


Article Figures & Data
Figures
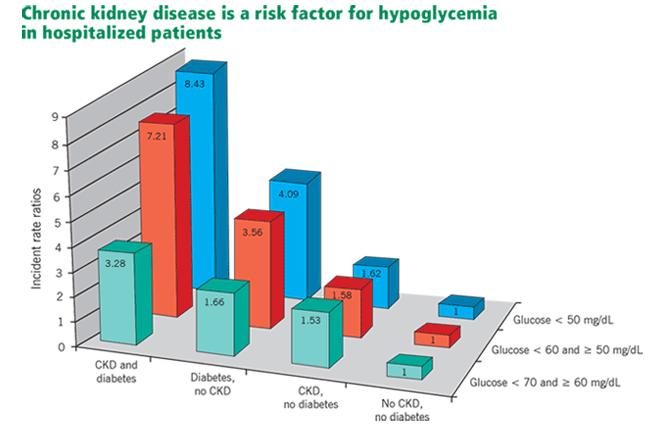
- FIGURE 1
Incidence of hypoglycemic episodes in hospitalized patients with or without chronic kidney disease (CKD) and diabetes in a Veterans Administration study.12 All differences compared with the reference group (no CKD, no diabetes) were statistically significant (P < .0001).
Republished with permission of the American Society of Nephrology. From Moen MF, Zhan M, Hsu VD, et al. Frequency of hypoglycemia and its significance in chronic kidney disease. Clin J Am Soc Nephrol 2009; 4:1121–1127. Copyright 2009. Permission conveyed through Copyright Clearance Center, Inc.

Tables
- TABLE 1
Possible causes of normoglycemia or hypoglycemia in dialysis patients who previously required insulin
Decreased renal clearance of insulin Decreased hepatic clearance of insulin Impaired renal insulin degradation Increased insulin half-life for reasons other than renal or hepatic conditions Decline in renal gluconeogenesis Deficient catecholamine release Other impacts of uremia on glucose homeostasis Diminished food intake because of problems such as anorexia, diabetic gastroparesis Protein-energy wasting (malnutrition-inflammation complex) Loss of body weight and fat mass Comorbid conditions Hypoglycemia during hemodialysis treatments Effects of peritoneal dialysis on glucose metabolism Prescribed medications Imposed dietary restrictions Low hemoglobin A1c owing to confounding by uremia or anemia Kovesdy CP, Park JC, Kalantar-Zadeh K. Glycemic control and burnt-out diabetes in ESRD. Semin Dial 2010; 23:148–156. Copyright John Wiley and Sons, 2010; used with permission.
Insulin Onset of action Peak effect Duration Frequency of administration Glargine 2 hours No peak 24 hours Once daily Detemir 2 hours 3–9 hours 12–24 hours Once or twice daily Neutral protamine 1–2 hours 4–8 hours 12–18 hours Once or twice daily Hagedorn Lispro, glulisine, aspart 5–15 minutes 1–2 hours 4–6 hours Before or after each meal Regular 30 minutes 2–4 hours 6–8 hours With meals or every 6 hours for patients on continuous tube feeding - TABLE 3
Suggested starting doses of basal insulin (glargine or detemir) for hospitalized patients
Type of diabetes Insulin dose (U/kg/day) Normal renal function GFR 10-50 mL/min GFR <10 mL/min Age > 70 Body mass index < 19 kg/m2 Type 1 0.2 0.15 0.1 0.15 0.15 Type 2 0.25 0.15 0.1 0.15 0.15 NOTE: For patients who are eating, give an equivalent amount as short-acting insulin (eg, for a 100-kg patient with a GFR of 30 mL/min, give 15 units basal once per day and 5 units short-acting insulin with each meal).
Drug Mechanism of action Advantages Side effects and disadvantages Use in chronic kidney disease Biguanide metformin Insulin sensitizer
Decreases hepatic glucose productionNo hypoglycemiaa
No weight gainGastrointestinal
Vitamin B12 deficiency
Lactic acidosisContraindicated if serum creatinine > 1.5 mg/dL in men and 1.4 in women in US (in most other countries may use if glomerular filtration rate [GFR] ≥ 30 mL/min) Sulfonylureas glyburide, glipizide, glimepiride Stimulate insulin release
Decrease postprandial glucoseLess expensive Hypoglycemia
Weight gainDue to risk of hypoglycemia, must be used with caution (short-acting glipizide preferred) Meglitinides repaglinide, nateglinide Stimulate insulin release
Decrease postprandial glucoseHypoglycemia
Weight gain
ExpensiveSafer than sulfonylureas Thiazolidinediones pioglitazone Insulin sensitizer in muscle and adipose tissue No hypoglycemiaa Weight gain
Edema
Bone fracturesSafe but can cause fluid retention, limiting its use in chronic kidney disease Alpha-glucosidase inhibitors acarbose, miglitol Slow carbohydrate absorption, decrease postprandial glucose No hypoglycemiaa Gastrointestinal Contraindicated if serum creatinine > 2 mg/dL GLP-1 receptor agonists exenatide, liraglutide, albiglutide Activate GLP-1 receptor
Increase insulin
Decrease glucagon
Decrease gastric emptying, increase satietyWeight loss
No hypoglycemiaaGastrointestinal
Pancreatitis
Medullary thyroid cancer
ExpensiveContraindicated if GFR < 30 mL/min Dipeptidyl peptidase-4 inhibitors sitagliptin, saxagliptin, linagliptin, alogliptin Inhibit breakdown of GLP-1
Increase insulin
Decrease glucagonNo hypoglycemiaa Pancreatitis
ExpensiveSafe
Require dose reduction except linagliptinDopamine agonist bromocriptine Stimulates dopamine receptors No hypoglycemiaa Hypotension Unknown Bile acid sequestrant colesevelam Unknown No hypoglycemiaa Constipation
Increases triglyceridesUnknown SGLT2 inhibitors canagliflozin, dapagliflozin, empagliflozin Inhibit sodium-glucose cotransporter-2 (SGLT2), reducing glucose reabsorption and increasing urinary glucose excretion No hypoglycemiaa Mycotic infections
Urinary tract infectionsContraindicated if GFR < 45 mL/min ↵a No hypoglycemia when used alone, but may cause hypoglycemia when used with insulin or sulfonylureas.




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.