


74 year-old woman presented to the hospital from the podiatry clinic for evaluation of bilateral foot pain and purple toes. She had a history of Janus kinase (JAK) 2 V617F–positive polycythemia vera, Raynaud syndrome, gastroesophageal reflux disease, prior breast cancer and thyroid cancer, hypertension, and deep vein thrombosis and pulmonary embolism. Her polycythemia vera had been treated with aspirin, which was discontinued due to stomach upset, and hydroxyurea, which was also recently discontinued. She was started on apixaban following her deep vein thrombosis and pulmonary embolism episode and was still taking it at the time she presented.
The patient reported that her symptoms began about 5 months earlier. At that time, she experienced intermittent burning foot pain, worsened by prolonged sitting and standing. She developed painful ulcers on her right hallux, described as “black dots” that expanded, and later developed additional ulcers on her left lateral ankle and right anterior shin. The ulcer on her left ankle was biopsied and found to be consistent with livedoid vasculopathy.
She was started on pentoxifylline and nifedipine, and hydroxyurea was discontinued due to concern that it was contributing to her ulcerations. The ulcers initially improved with wound care. However, about 3 weeks before her current presentation, her toes started to become purple, with persistent “stinging” pain that improved somewhat with warmth and elevation.
PHYSICAL EXAMINATION
On presentation, violaceous discoloration of both feet was noted, with necrotic tissue present distally (Figure 1). Her feet were cold to the touch, with palpable dorsalis pedis pulses bilaterally and intact sensation and strength. Cardiac examination was unremarkable, without murmurs, rubs, or gallops. Palpation of her abdomen did not reveal splenomegaly. No joint swelling, erythema, or tenderness to palpation was present.

Violaceous discoloration of patient’s toes on presentation.
DIFFERENTIAL DIAGNOSIS
1. What is the most likely diagnosis?
Livedoid vasculopathy
Critical limb ischemia
Microthrombi
Erythromelalgia
The differential diagnosis for purple digits is broad. In a hemodynamically stable patient, emergent etiologies include acute limb ischemia, embolic microthrombi, purpura fulminans,1 and catastrophic antiphospholipid syndrome (APS).2 Purple digits stem from abnormal blood flow, which can have various causes. These include microembolisms from upstream clots, large aneurysms, peripheral vascular disease, vasospasm, vasculitis and pseudovasculitis, thrombosis or mechanical obstruction, cryoglobulinemia, myeloproliferative syndromes, and hypercoagulability secondary to malignancies or hypercoagulable syndromes.1,2
Livedoid vasculopathy, and a "diagnostic time-out"
Livedoid vasculopathy, a thrombotic vasculopathy that is more common in females and presents with lower-extremity ulceration,3 was initially considered on the differential. However, the presence of abnormal findings of purple toes supporting a competing diagnosis such as microthrombi, diagnostic uncertainty, and unanticipated deviation from the expected ulcer treatment course prompted a “diagnostic time-out”4,5 to consider whether this patient’s presentation represented 1 process related to livedoid vasculopathy or 2 distinct processes.
Initially, the patient reported that the symptoms began 5 months previously. However, careful history revealed that her ulcers had been healing with the treatment for her livedoid vasculopathy, and the new symptoms of purple toes developed more recently. While livedoid vasculopathy presents with lower-extremity symptoms and burning, purple toes would be atypical. This prompted consideration of a separate process driving her current presentation or a unifying underlying condition tying these 2 distinct processes together.
Limb ischemia or microthrombi
One of the first branch points in the evaluation of purple digits is the presence or absence of a peripheral pulse. Acute arterial occlusion typically presents with the 5 “Ps”: pain, pallor, paresthesia, paralysis, and pulselessness.6 In this patient, palpable pulses, as well as intact strength and sensation, point away from acute limb ischemia requiring emergent evaluation and treatment. However, palpable pulses do not rule out embolic or thrombotic etiologies. Cholesterol embolization famously produces “blue toe syndrome,” and similarly microthrombi, commonly from endocardial vegetations or thrombi, block vessels distal to the dorsalis pedis, leading to ischemia with a palpable pulse. A cardiopulmonary examination can reveal murmurs pointing to endocarditis or valvular abnormalities as a potential source for showering thrombi or vegetations, and a vascular examination can reveal bounding pulses pointing to vascular aneurysms.
Erythromelalgia
Erythromelalgia is a complication of polycythemia vera that is thought to be mediated by a complex interplay of neural and vascular dysfunction involving arteriole-venule shunts7 and by platelet dysfunction.8,9 This disorder is marked by episodes of increased temperature, erythema, and burning pain in the extremities, and its symptoms are relieved by cooling of the extremity and limb elevation.7 Erythromelalgia was considered because the patient had been diagnosed with polycythemia vera but was not taking aspirin, which can improve symptoms or erythromelalgia,7 and because she reported symptom improvement with leg elevation, suggesting hyperviscosity. She discontinued taking aspirin due to intolerance and was started on apixaban. However, the patient’s report of symptom improvement with heat and her cold foot temperature made this diagnosis unlikely.
Other concerns
With concern for small-vessel ischemia, a paraneoplastic vasculitis separate from polycythemia vera–related JAK2-mediated thrombosis was considered, given her history of breast cancer and thyroid cancer (Table 1). An autoimmune vasculitis was also considered given her history of Raynaud disease. The patient showed no joint swelling or tenderness, suggesting no autoimmune involvement of the joints, but this did not rule out autoimmune conditions or vasculitis.
Details of the patient’s malignancy history
Of note, hydroxyurea, a rare cause of both ulceration10 and livedoid vasculopathy,11 had been stopped in this patient previously due to concern it was contributing to her leg ulcerations.
CASE CONTINUED: NOTABLE VASCULAR AND LABORATORY TESTING RESULTS
Laboratory test results were notable for hyponatremia to 126 mmol/L (reference range 132–148) and hypokalemia to 3.6 mmol/L (3.7–5.1). A pulse volume recording showing an ankle-brachial index (ie, the systolic blood pressure in the ankle divided by the higher of the systolic pressures in the 2 arms) of 1.08 on the right and 1.02 on the left (1–1.4). A complete blood cell count without differential showed the following:
White blood cell count 38.27 × 109/L (3.7–10.4)
Hemoglobin 12.9 g/dL (12.3–15.3)
Platelet count 323 × 109/L (150–400).
A differential the next day showed the following: white blood cell count 36 × 109/L, with 89% neutrophils (42–75), 4% lymphocytes (16–52), 1% monocytes (1–11), 2% eosinophils (0–7), and 1% basophils (0–4).
A partial workup for thrombophilia had been done when the patient developed lower-extremity ulcers, but full lupus anticoagulant testing was not completed at that time.
2. What aspect of this patient’s history or treatment would prevent full lupus anticoagulant testing?
Use of a direct oral anticoagulant (DOAC)
History of breast cancer
Polycythemia vera
Use of hydroxyurea
APS is an autoimmune condition in which the presence of antiphospholipid antibodies leads to thrombosis or obstetric complications.12 Clinical criteria include the presence of arterial, venous, or small-vessel thrombosis or obstetric complications, while laboratory criteria include the presence of antiphospholipid antibodies in plasma, namely lupus anticoagulant, anticardiolipin, or anti–beta-2-glycoprotein 1 antibodies.12,13
Full lupus anticoagulant testing could not be completed in this patient because she was taking apixaban. DOACs can affect APS laboratory assays, causing both false-positive and false-negative lupus anticoagulant findings,14,15 and different DOACs affect the assays differently.14 Other anticoagulants can also interfere with testing, but established neutralizers for heparin included in many reagents for the dilute Russell’s viper venom time, a common test for lupus anticoagulant, help mitigate this.14 Several strategies have been proposed to evaluate patients on DOACs for APS, including pausing DOAC, DOAC antagonists, and DOAC removal from the specimen,14,15 although these are not available in many laboratories.
Apart from guiding the diagnostic workup, her laboratory workup showed significant leukocytosis, hyponatremia, and hypokalemia. The leukocytosis was felt to be reactive, the hyponatremia was likely hypovolemic and improved with fluids, and potassium was repleted.
CASE CONTINUED: FURTHER MANAGEMENT
The partial laboratory workup was negative for anticardiolipin, anti–beta-2-glycoprotein 1 antibodies, and cryoglobulins, and positive for antinuclear antibody (1:640).
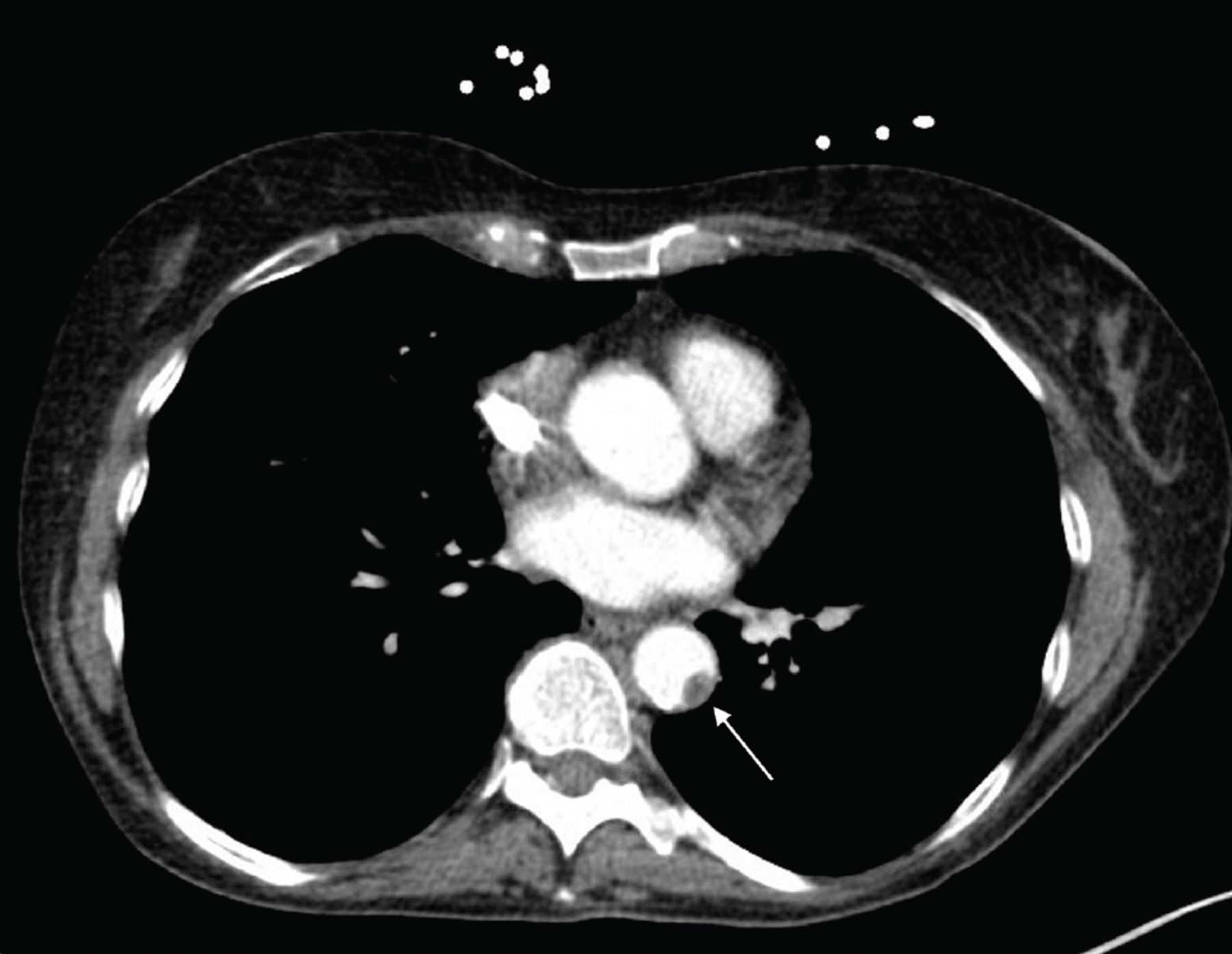
With thrombi on the differential, apixaban was discontinued, unfractionated heparin was begun, and an echocardiogram was ordered. Given her history of Raynaud disease and concern for vasoconstriction, nifedipine, which had been started as part of her treatment for livedoid vasculopathy, was continued, and nitroglycerin topical ointment was ordered for treatment of the digital ulcers. To evaluate for neoplastic syndrome, a computed tomography imaging of the chest, abdomen, and pelvis was obtained and showed an 8-mm thrombus (Figure 2).

Computed tomography scan showing aortic thrombus.
3. What is the most likely location of this patient’s thrombus?
Bilateral proximal deep veins of the left and right lower extremity
Central clot in the inferior vena cava
Aorta
Carotid artery
The presence of bilateral symptoms from thromboembolic disease implies either bilateral thrombi or a central arterial thromboembolic source. Venous thrombi would propagate towards the heart, not distally. The central arterial source is most commonly the heart, where structural or functional abnormalities can cause clot to form, and thus an echocardiogram is an essential part of the evaluation for arterial thrombi,16,17 even when, as in this patient, the cardiac examination revealed no murmurs or other abnormalities.
Thrombi within or proximal to the heart can embolize anywhere in the body, while more distal thrombi have fewer potential locations.17 A thrombus in the carotid arteries would be more likely to embolize to the brain than to the lower extremities.17 A rare but serious cause of peripheral embolism is mural thrombus in the aorta.16,18
THROMBOEMBOLIC DISEASE IN POLYCYTHEMIA VERA
The clinical question now centers on the development of a substantial thrombus in a patient taking apixaban and its management.
The patient was initially started on anticoagulation after she developed a deep vein thrombosis and pulmonary embolism in the setting of polycythemia vera. Thrombosis is a common complication of polycythemia vera, with an estimated incidence of 26% in patients followed for 20 years.19 Most thrombotic events occur early in the disease course, often preceding diagnosis.20 Interestingly, this patient’s thrombotic event occurred years after her initial polycythemia vera diagnosis. The JAK2 V617F mutation is a strong independent risk factor for thrombosis through multifactorial mechanisms, including overexpression of procoagulant factors and platelet and endothelial cell dysfunction.21
There is no clear consensus on the use of vitamin K agonists such as warfarin vs DOACs in patients with polycythemia vera and other myeloproliferative disorders,19 although there is a greater quantity of evidence for vitamin K agonists.21 The limited number of head-to-head studies comparing vitamin K agonists with DOACs in myeloproliferative disorders show similar outcomes, with some slightly favoring DOACs.21
While oral anticoagulation reduces both arterial and venous thrombus risk in patients with polycythemia vera, it is not as protective against arterial thrombus, which is mediated partially by platelet and endothelial dysfunction. Low-dose aspirin is typically used for primary prevention of thrombotic events, including arterial clots, in patients with polycythemia vera.19 The patient had been taking aspirin before she started apixaban for deep vein thrombosis or pulmonary embolism, at which point it was discontinued because of poor tolerance. It is unclear whether aspirin has an added benefit in patients with polycythemia vera on DOACs or merely increases bleeding risk without significant additional protection from thrombosis.19,21 Further studies are needed.
This patient potentially had risk factors for thrombosis apart from polycythemia vera. She had undergone a partial workup for APS in the past, but a full workup was needed at this point, especially in the context of her developing thrombosis while taking apixaban.
CASE CONTINUED: RHEUMATOLOGY REFERRAL
The 8-mm thrombus identified on computed tomography was located in the mid-descending thoracic aorta. Similar thrombus was noted in the abdominal aorta close to the bifurcation, and splenic infarcts were noted as well. Echocardiography showed normal systolic and diastolic function and no thrombi or vegetations.
Rheumatology was consulted because of concern for an underlying autoimmune condition, noting the patient’s high antinuclear antibody titer, lack of other clinical symptoms of systemic rheumatic disease, negative cryoglobulins, and no clinical or laboratory features of small-vessel vasculitis (Table 2). Rheumatology recommended an APS workup, which was positive for lupus anticoagulant. Vascular medicine recommended repeat lupus anticoagulant testing in 12 weeks.
Details of rheumatology consult clinical reasoning
ANTICOAGULATION IN APS
4. What is the preferred anticoagulant agent for APS?
DOAC
Warfarin
Aspirin alone
Clopidogrel alone
Two factors in the current presentation could disrupt testing: use of heparin and the presence of active thrombosis. While heparin can be neutralized by specific reagents during lupus anticoagulant testing, heparin levels can exceed the neutralizing ability, and these reagents are not usually present in activated partial thromboplastin time reagents.14 Thus, results obtained in this clinical context should be interpreted with caution and repeated in the coming weeks, as recommended by vascular medicine.
APS is associated with a characteristic netlike “livedo” rash, which can be further classified into livedo reticularis and livedo racemosa.22 Both are caused by reduced blood flow, but livedo racemosa is more widely distributed on the trunk and the limbs, is irregular and broken in shape, has abnormal histopathology findings, is always pathologic, and is associated with APS and several other diseases. Although this patient’s skin findings were not characteristic of livedo, with violaceous digits rather than a net-like violaceous pattern, her APS adds further evidence for increased thrombotic risk.
In APS, positive lupus anticoagulant is associated with a high risk for thrombosis.23 The presence of anticardiolipin and anti–beta-2-glycoprotein 1 antibodies may convey additional risk, and some guidelines define a “high-risk” APS profile as the presence of lupus anticoagulant, presence of double-positive antibodies with or without lupus anticoagulant, triple-positive antibodies, or high antibody titers.24
Patients with APS with arterial thrombosis typically are treated more aggressively than those with venous thrombosis.23 Current data show the risk of arterial thrombosis recurrence is lowest for patients on warfarin in combination with antiplatelet therapy, with some data, including a systematic review of 12 cohort studies and 4 randomized controlled trials, showing that international normalized ratio (INR) targets greater than 3 were associated with a lower risk of recurrence in patients with arterial thrombosis.25 However, the risk of bleeding with the addition of an antiplatelet agent, oral anticoagulation, or a higher INR target must be weighed against the risk of recurrent arterial thrombosis, especially in the context of studies showing no benefit of high-intensity warfarin in APS for venous thrombus.23
The question of vitamin K agonists vs DOACs for APS is more clear-cut than for myeloproliferative disorder, with evidence favoring the former.19,23 It is important to distinguish between low- and high-risk APS profiles when interpreting studies comparing DOACs vs vitamin K agonists, as some studies showing no differences in venous thrombosis outcomes are limited by underrepresentation of patients with a high-risk APS profile.24
Interestingly, in the 2018 Trial on Rivaroxaban in Antiphospholipid Syndrome (TRAPS)26 comparing warfarin with rivaroxaban in patients with triple-positive APS, recurrent thromboses were seen more often in the rivaroxaban group and were largely arterial. Our patient likely would have been placed on warfarin had her APS diagnosis been established at the time of the initial venous thromboembolism event. Her treatment with apixaban was less protective against future thrombotic events, particularly arterial thrombosis, although it is important to note that the studies done used rivaroxaban, not apixaban. Further, there is a dearth of studies examining use of DOACs specifically for arterial thrombosis in patients with APS.
CASE CONCLUDED
Vascular medicine recommended an intravenous heparin drip for 72 hours with a target activated partial thromboplastin time of 53 to 78 seconds, with a plan to transition to therapeutic enoxaparin 1 mg/kg twice daily for 4 weeks, followed by a bridge to warfarin with a target INR of 2 to 3 and clopidogrel. The patient’s burning bilateral foot pain continued despite the heparin therapy. She underwent aortography with suction thrombectomy of her infrarenal aortic thrombus, after which her pain improved, and she was discharged.
In patients with a descending thoracic aortic thrombus, the initial treatment strategy is typically conservative, with anticoagulation, sometimes anti-platelet agents and, rarely, thrombolytic therapy. Typically, endovascular treatments such as thrombectomy or surgical treatments are used in cases where conservative measures fail, as in this patient, although thrombus size and mobility and diagnostic uncertainty may lead to initially pursuing endovascular or surgical treatment options.27
Her hematology team transitioned her polycythemia vera treatment to ruxolitinib, a JAK1-JAK2 inhibitor shown to be superior to standard therapy in controlling hematocrit and symptoms in patients intolerant of hydroxyurea.28,29
TAKE-HOME POINTS
The differential diagnosis for purple toes is broad. A major branch point is the presence or absence of peripheral pulses to rule out critical limb ischemia necessitating urgent evaluation and management.
Recurrent thrombosis in the setting of anticoagulation necessitates further workup.
Patients may have multiple risk factors for thrombosis, which may change optimal anticoagulation management.
The anticoagulation of choice for all patients with APS is warfarin.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2024 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}