


Article Figures & Data
Figures
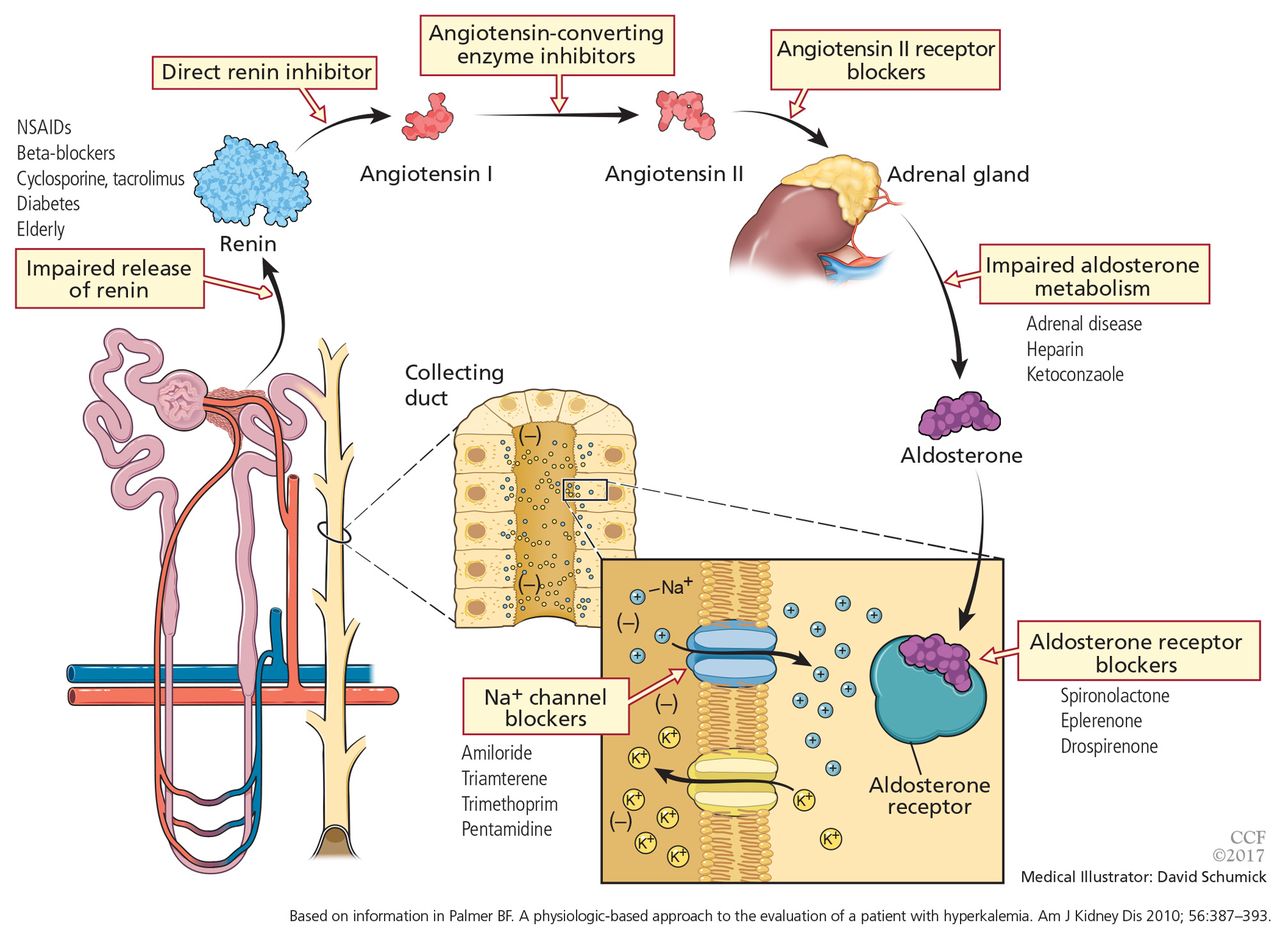
- Figure 1
A number of pharmacologic agents and conditions can interfere with the renin-angiotensin-aldosterone system, altering renal potassium excretion. Reabsorption of sodium in the collecting duct increases the luminal electronegativity, providing a more favorable gradient for potassium secretion. Aldosterone is critical for this reabsorptive process. A number of drugs and conditions interfere with the production of aldosterone and, as a result, reduce renal potassium secretion. In some patients, more than 1 disturbance may be present. NSAIDs = nonsteroidal anti-inflammatory drugs.
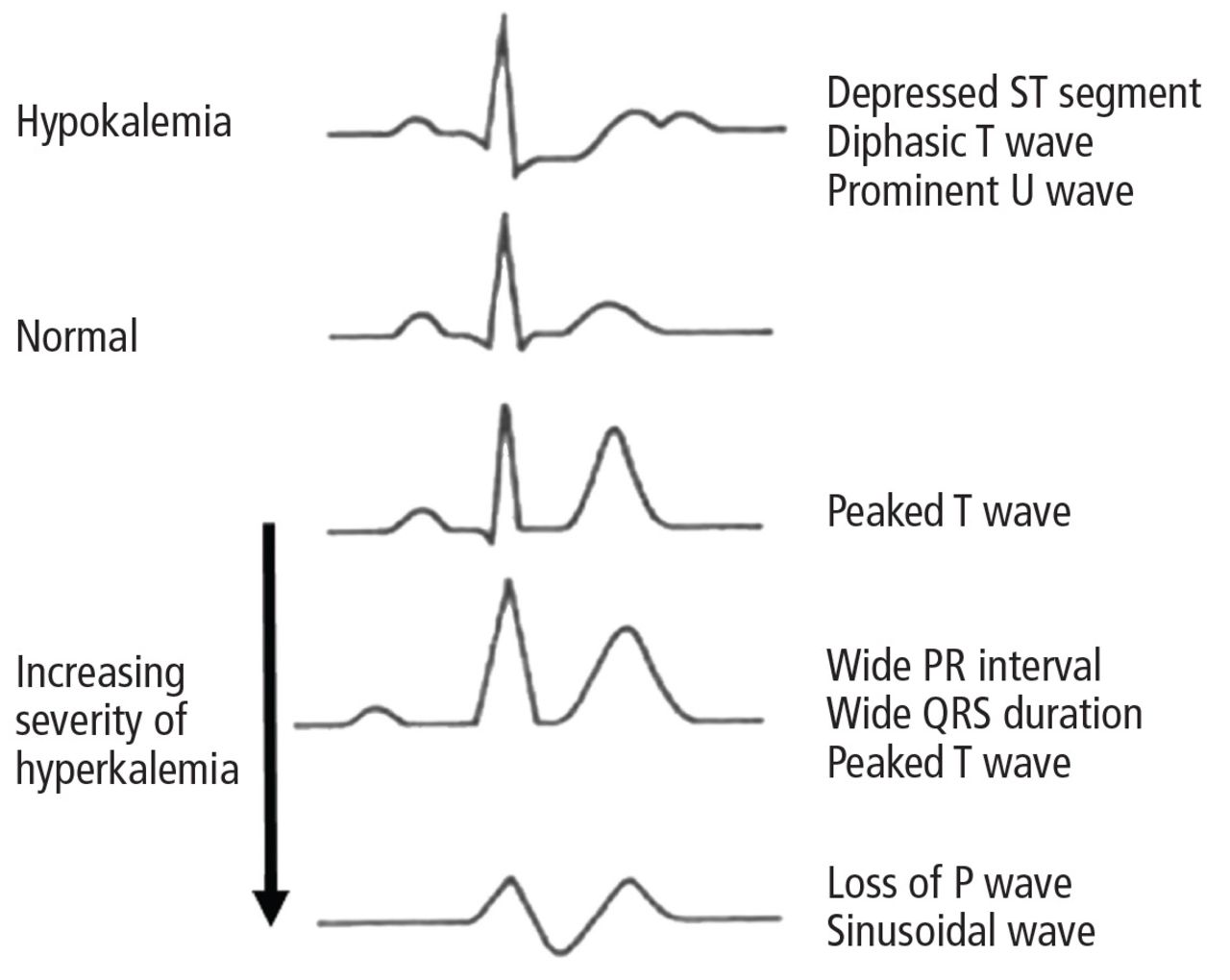
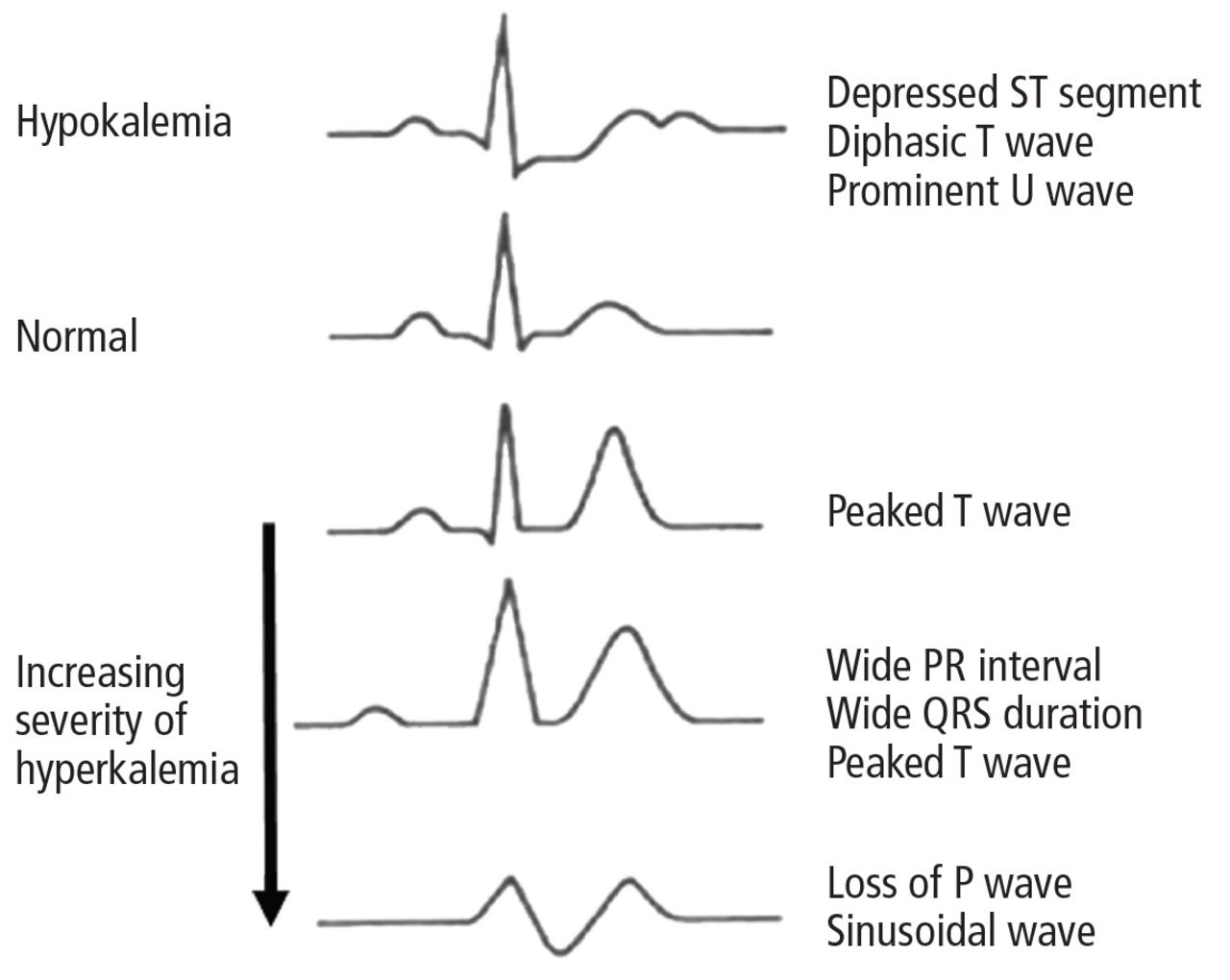
- Figure 2
Electrocardiographic signs of hyperkalemia

Tables
Pseudohyperkalemia Cellular redistribution
Mineral acidosis
Hypertonicity
Insulin deficiency
Beta-blockers (impair cell uptake of potassium)
Alpha adrenergic stimulation
Hyperkalemic periodic paralysis
Cell injuryExcess intake
(almost always in setting of impaired renal potassium excretion)Decreased renal excretion
Decreased distal delivery of sodium (oliguric renal failure)
Mineralocorticoid deficiency
Defect of cortical collecting tubule- TABLE 2
Reducing the risk of hyperkalemia when using renin-angiotensin-aldosterone system blockers
Assess renal function to define overall risk of hyperkalemia Discontinue medications that can impair renal potassium excretion, including herbal preparations and over-the-counter nonsteroidal anti-inflammatory drugs Reduce potassium in diet, avoid salt substitutes containing potassium Ensure effective diuretic therapy (loop diuretics should be used if the estimated glomerular filtration rate is < 30 mLmin/1.73 m2) Correct metabolic acidosis when present Start with low doses of renin-angiotensin-aldosterone system blockers and monitor closely




{kind=link}
{kind=link}