


A 66-year-old immunocompetent man presented with bulging and persistent burning pain in the right abdominal side for 4 days. Two days before the presentation, he went to another hospital and underwent abdominal computed tomography, which revealed no intraperitoneal abnormality.
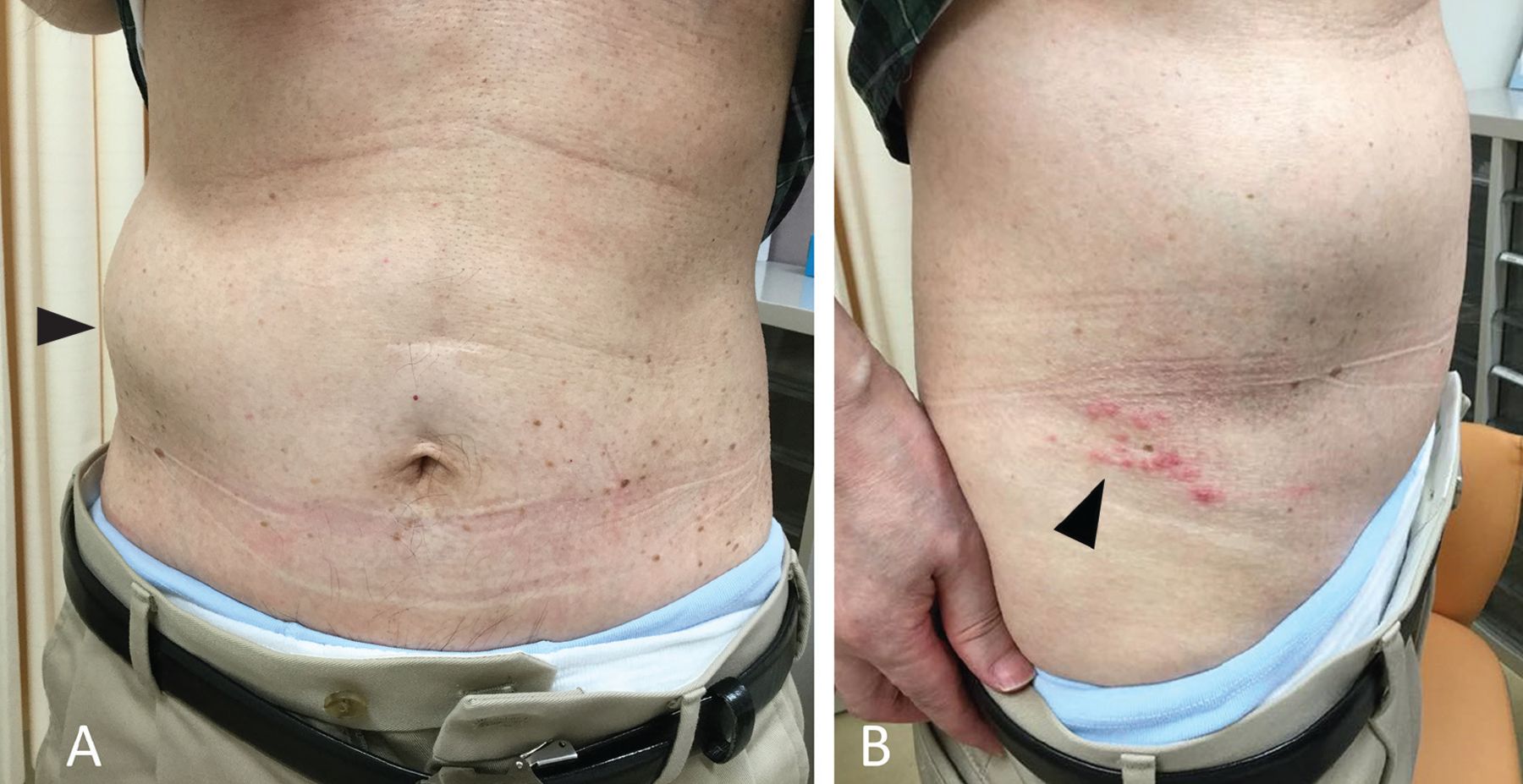
On examination, the bulge was soft and nontender and did not have any palpable mass (Figure 1A). Thermal hypoalgesia was detected by alcohol swab in a belt from the lower right side of the abdomen to the back, a neurologic finding suggestive of zoster infection. No other neurologic deficit was seen. However, there were papules aggregated above the right groin (Figure 1B). The patient had been unaware of this rash until it was pointed out. The rash was thus presumed to have developed on the morning of the presentation day because the patient confirmed that there was no skin change when taking a bath the previous night.
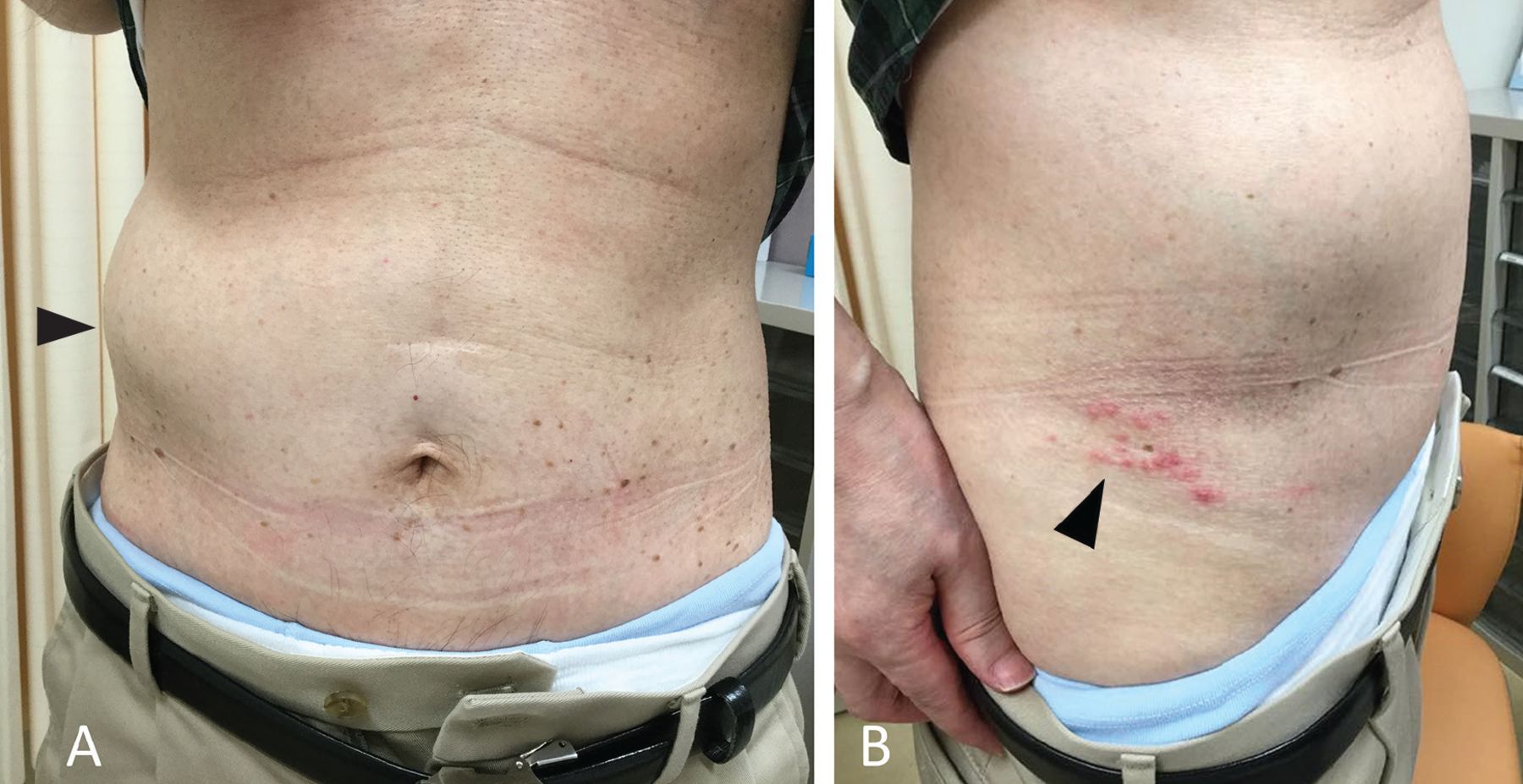
(A) Bulging of the right abdominal wall (arrowhead). (B) The papules aggregated in a row on the right side of the lower abdomen (arrowhead).
The diagnosis of abdominal pseudohernia due to herpes zoster was made based on the physical findings.
Lesions of herpes zoster often progress through stages, in the course of 7 to 10 days, from red macules and papules (as in this patient) to vesicles, to pustules and crusts,1 and then eventually subside spontaneously.2 Our patient was reassured that the condition would resolve on its own. He was prescribed valacyclovir 3,000 mg/day for 7 days. The bulging gradually improved over several weeks.
NEUROLOGIC COMPLICATIONS OF INFECTION
Although skin neuralgia is a well-known complication of herpes zoster, the varicella-zoster virus can also cause motor neuron deficits, probably because of direct spread into spinal anterior horn cells and ventral roots.3
When the virus affects the lower thoracic spine, unilateral abdominal bulging may occur because of paresis of abdominal muscle.4 Most cases subside spontaneously,2 and patients can be reassured and thus be spared unnecessary diagnostic tests or medications.
Causes of pseudohernia other than herpes include diabetic radiculoneuropathy; trauma, such as ventral root injury from tumor removal and prolapsed intravertebral disc; and infection, such as Lyme disease and poliomyelitis.5,6
KEYS TO THE DIAGNOSIS
There are several keys to the diagnosis of abdominal pseudohernia due to herpes zoster.
First, the physician should not rule it out simply because there is no rash. Although the condition is often termed postherpetic abdominal pseudohernia,3,4 the bulging precedes the herpetic rash in nearly 10% of patients.2 This is why I prefer the term abdominal pseudohernia due to herpes zoster.
Second, a targeted history is important, eg, to rule out tick exposure and Borrelia-related neurologic complications.7
Third, imaging tests including magnetic resonance imaging may be indicated to check for mechanical compression of thoracic nerve roots if close follow-up does not reveal delayed-onset herpetic rash.
The combination of unilateral bulging of the abdominal wall and herpetic rash indicates abdominal pseudohernia due to herpes zoster. The rash may develop after the bulging, and thus, close follow-up may be of benefit.
DISCLOSURES
The author reports no relevant financial relationships which, in the context of his contribution, could be perceived as a potential conflict of interest.
Acknowledgments
We thank Robert Blakytny, DPhil, from Edanz Group for editing a draft of this manuscript.
- Copyright © 2021 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}