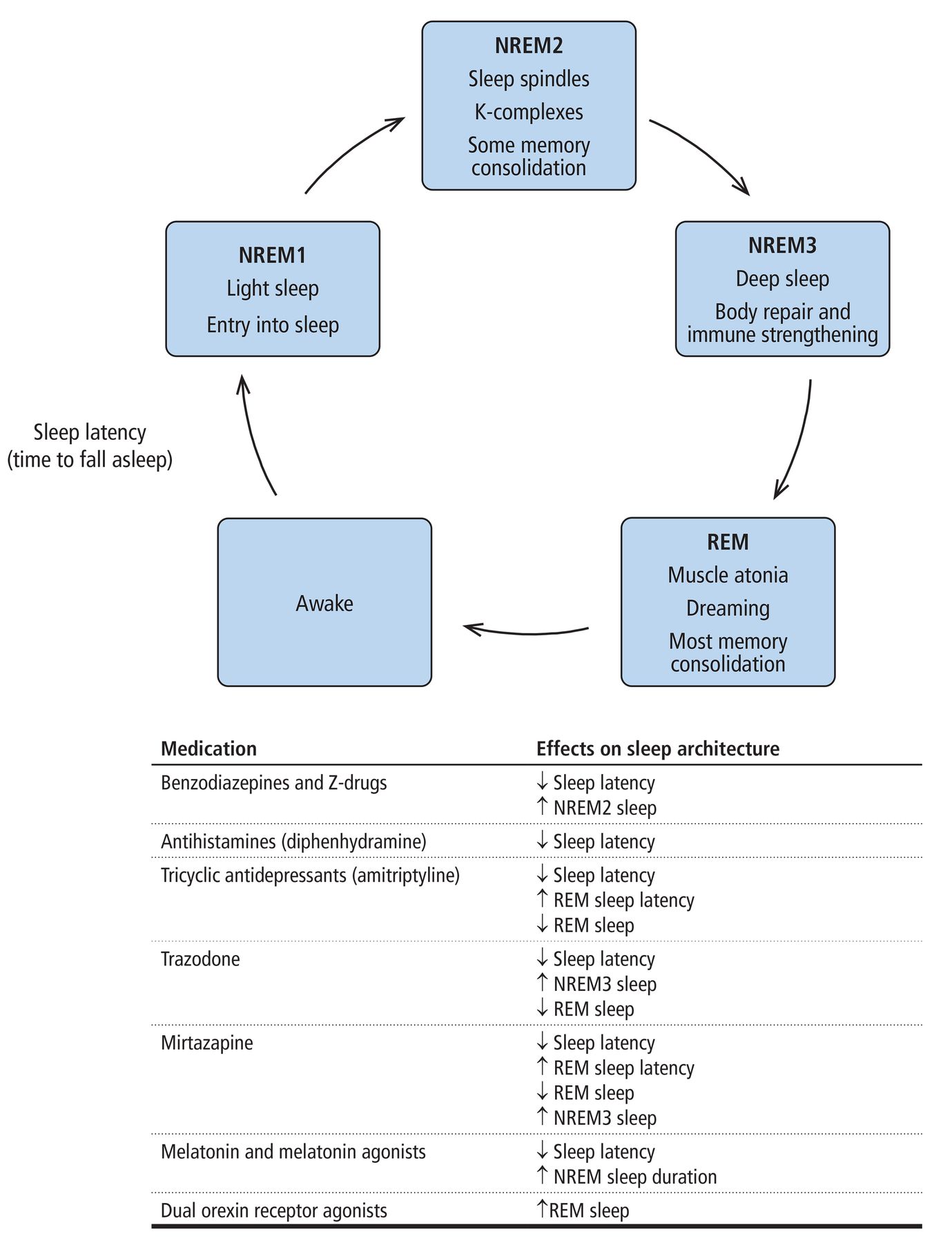
Figure 1 summarizes the effects of medications on sleep and sleep architecture.31

Sleep stage functions and medication effects on sleep architecture.
NREM = nonrapid eye movement; REM = rapid eye movement; Z drugs = zaleplon, eszopiclone, zolpidem, and others
Based on information from reference 31.
CANNABINOID COMPOUNDS
Evolving research suggests that cannabidiol may have therapeutic potential for insomnia treatment. Cannabidiol is one of the psychoactive components of cannabis (marijuana). The other, tetrahydrocannabinol, or THC, is thought to account for most of the euphoric effect of marijuana. Despite mixed results of research on cannabis and insomnia, it is generally accepted that tetrahydrocannabinol may lead to tolerance and disruption of the sleep cycle, while cannabidiol seems to have a positive effect on total sleep time and awakening after sleep onset.32
Cannabidiol appears to be well tolerated by older patients, with infrequent (< 15%) reports of mild adverse effects such as dizziness, tinnitus, and dry mouth.33 A recent small placebo-controlled study using 150 mg of cannabidiol showed improvement in sleep efficiency and subjective well-being, but not in other sleep parameters.34 Further research is needed to determine whether cannabidiol has a true benefit for insomnia treatment.
NONPHARMACOLOGIC TREATMENT
CBTI is recognized as the gold standard and first-line treatment for insomnia in young as well as aging patients.14,35 It has established efficacy, safety, and durability compared with pharmacologic treatments.14 Studies have shown a mean effect size with CBTI of 0.96 compared with 0.87 for pharmacotherapy.36 These results suggest a similar efficacy between treatments in the short term, but CBTI seems to have longer-lasting effects. The 2 therapies combined can improve some parameters, such as subjective sleep efficiency, but pharmacotherapy overall is not superior to CBTI alone.37 In the clinical setting, this suggests a ceiling effect past which adding more interventions to CBTI, such as pharmacotherapy, may not yield further benefit.
CBTI addresses maladaptive behaviors and cognitions that perpetuate insomnia. It incorporates psychoeducation, sleep hygiene, stimulus control, sleep restriction, relaxation training, and cognitive therapy techniques, such as cognitive restructuring. A course of CBTI generally takes 6 to 10 sessions delivered weekly or biweekly.13 Sleep diaries are used to establish a baseline, make behavioral interventions, and monitor treatment response.6
Sleep hygiene can promote healthy sleep. Interventions include no alcohol or caffeine before bed, no clock watching while in bed, no daytime naps, going to bed and getting up at the same time each day, and ensuring a room environment that promotes sleep.3,38
Stimulus control interventions strengthen the association between the bed and sleep. Typical instructions include going to bed only when sleepy, getting out of bed if not asleep in 15 to 20 minutes, and using the bed only for sleep and sex.3,38 This strategy is based on a model of insomnia suggesting that the development and maintenance of insomnia is a learned behavior. With more time spent in bed not sleeping, anxiety increases and promotes tension and frustration. Over time, the relationship between the bed and anxiety strengthens, leading to conditioned insomnia, and the bedroom becomes associated with wakefulness and frustration. The goal of stimulus control is to disrupt this coupling.3
Sleep restriction is a means of increasing sleep efficiency. Initially, patients limit time in bed to the approximate hours they have been sleeping and then gradually increase the time in bed as sleep efficiency improves.3,38 For example, if a patient’s average total sleep time is 5 hours and the average time in bed is 7 hours, the prescribed time in bed will be 7 hours. This “sleep window” must be followed each day irrespective of sleep quality. Sleep restriction may initially decrease total sleep time and increase daytime fatigue, but after several days it will lead to reduced sleep latency (time to fall asleep) and fewer nocturnal awakenings. As sleep efficiency increases, the sleep window increases—typically by 15 minutes each week—until the patient is getting an adequate amount of sleep each night.3
Sleep restriction has been studied as a single-component intervention in primary care settings. In a UK study, 642 patients were randomized to nurse-delivered sleep restriction therapy (combination of in-person and phone sessions) plus a sleep hygiene booklet or to a sleep hygiene booklet alone.39 At 6 months, the sleep restriction therapy group had medium to large sustained treatment effects for reduced insomnia severity compared with the sleep hygiene-only group. All participants were college-educated adults and there were no restrictions on usual care for either group, so results may not generalize to older populations. Relative contraindications to sleep restriction include pregnancy, bipolar disorder, seizure disorders, additional sleep disorders, shift work, and cognitive impairment.39
CBTI may challenge physicians and patients
People with insomnia often have thinking errors (such as, “I am never going to sleep again”) and nighttime worries that lead to autonomic hyperarousal and muscle or cognitive tension, all of which impair sleep.6,40 They may have pessimistic and unhelpful thoughts and beliefs about sleep, and also tend to have erratic sleep schedules and “take their worries to bed.” CBTI challenges dysfunctional beliefs about sleep, such as worrying about falling asleep or not getting enough sleep, and addresses maladaptive behaviors related to poor sleep.3,38 CBTI targets the person’s cognitive style as well as behavioral and hyperarousal factors associated with insomnia.3 Cognitive restructuring seeks to modify maladaptive beliefs about sleep (such as catastrophizing effects of a poor night’s sleep) and replace them with more helpful thinking.40
It is also helpful to teach patients relaxation strategies such as progressive muscle relaxation to decrease hyperarousal.6
Implementation of CBTI has challenges, as patients may resist participating or insist on medication. Another challenge may be lack of physician knowledge about CBTI. Research has shown that educating primary care physicians about CBTI results in clinically significant and sustained improvement in insomnia.14 Multiple effective apps and websites for patient-guided CBTI are available.16
BETTER STUDIES, BETTER OPTIONS
Natural sleep is regulated by a complex and delicate balance of multiple systems that is easily disturbed, especially in older adults. CBTI is a well-studied, safe, and efficacious treatment for insomnia in this age group. The drawbacks are that it is time-consuming to implement and not immediately effective. As sleep physiology is better understood, newly developed medications are providing safer alternatives, but they may be prohibitively expensive. Armed with a basic knowledge of sleep pathology, clinicians can consider the risks and benefits of both pharmacologic and behavioral options to safely restore sleep in the older adult population.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2025 The Cleveland Clinic Foundation. All Rights Reserved.
![]()
Clicking the link below will connect you to begin the credit-claiming process for CME and MOC. After clicking on the link, scroll to the bottom of the page and click on “Complete the CME/MOC Process.” You will need your myCME login information to access this.




{kind=link}