


Article Figures & Data
Figures
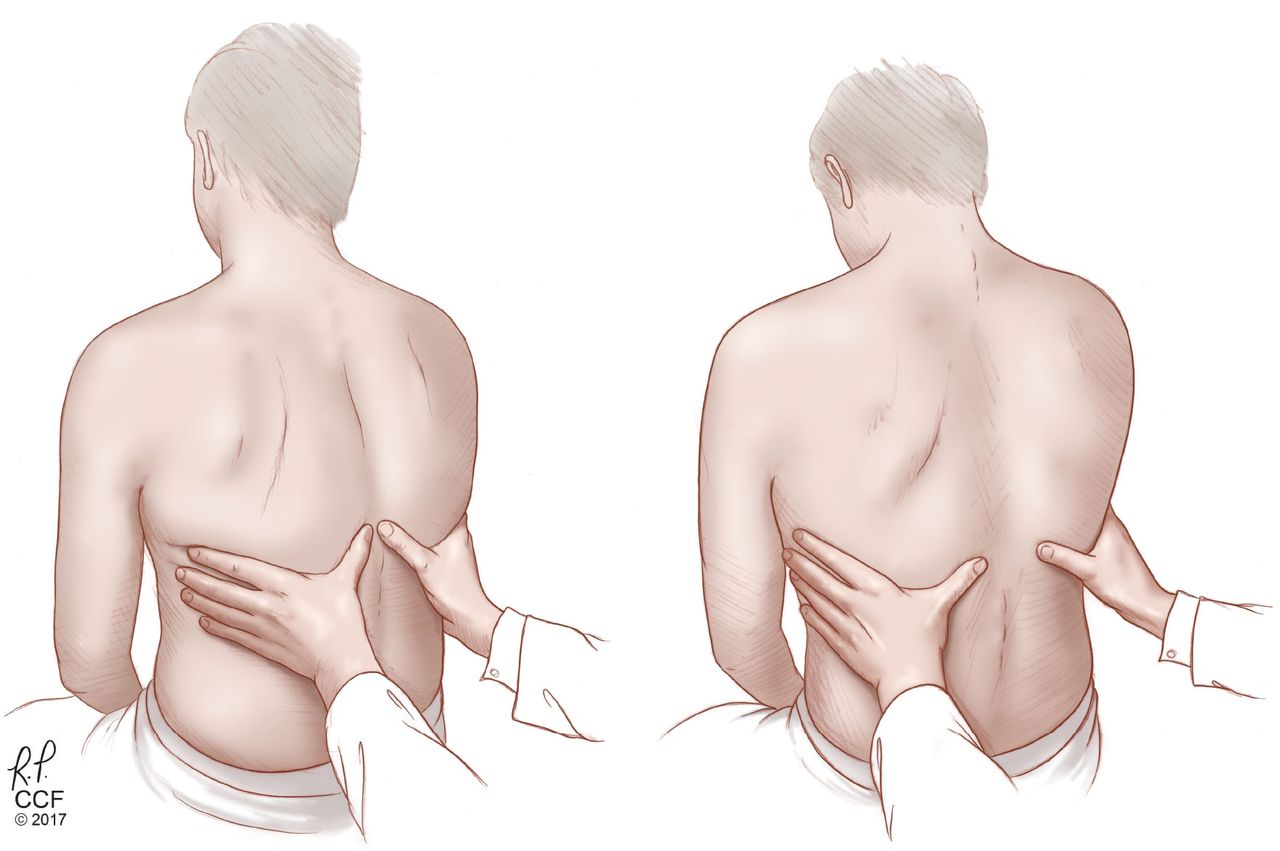
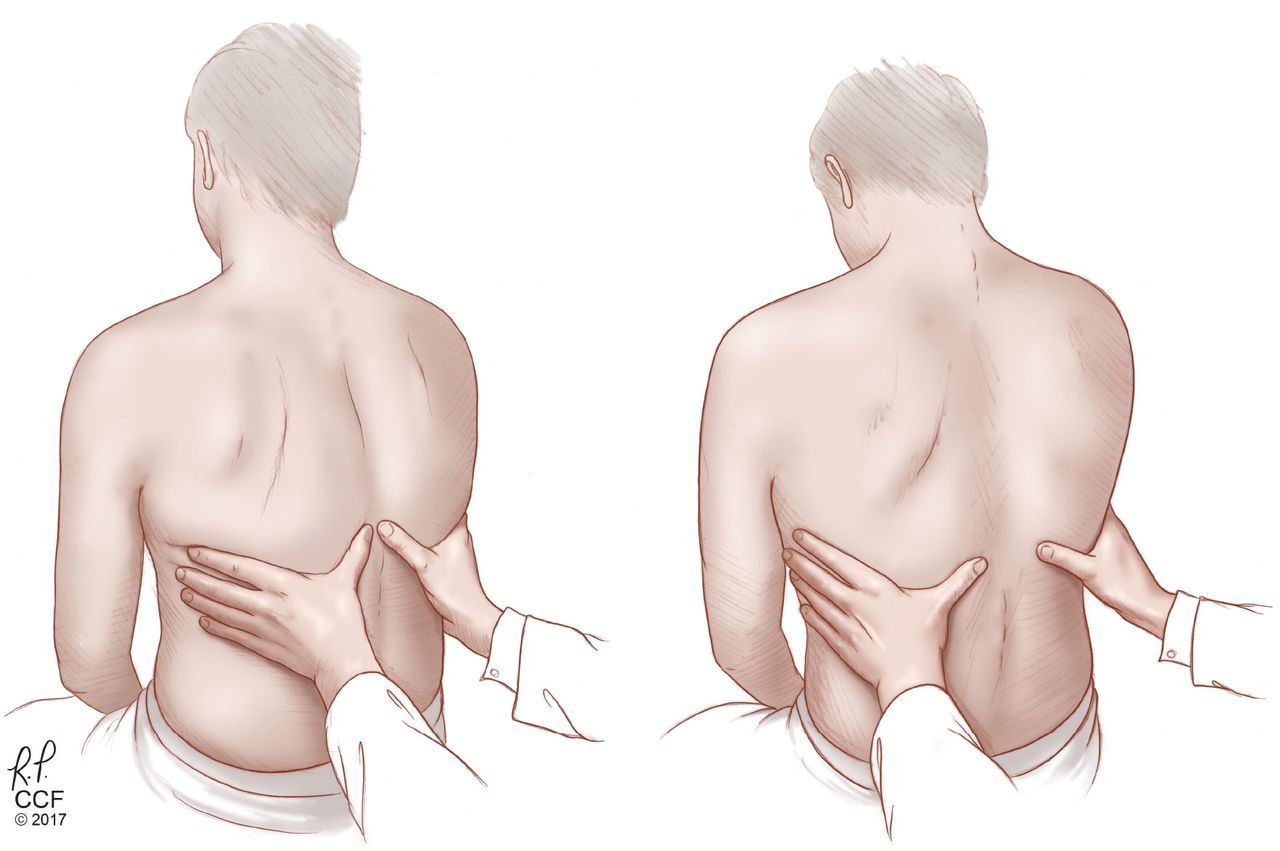
- Figure 1
Checking for asymmetry in chest expansion, a specific but not sensitive sign of pneumonia and of pleural effusion. Left, expiration; right, inspiration.
From Diaz-Guzman E, Budev MM. Accuracy of the physical examination in evaluating pleural effusion. Cleve Clin J Med 2008; 75:297–303.
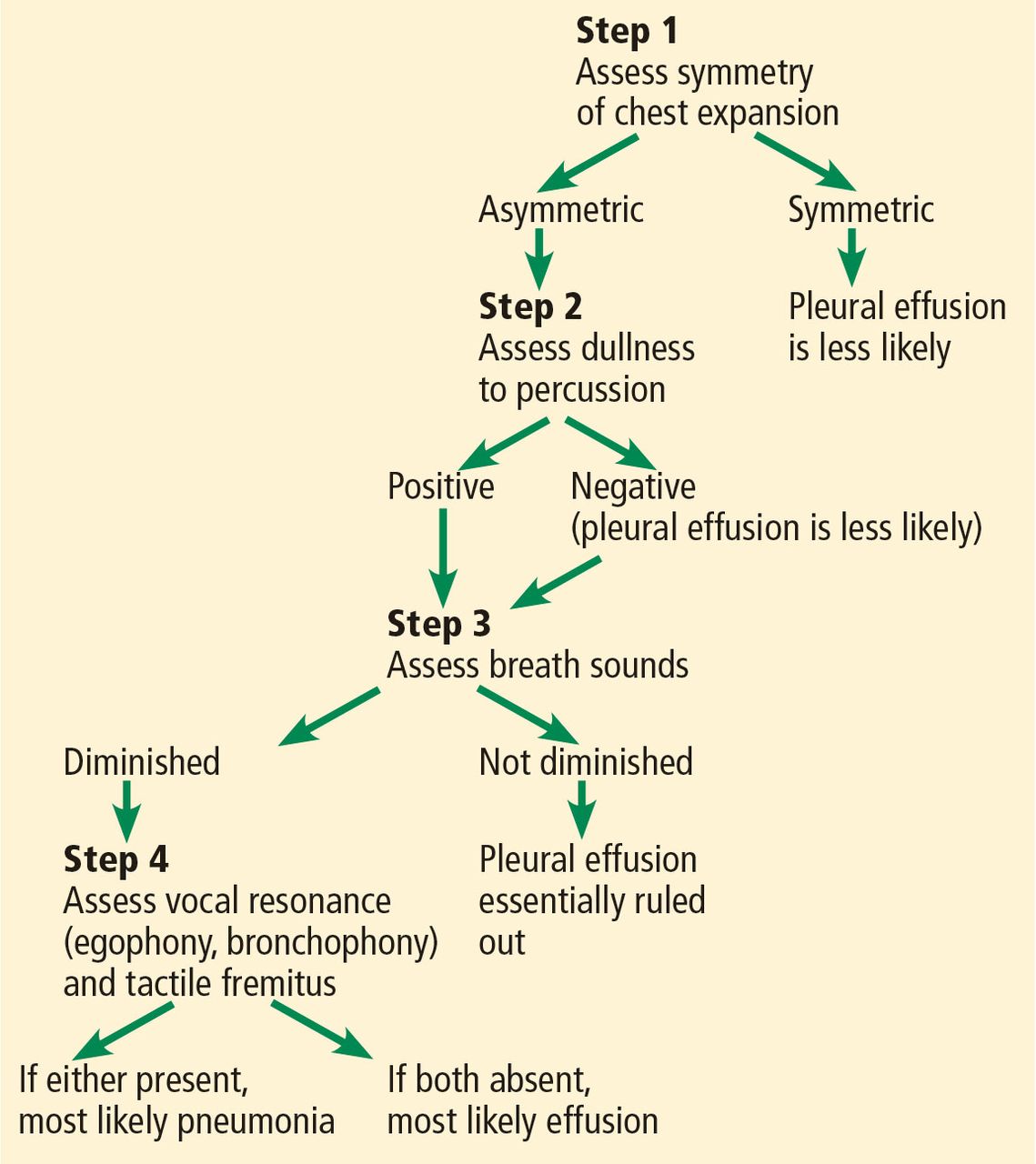
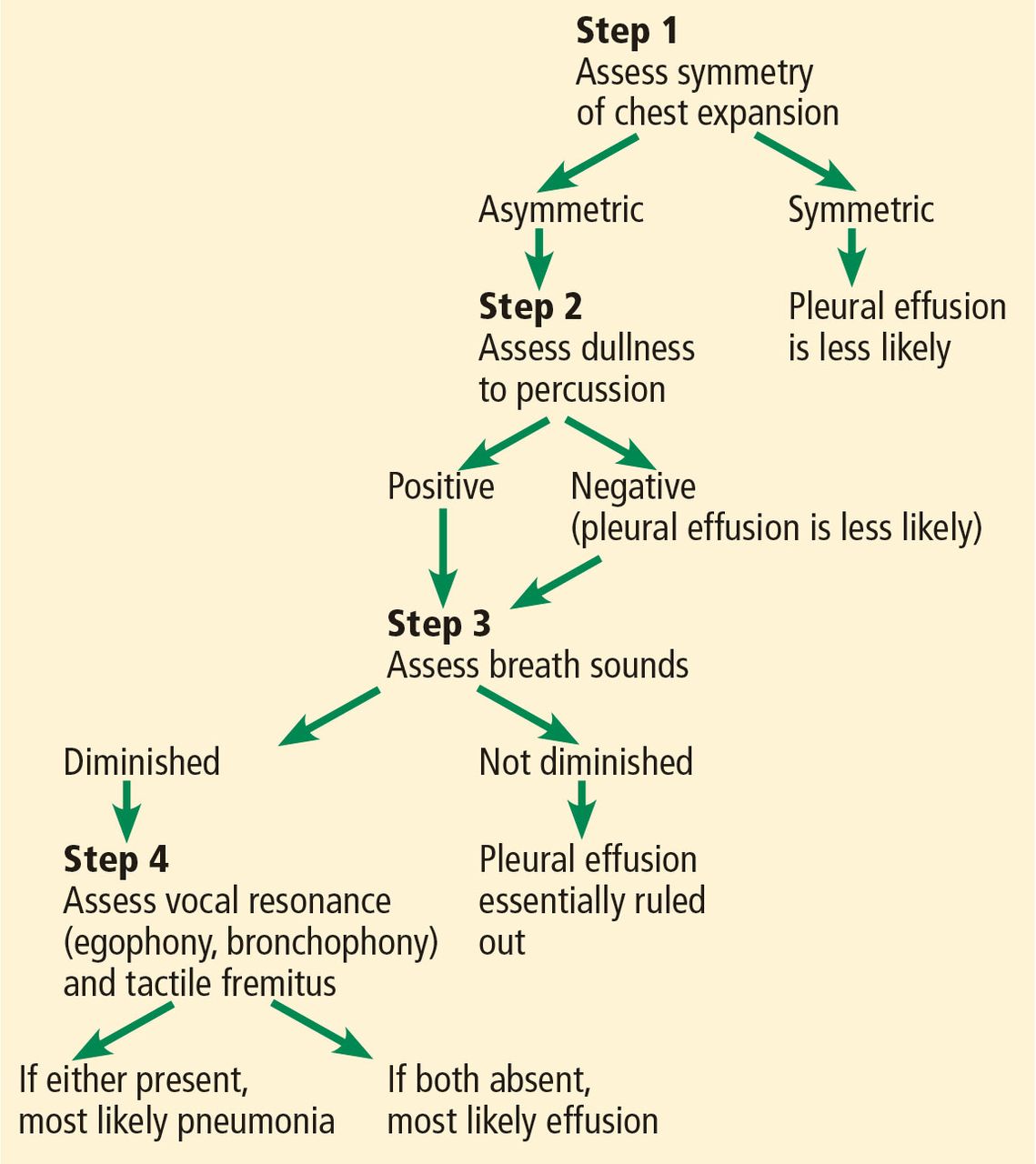
- Figure 2
Algorithmic approach to physical examination for suspected pneumonia vs pleural effusion.
Tables
Likelihood ratio Approximate change in probability 0.1 −45% 0.2 −30% 0.3 −25% 0.4 −20% 0.5 −15% 1 No change 2 +15% 3 +20% 4 +25% 5 +30% 6 +35% 8 +40% 10 +45% Values between 0 and 1 (negative likelihood ratios) decrease the probability of disease; values greater than 1 (positive likelihood ratios) increase the probability of disease.
From McGee S. Simplifying likelihood ratios. J Gen Intern Med 2002; 17:647–650.
Auscultatory breath sound Character Clinical correlation Normal (vesicular) breath sound Soft
Nonmusical
Inspiration/expirationDiminished in hypoventilation, airway narrowing, pleural effusion, pneumothorax, and lung destruction. Tracheal (tubular) breath sound heard at the periphery Hollow
Nonmusical
Inspiration/expirationConsolidation or compressed lung (pneumonia, tumor, atelectasis) Wheeze Musical and high-pitched
Inspiration/expirationUpper airway obstruction
Widespread airflow limitationRhonchi Musical and low-pitched
Inspiration/expirationAirway narrowing by mucous thickening, edema, or bronchospasm Fine crackles Short
Explosive
Nonmusical
Mid to late inspirationHeard in interstitial lung disease, congestive heart failure, fibrosis, pneumoconiosis, pneumonia Coarse crackles Short
Explosive
Nonmusical
Early inspiration
Throughout expirationIndicates intermittent airway opening in chronic obstructive pulmonary disease Stridor Musical
High-pitched
Audible to unaided earUpper airway obstruction
Extrathoracic in inspiration
Intrathoracic in expiration
Fixed lesions biphasicSquawk Short musical wheeze
Accompanying cracklesPneumonia (acutely)
Interstitial lung disease
PneumonitisBased on information in reference 4.
Signs Positive likelihood ratio Negative likelihood ratio Asymmetric chest expansion6 44.1 1.0 Egophony6,10,11 6.8 0.9 Dullness to percussion6,10–12 5.7 0.9 Bronchophony10 3.3 0.9 Crackles6,10–12 3.2 0.7 Diminished breath sounds10–12 2.5 0.7 Sign Positive likelihood ratio Negative likelihood ratio Dullness to percussion13 8.7 0.31 Asymmetric chest expansion14 8.1 0.29 Diminished tactile fremitus14 5.7 0.21 Diminished vocal resonance14 6.5 0.27 Signs Positive likelihood ratio Negative likelihood ratio Jugular venous pressure ≥ 8 cm23,26 9.7 0.3 Jugular venous pressure ≥ 12 cm23,24 10.4 0.1 Abdominojugular reflux28–30 8.0 0.3 Displaced apical impulse31–34 10.3 0.7




{kind=link}
{kind=link}