


Article Figures & Data
Figures
- Figure 1
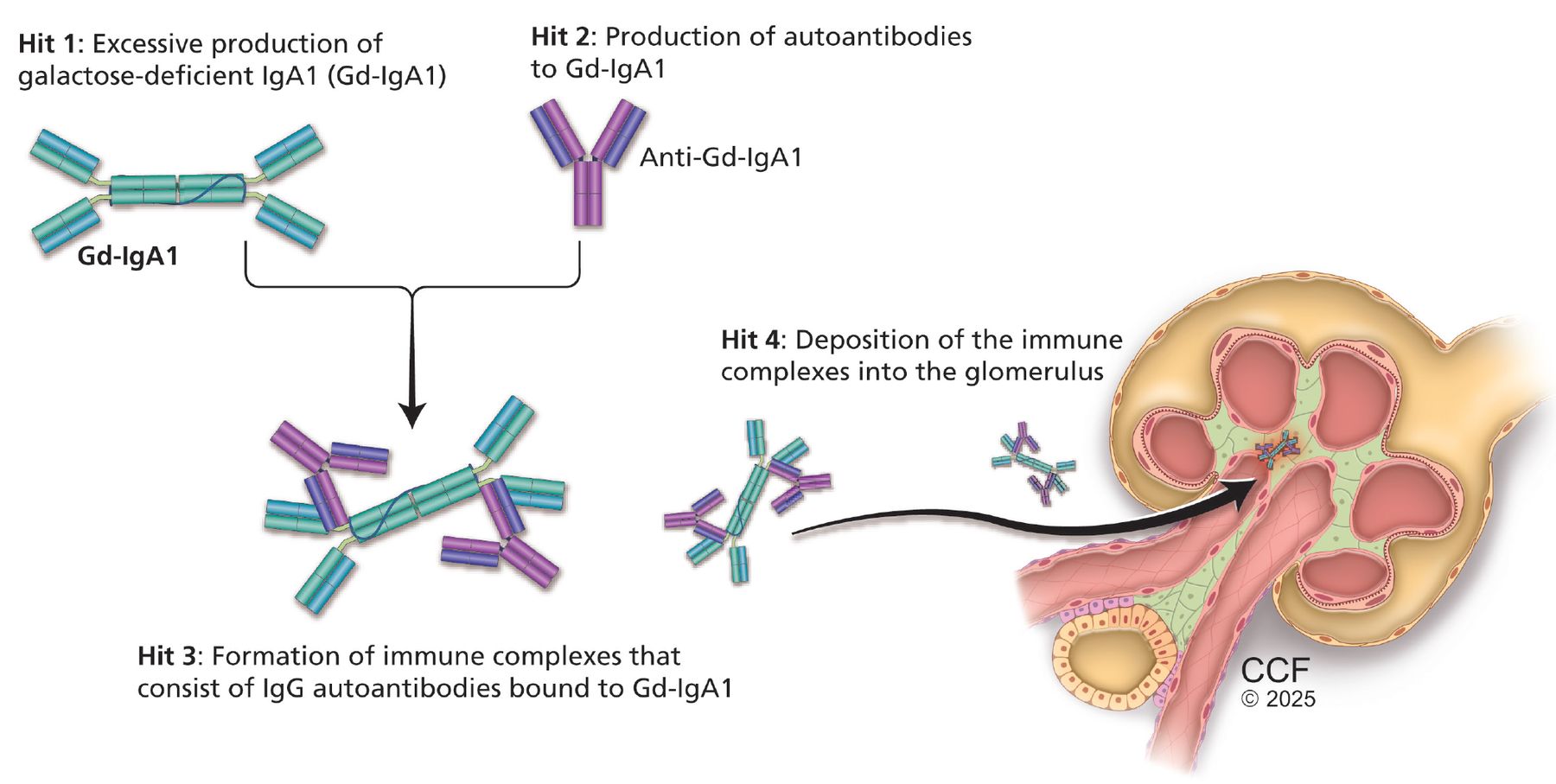
Pathogenesis of immunoglobulin (Ig) A nephropathy: the “4-hits” hypothesis.
- Figure 2
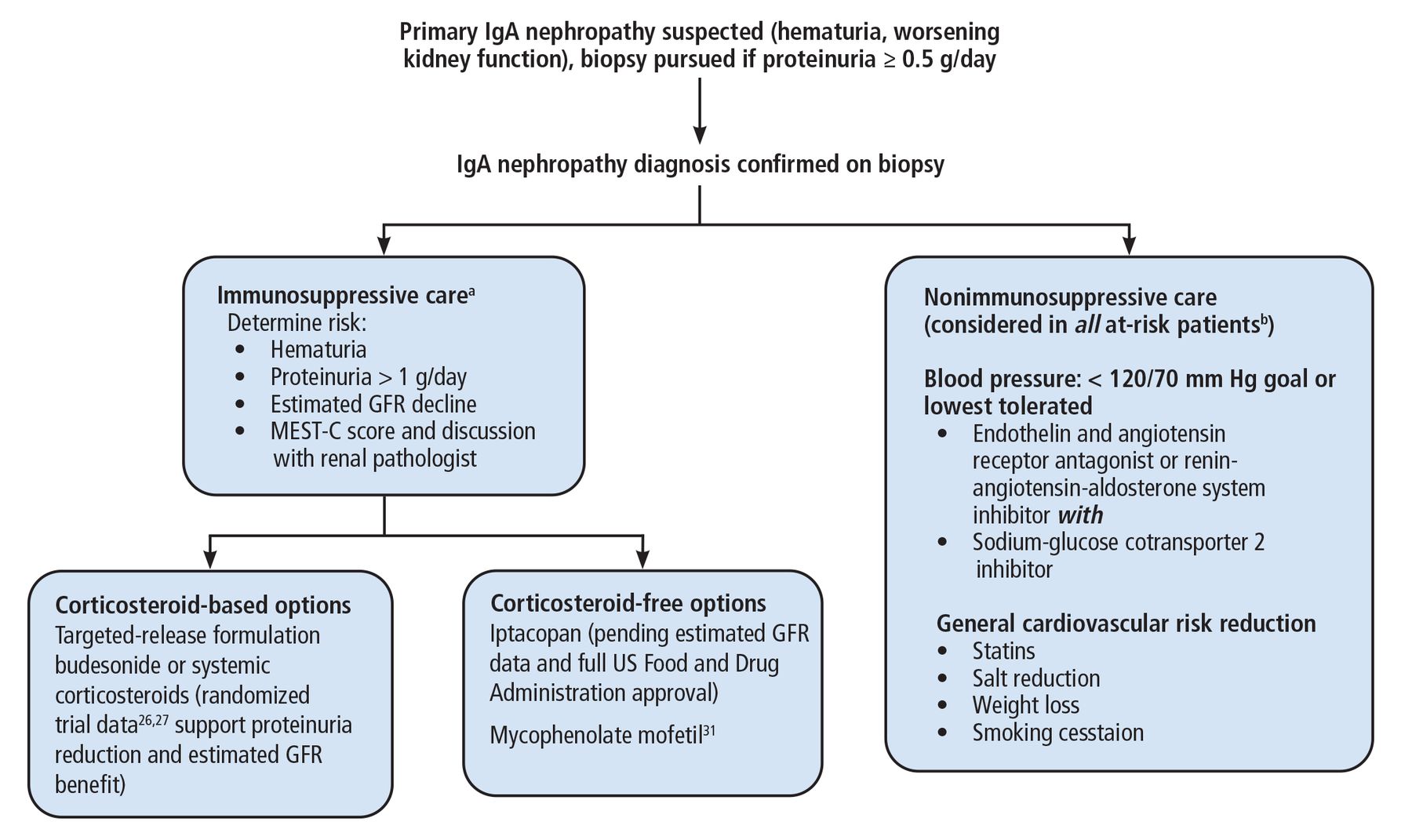
Our approach to immunoglobulin (Ig) A nephropathy.
aWe monitor patients receiving immunosuppressive therapy with assessment of blood pressure and protein-creatinine ratio, renal function panel, and urinalysis every 3 months.
bThose with proteinuria > 0.5 g/day.
GFR = glomerular filtration rate; MEST-C = mesangial hypercellularity, endocapillary proliferation, segmental glomerulosclerosis, tubulointerstitial fibrosis, crescents


Tables
IgA nephropathy1,12 Systemic IgA vasculitis1,12 IgA-dominant postinfectious glomerulonephritis13 Proliferative glomerulonephritis with monoclonal IgA deposits14 Clinical presentation Varied, can present with a range of clinical syndromes: microscopic hematuria (more common than macroscopic), acute kidney injury, rapidly progressive glomerulonephritis, macroscopic hematuria with concurrent respiratory or gastrointestinal infection (ie, synpharyngitic hematuria)
Involvement limited to kidneysMore common in children
Extrarenal involvement (leukocytoclastic vasculitis; rash; joint pain; gastrointestinal, pulmonary, neurologic involvement)Older adults, hypocomplementemia, acute kidney injury with hematuria and proteinuria Rare; involvement limited to kidneys Kidney biopsy Dominant mesangial IgA staining on immunofluorescence microscopy with variable IgG staining and frequent C3 staining; chunky, irregular mesangial IgA staining on immunofluorescence
Polyclonal light chain deposition with lambda more intense than kappaEndocapillary hypercellularity, often with neutrophils, on light microscopy
Dominant IgA staining with dominant or codominant C3 staining and absent or weak IgG staining; chunky, irregular mesangial IgA staining; lambda not dominant light chains on immunofluorescence microscopy
Subepithelial hump-shaped immune deposits on electron microscopyMembranoproliferative pattern on light microscopy
Monotypic light chain deposition of IgA kappa more intense than lambdaPathogenesis 4-hit model Unclear: likely a host-pathogen interaction with superantigens stimulating host T-cell response Unclear: rarely associated with malignancies despite monoclonal deposition of IgA Associations Primary and secondarya distinguished by presence of associated systemic disease Upper respiratory or gastrointestinal infection Staphylococcus aureus infection, diabetes Myeloma (rarely) ↵a Common secondary: liver disease, celiac disease, inflammatory bowel disease, viral (human immunodeficiency virus, hepatitis B and C), ankylosing spondylitis, rheumatoid arthritis, systemic lupus erythematosus, psoriasis, Sjögren syndrome, tumors (lung, renal, lymphoma).
Based on information from references 1,12–14.
Histologic feature Definition15,16 Prognosis Mesangial hypercellularity ≥ 4 mesangial cells in any mesangial area of a glomerulus
M0: < 50 glomeruli
M1: ≥ 50 glomeruliM1 is predictive of worse outcomes vs M015 Mesangial hypercellularity and endocapillary proliferation (hematoxylin and eosin stain, magnification ×400)

Endocapillary proliferation Increased number of cells in glomerular capillary lumen
E0: absent
E1: presentE1 is independently associated with worse renal survival in patients who receive no immunosuppression, and does not predict outcomes in studies where patients receive immunosuppression
Patients with endocapillary proliferation (E1) are more likely to receive immunosuppression, which is associated with improved outcomes in these patients16Segmental glomerulosclerosis Adhesion or sclerosis that does not involve the entire glomerulus
S0: absent
S1: presentS1 is predictive of worse outcomes compared with S015 Tubulointerstitial fibrosis Percentage of tubular atrophy and interstitial fibrosis of cortical area
T0: absent or ≤ 25% of tubules
T1: 26%–50% of tubules
T2: > 50% tubulesPresence of tubulointerstitial fibrosis (T1 or T2) is strongest predictor of adverse renal outcomes16 Crescent formation (periodic acid–Schiff stain, magnification ×400)
Crescents, cellular or fibrocellular Extracapillary cell proliferation > 2 cell layers and < 50% of matrix
C0: absent
C1: 1%–24% of glomeruli
C2: > 25% of glomeruliC1 is not predictive if immunosuppression is used
C2 is predictive of worse outcomes regardless of immunosuppression16Images courtesy of Leal Herlitz, MD, Cleveland Clinic Anatomic Pathology.
Drugs Status Recent approvals Endothelin and angiotensin receptor antagonist: sparsentan24
Endothelin receptor antagonist: atrasentan25
Corticosteroid: targeted-release formulation budesonide30
Complement inhibitor: iptacopan32,38Full approval
Accelerated approval
Full approval
AcceleratedFuture (not approved) treatment options Complement inhibitors33–35,37,39,40 Avacopan, ravulizumab, cemdisiran, vemircopan, pegcetacoplan
IONIS-Fb-LRx
Narsoplimab
RO7434656
ARO-C3Phase 2 and 3 trials in progress
Phase 3 trial in progress
Phase 3 negative trial
Phase 3 trial in progress
Phase 1 trial in progressB-cell–depleting therapies41–45 Atacicept
Sibeprenlimab, zigakibart, telitaciceptPhase 3 trial in progress
Phase 2 and 3 trials in progressPlasma cell inhibitors46,47 Felzartamab, mezagitamab, bortezomib Phase 2 trials in progress
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.